
記住我


Pancreatic cancer is one of the deadliest cancers, ranking as the seventh leading cause of cancer-related deaths in Taiwan in 2020,1 and the sixth leading cause of cancer-related deaths between 1992 and 2017 worldwide.2 Over 80% of patients with pancreatic cancer have adenocarcinoma, and unfortunately, the disease is often diagnosed at an advanced stage, with only about 20% of patients being eligible for surgery at the time of diagnosis. Systemic treatment is the mainstay of therapy for inoperable patients, and combining definitive radiotherapy (RT) with chemotherapy has been shown to improve local control of the disease.3 However, the prognosis for inoperable pancreatic adenocarcinoma remains poor, with a median overall survival of only around 1 year. Radiation dose escalation has been shown to improve disease control and even survival after induction chemotherapy.4 However, the proximity of the tumor to adjacent gastrointestinal (GI) organs presents a challenge. The current recommended radiation dose for definitive RT is 45 to 54 Gy, with dose constraints of 55 Gy for the duodenum and stomach.5 To overcome this limitation, different approaches have been tried.
To better target the tumor while minimizing damage to surrounding organs, conformal radiation therapy is a viable option. This can be achieved through the use of techniques such as carbon ion or proton RT, which take advantage of Bragg peak and sharper lateral penumbra. These therapies have shown promising overall survival rates in previous studies, with carbon ion therapy achieving 26.2 months and proton therapy achieving 25.6 months.6,7 Another approach to improving radiation therapy is by using traditional photon RT with real-time magnetic resonance imaging (MRI) guidance, which allows for precise monitoring of the tumor and surrounding GI tract during treatment. This technique has also shown promising results, with an overall survival rate of 20.8 months.8 While randomized controlled trials comparing different RT modalities are not yet available, studies have shown that approaches utilizing escalated radiation doses, either proton, carbon, or MRI-guided photon, have resulted in better overall survival rates compared to conventional concurrent chemoradiotherapy, which typically only achieves around 1 year of survival.
Another possible method for improving outcomes is by separating the tumor from the adjacent GI tract using a surgically inserted spacer or injection of a certain fluid. For example, endoscopic hydrogel injection was successfully used in a previous study to increase the space between the pancreatic head and adjacent duodenum, allowing for dose escalation.9 The results of that study showed that an 8 mm separation could reduce the mean volume receiving 20 Gy (V20 or more) value to the duodenum by 90.38%, with a relatively small additional dose reduction after 8 mm of separation. This technique of injecting materials to separate the target from surrounding tissues before a procedure is known as hydrodissection, and it has been applied in ophthalmology, general surgery, and interventional radiology.10–12 Hydrodissection may also be achieved by percutaneously puncturing the prepancreatic fascia under CT guidance. After injecting the substance, the distance between the pancreatic tumor and bowel loop may be increased.
To our knowledge, no previous study has investigated the feasibility of using hydrodissection in real-world situations. Therefore, we conducted a review of patients who received RT at Taipei Veterans General Hospital (TVGH) in order to estimate what percentage of the patients could potentially have benefitted from these techniques if they were to become clinically available.
2. METHODSPatient data were collected from the TVGH cancer registry. The inclusion criteria for this study were patients: (1) aged 20 years or more; (2) with pathological proof of pancreatic adenocarcinoma; (3) clinical stage I-III; (4) who were inoperable; and (5) who received definitive RT between 2010 and 2016 at TVGH. The exclusion criteria were patients: (1) who did not complete the RT course; and (2) with distant metastasis or other synchronous cancer noted before RT. The authors did not have access to information that could identify individual participants during or after data collection. The tumors were staged according to the AJCC 7th system. Simulated computed tomography (CT) scans before RT of each eligible patient with gross tumor volume (GTV) delineated by a radiation oncologist were provided to an interventional radiologist and a gastroenterologist. They then referred to the medical records and medical images of the patient to estimate whether a hypothetical approach of hydrodissection by injecting a fluid such as normal saline, hydrogel, or hyaluronic acid was feasible to dissect the GTV away from the adjacent GI hollow organ by at least 1 cm or more using a 21 gauge needle for the CT-guided injection (for the interventional radiologist) or endoscopic injection (for the gastroenterologist). The distance between the nearest GI tract and the tumor was measured as the shortest distance between their outer contours. For uncinate process tumors, the distance between the closest duodenum was measured (second or third portion). Endoscopic feasibility was judged by the gastroenterologist based on CT imaging. The interventional radiologist decided whether a trans-organ or trans-target approach was necessary. When an obliterated fat plan and/or irregular interface between the cancer and GI tract was noted, direct invasion was considered. Interferential statistics were performed with two-tailed Fisher exact test on a 2 by 2 contingency table. A p value < 0.05 was considered significant.
