
記住我


The concept of surgical interventions for lymphedema management dates back several decades. Lymphovenous shunt (LVS) for treatment of lymphedema is based on bypass of lymph fluid from obstructed the lymph vessel to the peripheral vein.1 Shunt usually utilizes larger lymph vessels and veins, which may be performed in more proximal area, such as in the thorax to bridge the thoracic duct to the superior vena cava for the treatment of chylothorax.2 During 1960 to 1970, the LVS started to be applied or studied for surgical treatment of secondary extremity lymphedema.3–5 As the collecting lymph vessels are too small to be anastomosed until 1990s, implantation of the lymph vessels into a relatively large vein or coaptation of the lymph node’s stump on a large vein are used in most LVS operations.
Over time, advancements in microsurgical techniques paved the way for more precise procedures, leading to the development of supermicrosurgical lymphovenous anastomosis (LVA), in which intima-to-intima coaptation of the collecting lymph vessels to the small veins or the venules.5–10 Around 1970, Yamada and O’Brien reported basic studies and clinical cases of LVA, which involved the direct connection of the lymph vessels to adjacent venules or small veins using microsurgical sutures.6 After 1980s, more reports of microvascular LVA emerged,7,8 but still gained little popularity until 2000, Koshima et al9 introduced the concept of supermicrosurgical anastomosis of lymphatic vessels with diameter <0.8 mm and recently, there has been a renewed interest in the surgical treatment of lymphedema. “Supermicrosurgery” means anastomosis is performed in extremely small vessels (0.3-0.8 mm in diameter). These procedures have recently gained momentum as a preferred surgical approach, particularly in patients with early-stage lymphedema, and relatively large numbers of procedures are performed in centers located in Japan, Taiwan, the United States, and European countries.10–12 Subsequent studies and refinements in surgical techniques demonstrated the efficacy and safety of LVA in various types of lymphedema.10,11 The advent of supermicrosurgery, characterized by the use of high-powered microscopes and specialized instruments, further enhanced the precision and success rates of LVA.1 Of the physiological surgical options for the management of lymphedema, LVS or LVA is often preferred as a minimal risk and less invasive option when compared with vascularized lymph node transfer (VLNT).13 Today, LVA is considered a well-established procedure for the treatment of lymphedema.
2. DIFFERENCES BETWEEN OTHER LV SHUNTS AND LVAWhile various surgical techniques have been developed for the treatment of lymphedema, it is essential to differentiate between traditional LVS and LVA due to their distinct characteristics and outcomes.
Traditional LVS involve the creation of direct connections between lymphatic vessels and veins, often using larger ones. These procedures aim to bypass obstructed lymphatic pathways and reroute lymphatic fluid into the venous system at proximal region of limbs. Two types of shunts were primarily performed, the lymph node–saphenous vein (LNSV) and afferent lymphatics–saphenous vein (ie, lymph vessel–saphenous vein [LVSV]).14 LNSV, the idea came to the authors’ minds when they observed lymph oozing freely from the subcortical sinuses of the transected lymph nodes.15 A node is implanted end-to-side into a window in the neighboring vein. For LVS, the incision is made proximally at the inguinocrural area to allow identification of the saphenous vein, or its branching, and the lymphatic collectors. Up to four anastomoses can be confectioned between prenodal lymphatics (afferent lymph vessels) of the crural area and collaterals (termino-terminal), or with the saphenous vein itself (termino-lateral) under stereomicroscopic view (magnification, ×40), respectively.16 Olszewski reported the results of his 45-year, one-surgeon, one-center experience with this technique, which showed 80% to 100% improvement in patients with primary hyperplastic lymphedema and 80% improvement in patients with secondary lymphedema after iliac lymphadenectomy. But this technique is not available for lymphedema of the upper limb or in patients with lower limb lymphedema secondary to inguinal lymphadenectomy.14,17 In addition, compared with LVA, traditional shunt procedures have certain limitations. They typically require larger incisions and involve more complex surgical dissections, increasing the risk of complications such as vessel injury, thrombosis, or graft failure. Because of several reports of postoperative deep venous thrombosis and pulmonary embolism, LVS has been considered contraindication for lymphedema treatment until 1990s when LVA was developed and applied. Another debate is the outcomes of traditional shunts may vary, and the long-term efficacy in reducing lymphedema remains uncertain. Furthermore, they often require some type of compression therapy after the procedure to maintain