
記住我


Venous thromboembolism (VTE), including symptomatic deep vein thrombosis (DVT) and pulmonary embolism (PE), is one of the common and serious complications after elective total knee arthroplasty (TKA) and total hip arthroplasty (THA) procedures.1–4 The recommendations from the American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines and American College of Chest Physician (ACCP) guidelines suggest giving pharmacologic agents to every patient undergoing a total joint arthroplasty (TJA) procedure, except for those at a higher risk of bleeding than of developing VTE.5,6 However, debate continues on whether routinely VTE thromboprophylaxis after TJA should be administered in Asia.7,8 Several large-scale studies have reported that the incidence of VTE after TJA in Asian countries (13.8-17.1 per 100,000 individuals) is much lower than that of Western countries (approximately 100 per 100 000 individuals).9–12 Moreover, pharmacologic thromboprophylaxis using aspirin or other anticoagulants has been associated with substantial rates of adverse events, such as hematoma (6.38%), persistent wound drainage (2.68%), wound infection (2.67%), and major bleeding (0.52%).13 Therefore, to identify patients at risk of VTE and provide appropriate thromboprophylaxis is especially clinically relevant in Asian populations with a low incidence of VTE events.7,8,14,15
According to the Asia-Pacific VTE consensus, pharmacological thromboprophylaxis should be administered in Asian patients with elevated VTE risk who are undergoing TJA procedure, but not in patients with standard VTE risk.16 However, there is lack of evidence of an ideal scoring system or method for VTE risk stratification in the Asian population,17 including the Caprini or Wells scoring system.18,19 To classify Asian patients as having standard or elevated VTE risk, risk factors in Asian patients who are undergoing TJA procedure should be identified. According to the National Institute for Health and Care Excellence (NICE) guideline, several risk factors for VTE have been identified, including age over 60 years, critical care admission, dehydration, thrombophilia, obesity, history of VTE, pregnancy, and other medical comorbidities.20 However, the NICE guideline focused on risk factors for VTE in all patients admitted to hospital but not TJA patients.20 Only a few Asian studies have been conducted to validate the risk factors for VTE in patients who are undergoing TJA procedure.21–25 However, these few studies had limitations such as the inclusion of multiple surgeons with inconsistent selection criteria and protocols for thromboprophylaxis,21,22 a lack of multivariate analysis, and small number of included patients.22–25 More evidence is necessary to determine to risk factors for VTE events in Asian patients who are undergoing TJA procedure. In this study, we analyzed a single-surgeon case series from the database of a tertiary referral hospital over a 10-year period. The aim of this study was to validate the factors associated with symptomatic VTE events in a Taiwanese population.
2. METHODSFrom January 2010 to December 2019, we reviewed and included the records of patients who underwent unilateral or simultaneous bilateral primary TKA or THA performed by a single surgeon at Taipei Veterans General Hospital, a tertiary referral hospital in Taipei, Taiwan. This study was approved by our institutional review board (2022-04-011BC), which waived the requirement for informed consent. We screened patients who were eligible for analysis according to Taiwan’s National Health Insurance procedure codes for TKA (PCS-64169B) or THA (PCS-64162B). The indications for TKA were primary or secondary knee osteoarthritis (International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] code: M17), spontaneous osteonecrosis of the knee (ICD-10-CM codes: M90.55, M90.56) or rheumatoid arthritis (RA) of the knee joint (ICD-10-CM codes: M05.76, M05.86, M06.86, M06.9). We included patients who underwent primary THA procedures for primary or secondary hip osteoarthritis (ICD-10-CM code: M16), osteonecrosis of the femoral head (ICD-10-CM codes: M87.05, M87.15, M87.25, M87.35, M87.85) or RA of hip joint (ICD-10-CM codes: M05.75, M05.85, M06.85, M08.45, M08.85, M08.95). The exclusion criteria were (1) TKA or THA reconstruction procedure after tumor resection; (2) TKA or THA for acute fractures; (3) history of bleeding disorders or with active bleeding problems; (4) Child-Pugh class B or C cirrhosis; (5) active or history of knee or hip infection; and (6) allergy to low molecular weight heparin (LMWH) or aspirin; (7) incomplete follow-up at postoperative 90 days.