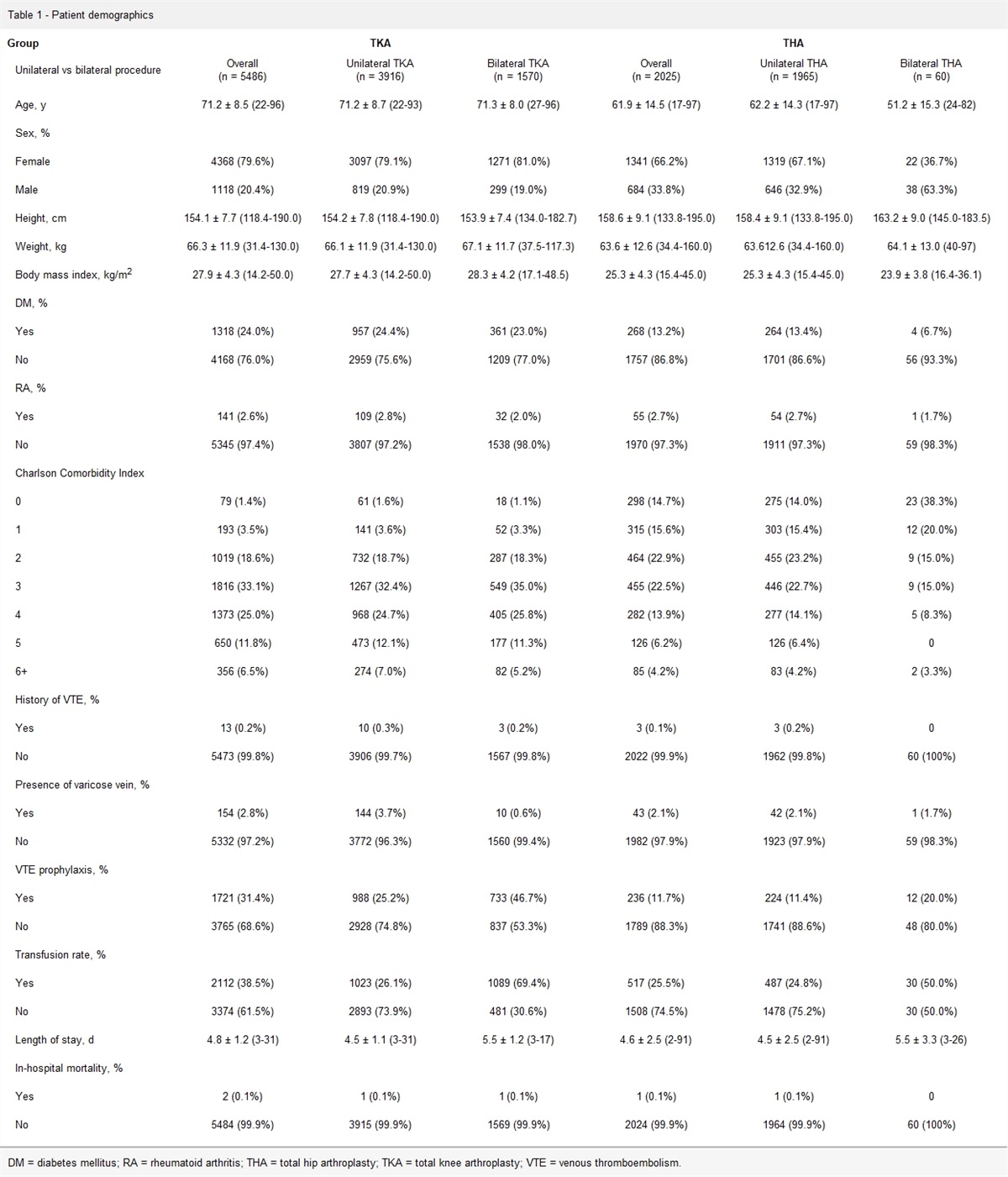
3. RESULTS 3.1. Patient characteristicsWe reviewed 50 consecutive patients, and their characteristics are shown in Table 1. The median age was 66 years, and half of the patients were male. Most patients had stage 3 disease. The pancreatic head was the most common origin, secondary to the pancreatic body.