a reduction in the edema.18 Another modified LVS proposed by Yamamoto is lymphaticovenous implantation (LVI)19. Thinner lymphatics (<0.5 mm in external diameter) were implanted telescopically into a larger cutaneous vein, which is simpler but has the drawback of allowing contact between venous endothelium and lymphatic adventitia and perilymphatic adipose tissue. This contact theoretically increases the risk of thrombus formation at the anastomosis site.19 Ishiura et al,20 compared the postoperative patency of LVA and LVI in a rat model and found that postoperative patency was significantly higher in the LVA group (100%) compared with the LVI group (33.3%). They suggest that LVA may have better postoperative patency than LVI, although intraoperative patency rates were similar between the two techniques.20 Consequently, LVI technique is considered inferior to precise intima-to-intima anastomosis, and may be used as a secondary option when supermicrosurgical anastomosis is not feasible when the lymph vessel is too small for a surgeon.21
Unlike traditional shunt procedures, LVA does not require the use of lymph node grafts or larger vessels, which minimizes the invasiveness of the procedure. The smaller size of the anastomosis enables surgeons to target more lymphatic vessels and perform multiple connections within a single surgical session. This allows for a more comprehensive and precise treatment of lymphatic insufficiency.9 There has been an increased interest in the use of this surgical method as a treatment modality for lymphedema as imaging techniques such as indocyanine green (ICG)-directed lymphography, better operating microscopes and microsurgical instrumentation and sutures have become available and have improved the surgeon’s ability to find lymphatic vessels appropriate for LVA and perform supermicrosurgical anastomosis with vessels as small at 0.1 mm in diameter.22 LVA utilizes distal lymphatic vessels in the extremities, which are less affected by lymphedema and more accessible for bypass. The subcutaneous vein, secondary or tertiary branch from the saphenous vein or cephalic/basilic vein, and the lymph vessel below the superficial fascia are usually utilized for LVA, as they have lower venous pressure and minimize venous backflow. With the advancements in supermicrosurgery, LVA has become a consistently and successfully performed procedure, enabling effective treatment of lymphedema.23,24
Another significant advantage of LVA is its ability to be performed under local anesthesia. The minimally invasive nature of the procedure, coupled with the use of supermicrosurgical techniques, reduces postoperative morbidity and enables faster recovery for patients.25,26 Additionally, the success rates of LVA have been reported to be favorable, with studies showing significant reductions in limb volume, improved lymphatic function, and alleviation of lymphedema-related symptoms.27–29 Initially, it is noted that LVA is most suitable for patients with localized or early-stage lymphedema, where functional lymphatic vessels are still present.10,30–32 In cases of more advanced lymphedema or extensive fibrosis, alternative surgical options, such as lymph node transfer or vascularized lymph node flap, may be considered. But recently, Cha et al,33 found that LVA can also effectively reduce the volume of the limb and improve subjective symptoms in patients with advanced stage lymphedema of the lower extremity.
The differences between traditional LV shunt and LVA highlight the evolution and refinement of microsurgical techniques in lymphedema management. LVA offers a less invasive, more targeted approach with potentially better outcomes for eligible patients.
3. IMMEDIATE LYMPHATIC RECONSTRUCTIONLVA has become increasingly popular as a therapy for well-established secondary lymphedema. However, it is worth noting that the onset of cancer-related lymphedema can vary significantly, occurring anywhere from 3 to 6 months to over 1.5 to 5 years after diagnosis and treatment.34–36 Thus, a cutoff 6 months is usually adopted for differentiation of acute transient swelling after surgery/radiotherapy/chemotherapy.37
Recently, there is a growing emphasis on immediate lymphatic reconstruction (ILR) at the axillary surgical site for patients immediately following axillary lymph node dissection. This concept, introduced by Boccardo and Campisi in 200938, is now commonly referred to as LYMPHA, which stands for Lymphatic Microsurgical Preventive Healing Approach.38 LYMPHA is so named because it involves reconstructing the lymphatic system near the proximal end of the limb, close to the veins, with the aim of preventing the development of lymphedema following lymph node dissection. Given the larger vein diameter near the proximal end of the limb, LVI or end-to-side LVA procedure is considered more suitable.39