2.1. Criteria and protocol for prophylaxis of VTEFrom January 2010 to December 2017, the criteria for prophylaxis of VTE included: (1) body mass index (BMI) ≥30 (kg/m2), (2) presence of varicose veins, or (3) history of DVT or PE. However, one patient who underwent simultaneous bilateral TKA did not meet any of the above criteria for prophylaxis but developed PE during the perioperative period in December 2017. Therefore, we adjusted the criteria from January 2018 to December 2019 to include: (1) BMI ≥30 (kg/m2), (2) presence of varicose veins, (3) history of DVT or PE or (4) simultaneous bilateral TKA or THA procedures. Patients who fulfilled the criteria for VTE prophylaxis received an injection of LMWH (enoxaparin, Clexane, 2000 IU, 20 mg, 0.2 cc) immediately after surgery and every day thereafter, up to and including postoperative day (POD) 3 before transitioning to low-dose aspirin (Bokey, 100 mg) for 2 weeks. If the patient was diagnosed as having DVT based on clinical symptoms and positive findings on Doppler ultrasonography, low-dose aspirin was then administered for a total of 5 weeks. According to the prescribing information of Clexane, for surgical patients with moderate to high risk of VTE, a daily dose of 2000 to 4000 IU for 7 to 10 days should be administered for prophylaxis or until the risk of VTE has diminished. Because the VTE risk after TJA procedure was lower in Asian patients,17 we administered a daily Clexane dose of 2000 IU for prophylaxis in our series. We have not chosen more potent chemoprophylactic agents such as dabigatran or rivaroxaban because of the lower VTE risk in our population.17,26
2.2.Operative procedure and postoperative protocolsA single fellowship-trained orthopedic surgeon Wei-Ming Chen (WMC) performed all TKA or THA procedures under spinal or general anesthesia. A minimally invasive mid-vastus approach was used for all TKA procedures27 and a minimally invasive trans-gluteal approach was used for all THA procedures in a lateral decubitus position.28 A tourniquet was used in every TKA procedure. A drain was used in every TKA and THA procedure. Three types of TKA prosthesis were used: Nexgen (Zimmer Biomet, Warsaw, IN), NRG (Stryker, Mahwah, NJ), and Triathlon (Stryker). All TKA components were fixed with cement. Trident cup (Stryker) with SecurFit femoral stem (Stryker) was the only type of THA implant used. The fixation method for all THA components was cementless. All the patients started ambulation within postoperative 24 hours, usually in the morning on POD1.
2.3. Transfusion criteriaPatients who had signs of hypovolemia in the operation room or postanesthesia care unit due to excessive intraoperative blood loss or drainage amount received a transfusion of packed red blood cells accordingly. We measured hemoglobin level on POD 1 and would transfuse patients with 1 to 2 units of packed red blood cells if they had a (1) hemoglobin level <9.0 g/dL or (2) hemoglobin level 9.0 to 10.0 g/dL and symptoms suggestive of anemia (eg, dizziness, malaise, pale conjunctiva, tachycardia, hypotension).
2.4. Outcome domainsThe primary outcome domains included symptomatic DVT and PE events. Most of the studies have validated that the incidence of VTE events was highest in the early postoperative period, and postoperative 30 and 90 days were the two most common time points used to report postoperative VTE events.21–25,29–34 Therefore, we recorded postoperative 30- and 90-day VTE events as our primary outcome domains. We performed Doppler ultrasonography on patients who had positive clinical symptoms, including severe pain, warmth, swelling, erythematous or discolored skin, to confirm the diagnosis of DVT. Computed tomography pulmonary angiography was used to diagnose PE in patients who had symptoms such as sudden onset dyspnea, shortness of breath, chest pain, hypotension, or desaturation. After discharge from the hospital, outpatient follow-up visits would be arranged at postoperative 2 weeks, 1 month, 3 months, and then annually. During the outpatient follow-up visits, VTE events would be documented if the patients had positive clinical symptoms/signs and image findings. The patients were able to contact with a designated physician assistant for any complication after the TJA procedure. The patients would be asked to return to the emergency department or clinic if the patients had symptoms/signs suspicious for VTE events. In addition to the hospital medical records, the complication of every patient who underwent TJA procedure was recorded on a special medical chart for review. Postoperative infections, including surgical site complications and periprosthetic joint infection, have not been analyzed in this study.