Table 1 - Patient characteristics Characteristic n = 50 Age, median (range), y 66 (33-93) Male 25 (50%) Stage, % 1 4 (8%) 2 12 (24%) 3 34 (68%) Site of pancreas, % Head 23 (46%) Neck 6 (12%) Body 19 (38%) Tail 2 (4%)The feasibility assessment after reviewing the medical images is shown in Table 2. We found that the stomach was the most common GI tract closest to the GTV. Half (50%) of the GTV was abutting or suspected to have invaded the closest GI organ. CT-guided injection was determined to be feasible in 23 (46%) patients. Organ puncture was determined to be necessary to approach in 10 of these patients. Puncture of the colon is not acceptable due to the risk of severe infection. The proposed trajectory of the CT-guided injection was indicated by the interventional radiologist on the representative axial CT image for each patient, as shown in Fig. 1. Complete images are provided in the Supplementary Appendix, https://links.lww.com/JCMA/A242. A CT-guided approach was not considered to be feasible in most patients because of suspected direct tumor invasion to adjacent GI organs. The gastroenterologist considered that hydrodissection by an endoscopic approach was feasible in 31 (62%) patients. The most common reason for the patient being considered not feasible was suspected direct invasion, in line with the assessment of the interventional radiologist. However, the feasibility evaluations of 12 (24%) patients were different between the gastroenterologist and the radiologist. Complete assessment records of each patient are provided in the Supplementary Appendix, https://links.lww.com/JCMA/A243. A comparison of the feasibility assessments of both approaches is shown in Table 3. We found 14 (28%) discrepancies among the 50 patients reviewed. Except for one patient who had no available trajectory with a CT-guided approach but was considered feasible by endoscopic injection, the other 13 patients had different interpretations of whether direct invasion was present in the CT images. Two-tailed Fisher exact test on the 2 by 2 contingency table found a p value of 0.001 showing that the association of feasibility assessment on both approaches was statistically significant.
Table 2 - Feasibility assessment Characteristic n = 50 Closest GI tract, % Stomach 28 (56%) Duodenum 19 (38%) Colon 3 (6%) Closest distance, % 0 25 (50%) ≤10 mm, >0 13 (26%) >10 mm 12 (24%) CT-guided feasibility, % Feasible 23 (46%) Organ puncture Unnecessary 13 (26%) Necessary 10 (20%) Stomach 7 (14%) Liver 3 (6%) Not feasible 27 (54%) Direct invasion 25 (50%) No available trajectory (trans-colon needed) 2 (4%) Endoscopic feasibility, % Feasible 31 (62%) Not-feasible 19 (38%) Difficult trajectory 2 (4%) Direct invasion 17 (34%)CT = computed tomography; GI = gastrointestinal.
CT = computed tomography.