Recent clinical studies have increasingly demonstrated the preventive effectiveness of LYMPHA against upper or lower limb lymphedema in cancer patients.40 However, a blanket application of ILR to all cancer patients undergoing lymph node dissection may lead to unnecessary surgery for individuals who would not have developed lymphedema.28,41 In practice, a more thorough comprehension of the risk factors associated with postoperative lymphedema would enhance the effectiveness of LYMPHA.42–44 Additionally, utilizing techniques like reverse mapping during axillary/pelvic/groin lymph node dissection to evaluate lymphatic duct disruption or leakage can aid in determining the necessity of ILR. However, the overall therapeutic advantages of this approach warrant further investigation through comprehensive, large-scale studies.41
4. COMPARISON BETWEEN LVA AND VLNTLVA and VLNT are two surgical techniques used to address lymphedema by providing physiological reconstruction of the lymphatic system.1 LVA creates connections between lymphatic vessels and veins to establish an alternative drainage route, primarily for early-stage lymphedema. VLNT transplants healthy lymph nodes and surrounding tissue, recommended for advanced lymphedema or when LVA is ineffective. It offers drainage pathways, immune function, and lymphangiogenesis, potentially providing more comprehensive relief. However, it is a more complex and invasive procedure with longer recovery times and a higher risk of complications.2,3
Comparing outcomes, LVA may offer effective and safe outcome in early-stage lymphedema,4,5 while VLNT can provide more extensive and lasting results, especially in advanced cases.6
The choice between LVA and VLNT depends on the patient’s specific condition, and careful consideration by a specialized medical team is essential to determine the most suitable treatment approach.7,45
Recently, there have been reports of combining LVA with VLNT to achieve more comprehensive lymphedema management.8
5. SEVERITY STAGING AND INDICATION OF LVACurrently, the severity of lymphedema is typically assessed based on clinical presentation, limb volume measurements, and functional impairment. Staging systems, whether according to clinical symptoms or image studies for lymphedema are important in defining the severity of the problem, determining treatment modalities, potentially predicting outcomes, and documenting response to therapy.46 The ideal staging system should be comprehensive, reproducible, and have correlation between clinical, imaging, and functional assessments.47 For clinical staging, International Society of Lymphology (ISL) staging (derived from original staging system described by Campisi et al47,48) is simple and categorizes lymphedema into four levels of clinical severity: Stage 0: Subclinical lymphedema with no visible swelling. Stage I: Early-stage lymphedema with reversible swelling. Stage II: Moderate lymphedema with minimal pitting. Stage III: Advanced lymphedema with non-pitting fibrosis.49 But clinical staging could not provide details in anatomic abnormalities or location of lymphatic ducts and hence is not helpful in making decision for corresponding treatment. However, for performing LVA, more information about the status of subdermal lymphatic status is crucial for proper patient selection to achieve optimal outcomes in the treatment of lymphedema. In contrast, image studies not only can reveal anastomotic structure and composition according to severity but also delineate status of lymphatic ducts and lymph nodes. Now, the image modalities used to evaluate edema status include ultrasound, computed tomograph (CT), magnetic resonance imaging (MRI) and particularly, there are image tools that could provide information about location of lymphatic duct and flow status, such as lymphscintigraphy, ICG lymphography, or MR lymphangiography. In addition, many staging system of limb lymphedema based on these image findings could better provide the information for pre-, intra-, and postoperative application in LVA.46,50–52 Due to their high reliability, both lymphoscintigraphy and ICG lymphography (ICG-L) have emerged as the gold standard diagnostic methods for lymphedema.53 However, whether image staging is directly correlated with clinical staging and pathophysiological status is controversial.47,54,55 To date, no imaging technique has been widely adopted for the staging of lymphedema.
Lymphoscintigraphy revealed distribution of lymphatic obstruction, delay in lymphatic transport, presence or absence of regional lymph nodes, formation of collateral lymphatics and/or the presence of dermal backflow (DB).56–58 Many staging systems based on lymphoscintigraphy findings have been proposed. Theses staging/scoring systems cover most of the lymphoscintigraphy findings in lymphedema, but are not integrated into clinical practice due to complexity and not clear relationship with the severity of the disease and treatment response.54,58–63