2.5. Potential source of biasThe medical history has been reported by the patient, including smoking habits, history of VTE, and medical comorbidities. Recall bias could have occurred. A total of 81 (1.1%) patients have been excluded because of incomplete follow-up at postoperative 90 days. The risk of attrition bias was low.
2.6. Statistical analysisWe performed all analyses using SPSS version 22 (IBM Corp., Armonk, NY). We used descriptive statistics to characterize the patient demographics and rates of VTE in Tables 1 and 2, respectively. Fisher exact test was used to compare differences between the two groups for each categorical variable. A value of p < 0.05 was considered statistically significant. Multivariate logistic regression analysis was performed to validate the risk factors for VTE in this population. The input variables included age, sex, BMI, smoking history, diabetes mellitus (DM), RA, Charlson Comorbidity Index (CCI) score, VTE history, presence of varicose veins, receipt of TKA or THA procedure, unilateral vs bilateral procedure, receipt of pharmacological prophylaxis or transfusion and length of stay. The enter method was employed to validate risk factors associated with 30- and 90-day symptomatic VTE events. The significance level for factors in the multivariate logistic regression model was 0.05. The results were expressed in odds ratio with a 95% CI. Receiver operating characteristics curve analysis was used to validate the optimal cutoff value of the continuous variables.
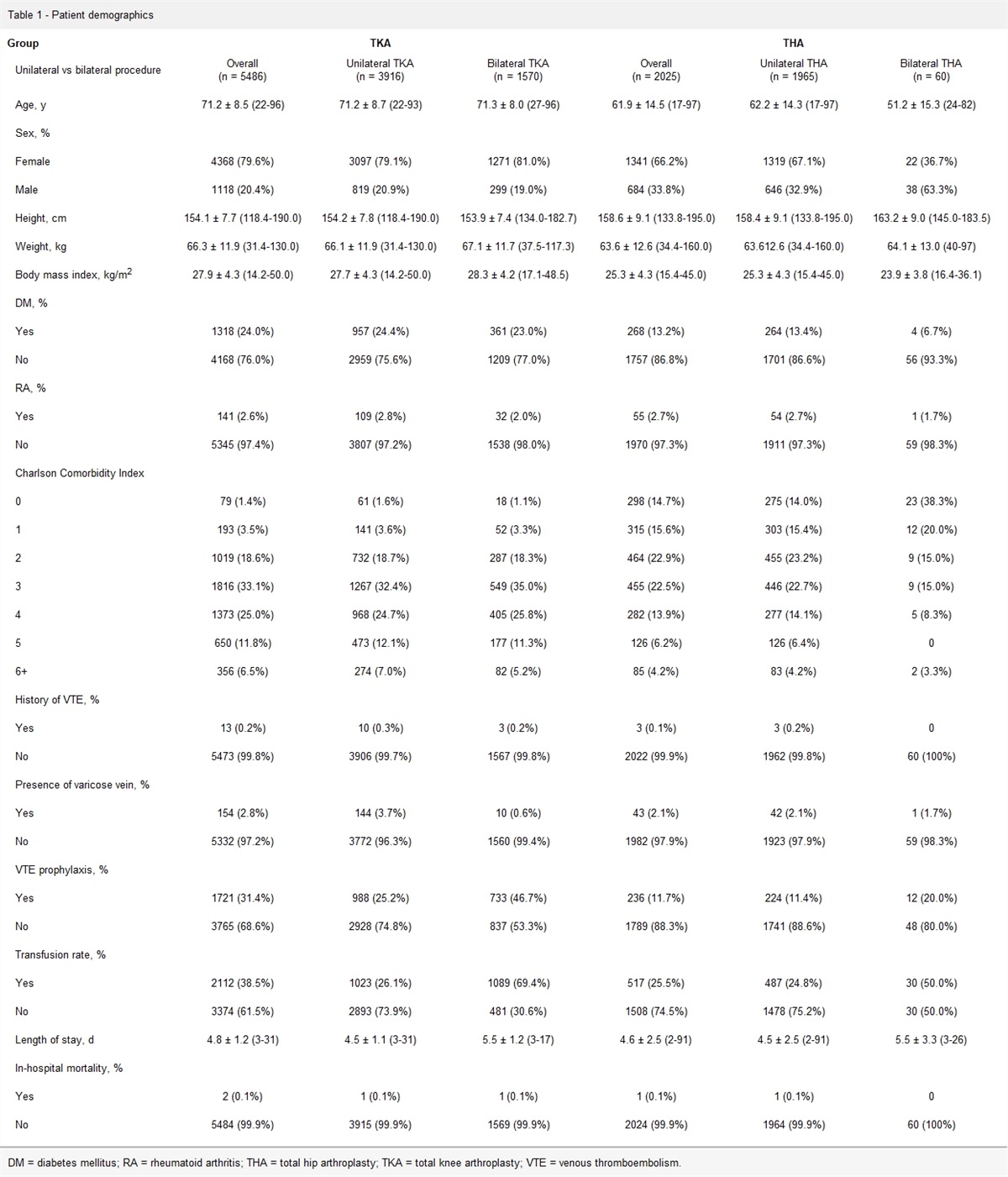