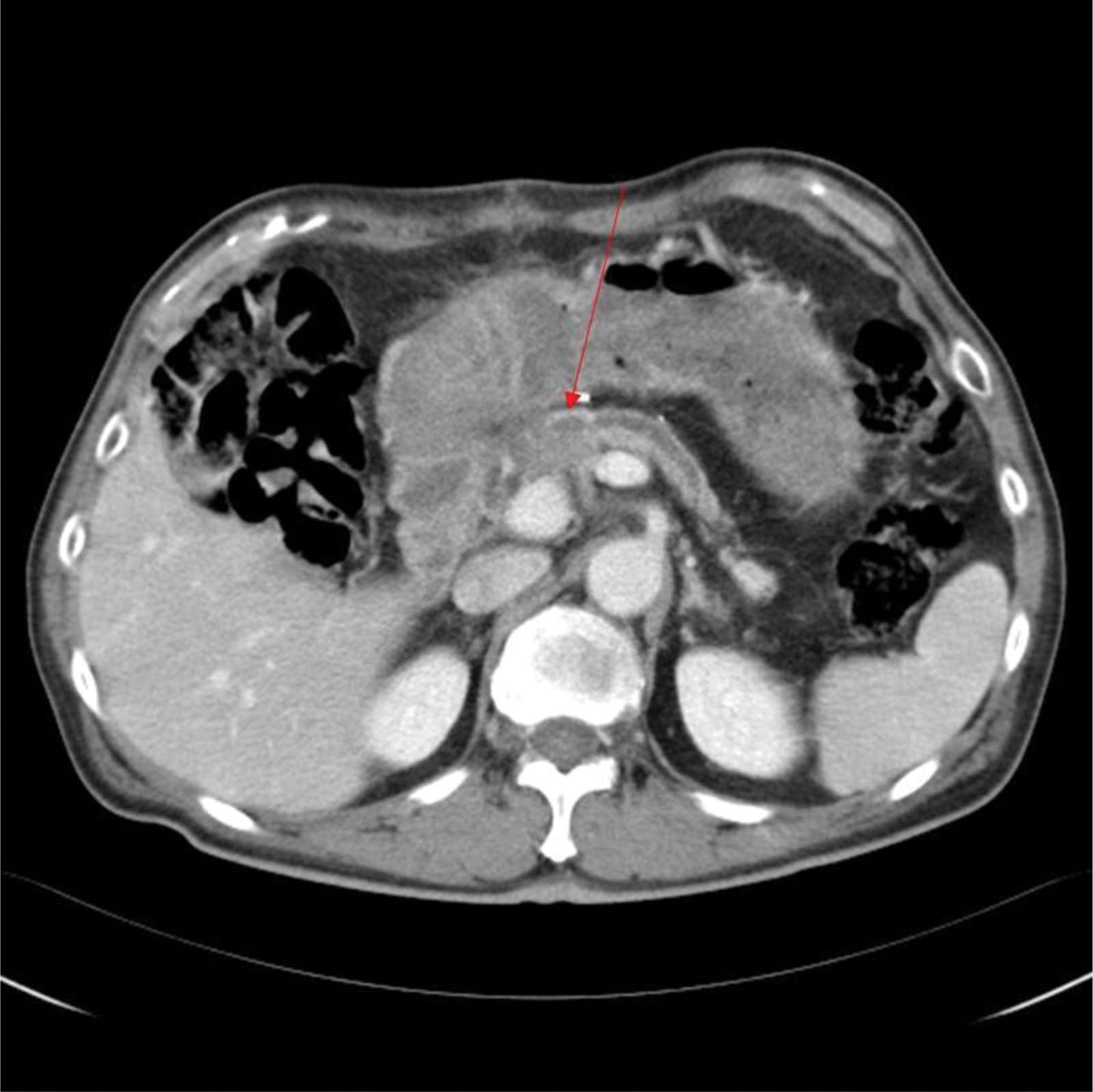
 Fig. 1:
Fig. 1: Representative proposed trajectory for CT-guided hydrodissection. A trans-stomach pathway was required as assessed by the interventional radiologist to separate the target from adjacent stomach and duodenum. Proposed percutaneous trajectories of all 50 patients, if feasible, are listed in the supplement. CT = computed tomography.