ICG-L is captured by the use of a near-infrared camera device to detect lymphatic status. The major staging systems of ICG-L are DB stage, MD Anderson (MDA) classification, and ICG stage.64 arm dermal backflow (ADB) scale mainly categorized ICG-L findings into linear and abnormal DB pattern, including splash, stardust, and diffuse. The severity of lymphedema from ICG-L are classified into 0 to 5 in the extremity and 0 to 4 for the genital area. LVA is indicated in the lymphedema patient with stage 2 to 5.51 Recently, Imai et al,65 studied 35 patients with lower extremity lymphedema and found a strong correlation between lymphoscintigraphy and ICG-L, but there was no correlation with any other lymphatic image or clinical severity. MDA classification also has 0 to 5 stage to grade the degree of lymphedema severity. In their study, Jørgensen et al64 examined the association between the ADB and MDA scales and the clinical presentation of breast cancer-related lymphedema (BCRL). The findings of their research indicated that staging BCRL using ICG-L is a dependable and secure method that offers distinctive disease-related information that cannot be obtained solely through clinical measurements. Although some reported superiority of a staging system compared to the other, no consensus is established on which staging system is the most suitable for lymphedema evaluation.64
Magnetic resonance lymphangiography (MRL) offers greater sensitivity in imaging and is capable of detecting subtle changes at an earlier stage compared with lymphoscintigraphy. Unlike ICG-L, MRL enables the visualization of both superficial and deep lymphatic vessels, providing a more precise depiction of edema within the limb beyond superficial DB patterns. Additionally, MRL can be utilized to calculate transport times, accurately measure lymphatic vessel diameter, and assess alterations in lymph node basins. However, its practical application in real-time surgical procedures is currently limited.66
There is currently no widely accepted consensus regarding the indications for lymphovenous procedures. The existing studies on this topic are primarily retrospective and yield varying results. However, most experts concur that LVA should be considered for patients who have not responded to conservative treatments or experience recurring cellulitis or lymphangitis.10,21
6. BASIC ANATOMY AND PREOPERATIVE MAPPINGUnderstanding the lymphatic anatomy and conducting preoperative mapping are essential steps in performing successful LVA procedures. A thorough knowledge of the lymphatic system helps identify suitable donor and recipient vessels and improves the overall surgical planning. Preoperative mapping enables surgeons to identify suitable donor lymphatic vessels and nearby recipient veins for the anastomosis. It helps guide the surgical approach, determine the number of anastomoses required, and optimize the overall success of the procedure.17
The lymphatic system is a complex network of vessels and nodes responsible for fluid balance, immune function, and lipid absorption. Lymphatic vessels collect excess interstitial fluid, known as lymph, from the tissues and transport it back into the venous circulation. The major lymphatic vessels include the initial lymphatics, precollectors, collectors, and main lymphatic trunks.67,68
The lymphatic vessels are composed of thin endothelial channels that can vary in diameter and complexity. They are often located within the subcutaneous tissue, accompanying blood vessels and nerves. The lymphatic vessels drain into lymph nodes, which filter and process the lymph before it returns to the venous circulation.67
Several techniques can be employed to aid in preoperative lymphatic mapping, including ICG-L and ultrasound.69–72 While lymphoscintigraphy and ICG fluorescent lymphography serve as the standard diagnostic tools for lymphedema, each has its inherent limitations in lymphatic mapping. Alternative imaging methods are required for accurate vessel identification.72–74 When ICG-L shows linear images, ultrasonography can be used to analyze marked collectors’ diameter, depth, and quality. In moderate to severe lymphedema cases with only DB patterns, ultrasonography directly searches large lymphatic channels, leading to impressive surgical outcomes. Ultrasonography helps locate recipient venules for precise bypassing of the selected lymphatic channel.72
In a proof-of-concept study, researchers explored the use of Multispectral Optoacoustic Tomography (MSOT) as a noninvasive tool for lymphatic imaging in lymphatic reconstructive surgery. They compared MSOT with conventional ICG-L in seven lymphedema patients. MSOT accurately visualized lymph vessels, including areas affected by DB, correlating well with macroscopic appearance. MSOT shows promise as a preoperative mapping tool for LVA site selection in lymphedema patients.74
Pons et al75 presents a protocol for lymphaticovenous anastomosis (LVA) preoperative planning in lymphedema patients using ICG-L and MRL. The combination of these noninvasive techniques accurately identified functional lymphatic vessels, aiding successful LVA surgery in 91.4% of cases, and represents a significant advancement in lymphedema management.