Table 1 - Patient demographics Group TKA THA Unilateral vs bilateral procedure OverallDM = diabetes mellitus; RA = rheumatoid arthritis; THA = total hip arthroplasty; TKA = total knee arthroplasty; VTE = venous thromboembolism.
VTE = venous thromboembolism.
aTwo pulmonary embolism events.
bNo pulmonary embolism events.
We included 7511 patients who underwent primary TJA (TKA procedure, N = 5486, 73.0%; THA procedure, N = 2025, 27.0%) for analysis, including 5881 (78.3%) unilateral and 1630 (21.7%) bilateral procedures. The mean age of the patients was 68.7 ± 11.2 years and 76% (N = 5709) of them were female. The mean body height, weight, and BMI were 155.3 ± 8.3 cm, 65.6 ± 12.1 kg, and 27.2 ± 4.4 kg/m2, respectively. In this cohort, we recorded the history of smoking (N = 623, 8.3%) and the incidence of DM (N = 1586, 21.1%), RA (N = 196, 2.6%), VTE (N = 16, 0.2%), and varicose veins (N = 197, 2.6%). The CCI score for the majority of the patients was 2 (N = 1483, 19.7%), 3 (N = 2271, 30.2%), or 4 (N = 1655, 22.0%) points. A total of 1957 (26.1%) patients received VTE thromboprophylaxis. The overall transfusion rate was 35.0%. The transfusion rates during and after the TJA procedure were 24.8% (N = 1853) and 14.2% (N = 1067), respectively. The mean length of stay was 4.7 ± 1.7 days. The in-hospital mortality rate was 0.04% (N = 3). The patient demographics stratified by TKA or THA, unilateral or bilateral procedures are shown in Table 1.
The 30-day symptomatic VTE rate in this cohort was 0.33% (N = 25), including symptomatic DVT (N = 23, 0.31%) and PE (N = 2, 0.02%). The 90-day symptomatic VTE rate was 0.44% (N = 33), including symptomatic DVT (N = 31, 0.41%) and PE (N = 2, 0.03%) (Table 2).