Furthermore, the concept of lymphosome is also important for selection of appropriate incision site and avoid compromising remaining lymphatic pathway. In upper extremity, for example, Suami’s research revealed that lymphatic pathways from the hand and forearm generally flow to the axillary region’s sentinel lymph node. The lateral upper arm pathway often bypasses the axillary nodes, while the medial upper arm pathway consistently drains into the axillary basin.76,77 Understanding these pathways has important clinical implications, as they can act as backup routes in case of injury. The knowledge of the location of the functional lymphatic pathways also could inform surgeons of anatomic regions where extirpative procedures may be at high risk of causing lymphedema69
7. SURGICAL PROCEDURES (DISSECTION/PREPARATION OF LYMPH/VEIN, ANASTOMOSIS CONFIGURATION/CONSIDERATION, PATENCY EVALUATION)Supermicrosurgery offers solutions for lymphedema, finger amputations, and minimally invasive reconstruction using perforator-to-perforator technique, enabling targeted customization.1 Supermicrosurgery LVA is defined as microsurgery in less than 0.8 mm vessels and involves intima-to-intima coaptation between lymphatic vessel and vein.9,78 Expertise is required for supermicrosurgery due to its advanced technique and learning curve. It builds upon microsurgery principles with enhanced tools, planning, technique, and aftercare.9
Identification of functional lymphatic vessels and suitable recipient veins are both crucial factors for a successful LVA.79,80 Lymphatic vessels are delicate structures that require careful handling during dissection and preparation. Various image techniques can be employed to visualize lymphatic vessels. These imaging modalities assist in identifying lymphatic vessels and mapping their course.79 Once identified, the key to safely and quickly isolation of lymphatic vessels for LVA is differentiation of fat lobules, superficial fascial, and interlobular septum meticulous.81 Special attention is given to avoid unnecessary trauma or damage to the lymphatic system.82,83 Using intraoperative microscopic ICG-L, navigational lymphatic supermicrosurgery enables early identification and dissection of lymphatic vessels, enhancing the success of lymphaticovenular anastomosis procedures.84
The identification and dissection of a suitable adjacent reflux-free recipient vein is also crucial for successful anastomoses.71,85–89 Surgeons typically utilize magnification devices, such as surgical microscopes or loupe magnifiers, to aid in vein identification.90 Commonly used veins for anastomosis include the vena comitans of the superficial veins and small venules in the vicinity of the lymphatic vessels. Careful dissection and isolation of the vein are performed to ensure adequate exposure and a healthy vessel for anastomosis.91
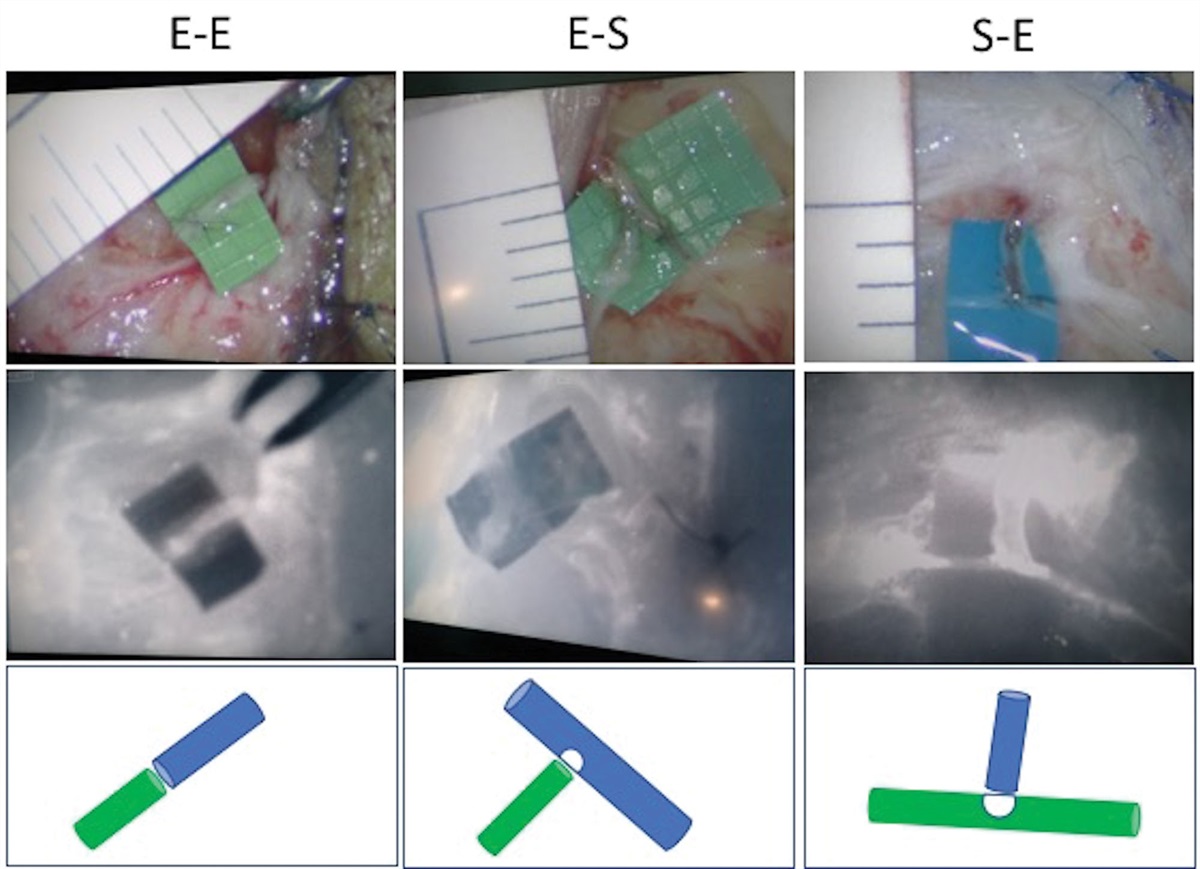
The configuration of the LVA is a critical aspect of the procedure. Surgeons have several options for the configuration, including end-to-end, side-to-end, end-to-side, and side-to-side anastomoses (Fig. 1 for end-to-end, side-to-end, end-to-side and Fig. 2 for side-to-side anastomosis).11,25,31,92–94 The main determining factors for proper anastomotic configuration selection relies on the size and the comparative discrepancy between the lymphatic vessel and recipient vein.95
 Fig. 1:
Fig. 1: The LVA configurations, arranged from left to right as end-to-end, end-to-side, and side-to-end. The first row shows images in bright light, the second row presents the ICG lymphography view, and the third row provides corresponding illustrations for clarity. ICG = indocyanine green; LVA = lymphovenous anastomosis.
 Fig. 2: The image of the side-to-side LVA is sourced from the study conducted by Yamamoto et al.93 LVA = lymphovenous anastomosis.
Fig. 2: The image of the side-to-side LVA is sourced from the study conducted by Yamamoto et al.93 LVA = lymphovenous anastomosis.To achieve a favorable antegrade flow of lymph into the vein, it is advisable to select a less sclerotic lymphatic duct with a larger diameter and a recipient vein with a smaller diameter for the anastomosis.96 Various animal studies evaluated long-term anastomosis patency in LVA, with 80% using end-to-side and 47% using end-to-end techniques, within up to 5 months of follow-up.17 But these studies involved small sample sizes and acute, not chronic, lymphedema models.97 End-to-end anastomosis involves the direct connection of a lymphatic vessel to a venous vessel. This configuration allows for a more straight forward flow of lymphatic fluid into the venous system. It is typically preferred when there is a suitable size match between the lymphatic and venous vessels.81 But when there is a significant gap between a lymph vessel and a recipient vein, end-to-end lymphaticovenular anastomosis can be difficult and side-to-end anastomosis is impossible, end-to-side can be an alternative method. End-to-side anastomosis involves connecting the lymphatic vessel to the side of a venous vessel. This configuration allows for the diversion of lymphatic fluid into the venous system without disrupting the venous flow. It is commonly used when there is a size discrepancy between the lymphatic and venous vessels. In performing end-to-side anastomosis, Yang et al,91 stated that supplementary retrograde anastomoses is discouraged since it may lead to inferior post-LVA outcome compared to antegrade-only anastomoses. Side-to-end anastomosis involves connecting the venule to the side of a lymphatic vessel. This configuration allows for the drainage of both antegrade and retrograde lymphatic flow into venous system.98 In a study, side-to-end and end-to-end LVA effectively improved early-grade extremity lymphedema. Side-to-end had the advantage of greater efficacy in lymph drainage, requiring just one anastomosis and eliminating the need for compression garments (CGs).32,33,97 Another study showed that both end-to-end and side-to-end lymphovenous anastomoses effectively reduced volume, but side-to-end showed significantly better results in advanced-phase (stage II late and stage III) lymphedema, while no difference was observed in early-phase cases.99 But side-to-end is not suggested under the presence of venous reflux due to increasing risk of thrombosis.79 Side-to-side anastomosis involves connecting a lymphatic vessel to a venous vessel by creating a communication between them. This configuration provides an alternative route for lymphatic drainage into the venous system. It is particularly useful when the lymphatic vessels are too small to directly anastomose with a venous vessel.
Assessing the patency of the LVA is crucial for determining the success of the procedure. Various methods can be employed to evaluate the patency of the anastomosis such as ICG-L, Doppler ultrasound and contrast-enhanced lymphangiography.100 These patency evaluation techniques assist surgeons in determining the functionality and effectiveness of the LVA, enabling them to make any necessary adjustments or interventions. Recent review showed that an increased number of anastomoses between the lymphatic ducts and veins did not seem to improve the effectiveness of LVA.93
Briefly, the surgical procedures involved in supermicrosurgical LVA encompass meticulous dissection and preparation of veins and lymphatics, consideration of anastomosis configuration based on patient anatomy, and evaluation of anastomotic patency. By mastering these procedures, surgeons can enhance the success rates of lymphedema treatment and improve patient outcomes.