The results from multivariate regression analysis revealed that BMI ≥30 (aOR: 4.862, 95% CI, 1.776-13.313), bilateral TJA procedure (aOR: 2.665, 95% CI, 1.000-7.104), and presence of varicose veins (aOR: 9.946, 95% CI, 1.099-90.024) were associated with higher odds of 30-day symptomatic VTE events. Age ≥77 years (aOR: 2.358, 95% CI, 1.034-5.381) and BMI ≥30 (aOR: 2.832, 95% CI, 1.039-7.721) were associated with higher odds of 90-day symptomatic VTE events. In addition, VTE prophylaxis was associated with lower odds of 30-day (aOR: 0.097, 95% CI, 0.023-0.401) and 90-day symptomatic VTE events (aOR: 0.148, 95% CI, 0.040-0.545) (Table 3). The results of the univariate and multivariate analysis of all the registered variables were shown in Supplementary Tables S1–S2, https://links.lww.com/JCMA/A246.
Table 3 - Risk factors for postoperative venous thromboembolism events Independent variable β-coefficient 95% CI p 30-d VTE events BMI≥30 kg/m2 4.862 1.776-13.313 0.002 VTE prophylaxis 0.097 0.023-0.401 0.001 Bilateral TJA 2.665 1.000-7.104 0.050 Varicose veins 9.946 1.099-90.024 0.041 90-d VTE events Age ≥77 y 2.358 1.034-5.381 0.041 BMI ≥30 kg/m2 2.832 1.039-7.721 0.042 VTE prophylaxis 0.148 0.040-0.545 0.004The input variables included age, sex, BMI, smoking history, diabetes mellitus, rheumatoid arthritis, Charlson Comorbidity Index, VTE history, presence of varicose veins, total knee arthroplasty or total hip arthroplasty procedure, unilateral or bilateral procedure, receiving pharmacologic prophylaxis, blood transfusion, and length of stay.
BMI = body mass index; TJA = total joint arthroplasty; VTE = venous thromboembolism.
This is a single-surgeon case series of 7511 Taiwanese patients who underwent primary TJA over a 10-year study period. Patients with either (1) age ≥77 years, (2) BMI ≥30, (3) bilateral TJA procedure, or (4) presence of varicose veins were at higher odds of developing symptomatic VTE events. In addition, patients who received thromboprophylaxis were at lower odds of 30- and 90-day symptomatic VTE events.
According to a meta-analysis conducted by Lee et al,8 the routine use of chemoprophylaxis for VTE in every Asian patient after a TJA procedure remains debatable, because the incidence of symptomatic DVT (1.9%) and PE (0.01%) were very low in Asian patients who do not receive chemoprophylaxis.8 In recent Asian studies that validated the risk factors for VTE events in patients who underwent TJA procedures, the reported incidence of VTE ranged widely, 0.48%-46.8%.21–25,34 The large difference in the incidence of VTE resulted from the different strategies used to detect DVT. The incidence of DVT was generally higher in studies that reported asymptomatic DVT screened by routine Doppler ultrasonography (17.1%-46.8%),22–25,34 compared with studies that reported only symptomatic DVT events (0.48%-0.90%).21,33 In our study, the incidence of 30-day symptomatic DVT was 0.31% and the 90-day incidence was 0.41%, results similar to those from studies that reported symptomatic DVT events.21,33 The AAOS and ACCP guidelines both recommend against the routine screening for DVT using ultrasonography before and after elective arthroplasty procedures.5,6 This recommendation was based on two randomized controlled trials that found no difference in PE rates between the screened and non-screened groups.35,36 Patients with symptomatic DVT events usually show a greater extent of thrombosis, inadequacy of collateral vessels, associated vascular occlusion, and inflammation, any one of which may place them at higher risk of recurrent DVT events or progression to PE.33,37–39 Therefore, using ultrasonography to detect DVT events in symptomatic patients only, rather than the routine screening done in our study, has been shown to be appropriate.