8. POSTOPERATIVE MANAGEMENTThe success of LVA depends on both the surgical procedure and postoperative management. Compression therapy is a crucial aspect of postoperative care, aimed at reducing swelling, promoting lymphatic drainage, and sustaining the newly created lymphovenous anastomoses. Rodriguez et al used Grade III CGs or elastic bandages for enhanced lymphovenous gradient via anastomosis, encouraging ambulation and using CGs full-time for 2 weeks, then at daytime. He suggested CGs were maintained for at least 1 years after surgery.79 Another protocol involved a 35 to 40 mmHg compression bandage, with patients receiving guidance and encouraged to continue for 6 months.33
Considering diminishing anastomosis patency and potential coagulation tendencies, Aljindan and Cheng et al implemented a non-garment compression strategy post-surgery. Patients rested for 3 days for endothelial healing, then experienced a 2-week rehabilitation involving manual drainage and controlled limb use, without anticoagulants.97
While the current literature lacks uniformity in postoperative LVA, the majority of approaches include a perioperative management strategy that involves prophylactic antibiotics, elevating the affected limb during the night and hospital stay, and utilizing compression therapy for a duration of 4 weeks post-surgery for a period of 6 months.
9. OVERVIEW OF OUTCOMES IN LVA FOR LIMB LYMPHEDEMARegarding the assessment of LVA outcomes, it can be roughly categorized into objective and subjective evaluations. However, it should be noted when explaining the following that the number of patients used in each study, whether it is upper or lower limb, and the assessment and measurement methods varied significantly, leading to a high degree of heterogeneity. Consequently, the interpretation of the results may be subject to bias.29
Nevertheless, overall, objective assessments are typically presented using limb circumference measurements, volume measurements, and volume differentials. Another commonly presented objective assessment is the frequency of cellulitis occurrences before and after surgery. Subjective assessments often include symptom relief and/or validated quality of life measures, as well as the duration of compression therapy usage.30,31
In terms of measurements around the limbs, the results vary widely, but most studies show significant improvements. Only a very small number of cases demonstrate no improvement post-surgery. In early-stage (stage 1-2) patients, the proportion of those who see improvements after LVA is higher than in cases of advanced lymphedema. In the majority of studies, the frequency of cellulitis occurrences post-surgery also decreases, and over half of the patients report an improvement in their quality of life. Most patients reduce their use of CGs post-surgery, with approximately 30% to 100% of patients being able to discontinue compression therapy.97 The likelihood of complications with the LVA procedure is also very low.29
10. PERSPECTIVESSupermicrosurgical LVA, evolving since the last century, has emerged as a pivotal domain within modern microsurgery. This technique plays a crucial role in treating lymphedema disorders. Recent literature has explored clinical imaging, surgical techniques, postoperative care, and efficacy. LVA was found to lead to objective reductions in limb circumference and subjective improvements in the quality of life for both upper extremity and lower extremity lymphedema. Additionally, there was a notable decrease in the frequency of cellulitis episodes and an increased likelihood of discontinuing compression therapy.
This review compiles recent studies in these facets for readers’ quick understanding. Ongoing research in the field continues to harness the revolutionary approach of supermicrosurgery, such as LYMPHA or ILR, which enables intricate operations on minute lymphatic vessels, facilitating lymphatic system restoration, which offering safer and more effective treatments.
REFERENCES 1. Hong JP, Song S, Suh HSP. Supermicrosurgery: principles and applications. J Surg Oncol. 2018;188:832–9. 2. Miller TJ, Gilstrap JN, Maeda K, Rockson S, Nguyen DH. Correction of complete thoracic duct obstruction with lymphovenous bypass: a case report. Microsurgery. 2019;39:255–8. 3. Nielubowicz J, Olszewski W. Surgical lymphaticovenous shunts in patients with secondary lymphoedema. Br J Surg. 1968;55:440–2. 4. Laine JB, Howard JM. Experimental lymphatico-venous anastomosis. Surg Forum. 1963;14:111–2. 5. Yamada Y. The studies on lymphatic venous anastomosis in lymphedema. Nagoya J Med Sci. 1969;32:1–21. 6. O’Brien BM, Sykes PJ, Threlfall GN, Browning FS. Microlymphaticovenous anastomoses for obstructive lymphedema. Plast Reconstr Surg. 1977;60:197–211. 7. Gong Kang H, Ru Qi H, Zong Zhao L, Yao Liang S, Tie De L, Gong Ping P. Microlymphaticovenous anastomosis in the treatment of lower limb obstructive lymphedema: analysis of 91 cases. Plast Reconstr Surg. 1985;76:671–7. 8. O’Brien BM, Mellow CG, Khazanchi RK, Dvir E, Kumar V, Pederson WC. Long-term results after microlymphaticovenous anastomoses for the treatment of obstructive lymphedema. Plast Reconstr Surg. 1990;85:562–72. 9. Koshima I, Inagawa K, Urushibara K, Moriguchi T. Supermicrosurgical lymphaticovenular anastomosis for the treatment of lymphedema in the upper extremities. J Reconstr Microsurg. 2000;16:437–42. 10. Chang DW. Lymphaticovenular bypass for lymphedema management in breast cancer patients: a prospective study. Plast Reconstr Surg. 2010;126:752–8. 11. Yamamoto T, Koshima I, Yoshimatsu H, Narushima M, Miahara M, Iida T. Simultaneous multi-site lymphaticovenular anastomoses for primary lower extremity and genital lymphoedema complicated with severe lymphorrhea. J Plast Reconstr Aesthet Surg. 2011;64:812–5. 12. Campisi C, Bellini C, Campisi C, Accogli S, Bonioli E, Boccardo F. Microsurgery for lymphedema: clinical research and long-term results. Microsurgery. 2010;30:256–60. 13. Garza RM, Chang DW. Lymphovenous bypass for the treatment of lymphedema. J Surg Oncol. 2018;118:743–9. 14. Olszewski W. Lymphovenous microsurgical shunts in treatment of lymphedema of lower limbs: a 45-year experience of one surgeon/one center. Eur J Vasc Endovasc Surg. 2013;45:282–90. 15. Olszewski W. The treatment of lymphedema of the extremities with microsurgical lympho-venous anastomoses. Int Angiol. 1988;7:312–21. 16. Mukenge S, Negrini D, Alfieri O. Secondary lymphedema: clinical interdisciplinary tricks to overcome an intriguing disease. Biology. 2023;12:646. 17. Yamamoto T, Yamamoto N, Kageyama T, Sakai H, Fuse Y, Tsuihiji K, et al. Technical pearls in lymphatic supermicrosurgery. Glob Health Med. 2020;2:29–32. 18. Foldi M. Editorial treatment of lymphedema. Lymphology. 1994;27:1–5. 19. Yamamoto Y, Horiuchi K, Sasaki S, Sekido M, Furukawa H, Oyama A, et al. Follow-up study of upper limb lymphedema patients treated by microsurgical lymphaticovenous implantation (MLVI) combined with compression therapy. Microsurgery. 2003;23:21–6. 20. Ishiura R, Yamamoto T, Saito T, Mito D, Iida T. Comparison of lymphovenous shunt methods in a rat model: supermicrosurgical lymphaticovenular anastomosis versus microsurgical lymphaticovenous implantation. Plast Reconstr Surg. 2017;139:1407–13. 21. Demirtas Y, Ozturk N, Yapici O, Topalan M. Topalan, supermicrosurgical lymphaticovenular anastomosis and lymphaticovenous implantation for treatment of unilateral lower extremity lymphedema. Microsurgery. 2009;29:609–18. 22. Garza R, Skoracki R, Hock K, Povoski SP. A comprehensive overview on the surgical management of secondary lymphedema of the upper and lower extremities related to prior oncologic therapies. BMC Cancer. 2017;17:1–18. 23. Park JE, Chang DW. Advances and innovations in microsurgery. Plast Reconstr Surg. 2016;138:915e–24e. 24. Patel KM, Manrique O, Sosin M, Hashmi MA, Poysophon P, Henderson R. Lymphatic mapping and lymphedema surgery in the breast cancer patient. Gland Surg. 2015;4:244–56. 25. Yamamoto T, Narushima M, Kikuchi K, Yoshimatsu H, Todokoro T, Mihara M, et al. Lambda-shaped anastomosis with intravascular stenting method for safe and effective lymphaticovenular anastomosis. Plast Reconstr Surg. 2011;127:1987–92. 26. Narushima M, Mihara M, Yamamoto Y, Iida T, Koshima I, Mundinger GS. The intravascular stenting method for treatment of extremity lymphedema with multiconfiguration lymphaticovenous anastomoses. Plast Reconstr Surg. 2010;125:935–43. 27. Yamamoto T, Yamamoto N, Kageyama T, Sakai H, Fuse Y, Tsuihiji K, et al. Supermicrosurgery for oncologic reconstructions. Glob Health Med. 2020;2:18–23. 28.
留言 (0)