Few studies have addressed the risk factors for VTE events in an Asian population.21–25 Xu et al,21 reviewing 15,326 patients who underwent elective TJA procedures, reported a symptomatic VTE rate of 0.48% (N = 73). Multivariate regression analysis revealed that the risk factors for VTE were older age, TKA (compared to THA), use of a drain, and delayed ambulation. However, specifics of the thromboprophylaxis criteria, the choice of pharmacologic agents, and the proportion of patients who received thromboprophylaxis were unclear and not analyzed. Zhang et al22 conducted a single-surgeon case series of 963 patients. Routine screening of DVT was performed and the overall VTE rate was 17.96% (N = 173). In univariate analysis, age, BMI, cholesterol, high-density lipoprotein, apolipoprotein A, history of tumors, visual analog scale score, and operative duration were associated with VTE events. However, the results of multivariate regression analysis were lacking. All the patients in this study received pharmacological thromboprophylaxis with either LMWH (2850 IU, once daily) or rivaroxaban (10 mg, once daily). The dosage level of LMWH used for prophylaxis was considered to be moderate. Interestingly, the VTE rate in the LMWH group (48.56%) was much higher than that in the rivaroxaban group (6.23%). However, the criteria for choosing either agent were not described and selection biases could have existed. The three other single-surgeon case series reports had higher quality of research methodology.23–25 In each of these, all patients received pharmacologic thromboprophylaxis with a consistent protocol and all were routinely screened for DVT using Doppler ultrasonography. Age, BMI, bilateral TJA procedure, history of DM, hyperglycemia, and elevated preoperative D-dimer and homocysteine were associated with VTE events.23–25 Compared with these studies,21–25 our study had several advantages, including a larger patient population (N = 7511) and a single-surgeon case series with consistent protocol for thromboprophylaxis and perioperative care. However, more evidence is needed to enable risk stratification of VTE events in the Asian population.
We identified several risk factors that were consistent with the findings of other studies, such as older age, higher BMI, and receipt of simultaneous bilateral procedures.21–25 Studies have indicated that older patients often have vascular sclerosis, venous valve dysfunction, coagulopathy, and inactivity after TJA, all of which might predispose them to DVT events.14,21,23 Obesity has been associated with an increased risk of all complications, readmissions, reoperations, and revisions.40 The reduced activity level and slower venous return in obese patients may have contributed to the formation of venous thrombus in the lower extremities.41 Compared with unilateral TJA procedures, receipt of bilateral TJA procedures may increase the risk of all complications, including VTE events, perhaps due to the longer operation time and decreased physical activity during the early postoperative period.42 The higher concentrations of von Willebrand factor, fibrinogen, and endothelium-derived mediators in DM patients may lead to increased blood viscosity, platelet activation, and adhesion.43 In addition, fibrinolysis is impaired by the increased level of plasminogen activator inhibitor-1 in DM patients.43 However, whether DM is associated with increased risk of VTE following TJA procedures is controversial.21,23,24,34,44 In our study, we failed to observe an association between DM and VTE events. Interestingly, we validated the presence of varicose veins as a risk factor for VTE following TJA procedures. The increased levels of prothrombotic and inflammatory markers, as well as the slower blood flow in patients with varicose veins, could have led to an increased risk of VTE events in these patients.45 Notably, every risk factor identified in the multivariate regression model would be considered to influence the outcome measure. Indeed, there might be statistical fluctuation. Because the 30- and 90-day symptomatic VTE events were both important outcome measures for postoperative VTE events, we would consider all these risk factors, either associated with 30- or 90-day VTE events, to have an impact on early postoperative VTE events rather than to emphasize the effect at a certain point of time.
We should recognize some limitations of this study. First, we performed Doppler ultrasonography only on patients with positive clinical symptoms of DVT. Therefore, we did not report asymptomatic DVT events. However, the higher risk of progression to PE in symptomatic DVT patients,33,37–39 as well as the recommendations against the routine ultrasonographic screening of DVT following TJA procedures from the AAOS,5,6 make this clinical practice appropriate. Second, despite the large number of included patients in this study (N = 7511), the number of symptomatic VTE events was small (N = 33, 0.44%). As the number of events becomes smaller, the unadjusted R2 tends to increase. The difference between the adjusted and unadjusted coefficient of determination might be the explanation to this finding. The adjusted R2, which accounts for degrees of freedom is an approximately unbiased estimator of the
留言 (0)