4. DISCUSSIONThis study aimed to evaluate the feasibility of using hypothetical hydrodissection with a needle approach before irradiating pancreatic tumors in 50 consecutive patients who received definitive RT at TVGH. We found that almost all of the patients had a suitable trajectory for a needle approach using either CT-guided or endoscopic techniques. However, for some patients, hydrodissection was not feasible because the tumor had already invaded an adjacent hollow organ.
The idea of separating the GTV from surrounding tissues using an artificial spacer before RT is not new, and it has been widely used in the treatment of prostate cancer, where the tumor is close to the rectum. Commercial products such as SpaceOARTM are available for this purpose.13 Surgically inserted spacers, made of Gore-TexTM (W.L. Gore & Associates, Inc., Newark, DE), silicone, or glycolic acid, have also been reported.14–16 However, surgical insertion is highly invasive and requires general anesthesia, and the long-term safety of leaving the spacer permanently inside the body is uncertain.
In the past, pancreatic adenocarcinoma was commonly believed to progress mainly through distant dissemination during the initial stages of treatment, with local failure having only a minor impact on patient outcomes. However, findings from a carbon ion study conducted in Japan indicated that local control may play a more significant role in treating this disease than previously thought. One study utilized regular positron emission tomography scans to track local progression, and discovered that nearly half of the patients experienced local failure within 1 year of receiving a carbon ion radiation therapy dose of 43.2 to 55.2 GyE in 12 fractions.6 Interestingly, CT scans of the same patient cohort failed to detect local failure even after more than 2 years. The findings of the study suggest that achieving local control may be a critical factor in treating pancreatic adenocarcinoma, and that relying solely on CT scans to detect local disease progression may have limitations. Even with the use of a high linear energy transfer and low oxygen enhancement ratio source of carbon ion radiation therapy, almost all patients in the study experienced local progression of the disease within 3 years of treatment.6 This underscores the need to develop strategies that can facilitate further dose escalation in radiation therapy, even when using advanced techniques such as carbon ion radiation therapy.
Hydrodissection with a needle approach may be a suitable, minimally invasive alternative to surgical insertion. However, the optimal fluid for this technique has yet to be determined. Saline is an economic and readily available option, but it does not adhere to the GTV and is absorbed by the body within days. Patient blood can create a hematoma that poses a risk of infection. Hydrogel has shown promise in treating prostate cancer and was tried in a cadaver study of pancreatic head cancer.9,13 However, for pancreatic cancer, the fluid would need to be injected into the highly mobile tissues surrounding the GI tract, and it is uncertain whether the injected spacer would remain in place. In a recently published study, endoscopic injection of 2.5 to 10 cc hydrogel was performed successfully in six patients with pancreatic ductal adenocarcinoma in the head or neck of the pancreas to create a mean space of 7.7 ± 2.7 mm shown by simulation CT.17
As an illustrative case, we performed pre-RT CT-guided hydrodissection via the off-label use of sodium hyaluronate solution (HYAJOINTTM, Kaohsiung, Taiwan) to separate the stomach away from the GTV of a patient with pancreatic metastasis of small cell lung cancer in March 2023 (Fig. 2). We used an 18-gauge percutaneous transhepatic cholangiography puncture needle to puncture the space between the stomach and pancreatic mass, and then injected diluted contrast medium (1:20) to confirm the needle location and contrast retention site. At the final location after satisfactory hydrodissection with the diluted contrast medium, a total of 30 cc of sterile sodium hyaluronate solution (HYAJOINTTM) was injected with 3 cc of contrast medium. The patient received the first fraction of RT after verification by cone-beam-CT that the injected material remained unchanged 2 hours after injection. However, the injected material was no longer visible on the second day, 17 hours after the injection. Although it took several weeks to complete the course of conventional RT and the stability of the injected material was a problem, the current trend of stereotactic body radiation therapy (SBRT) would require less time to complete, or even single fraction RT immediately after hydrodissection may be possible.
 Fig. 2:
Fig. 2: Illustrative case of CT-guided hydrodissection in a patient with pancreatic metastasis of small cell lung cancer. A, Simulation CT of the patient before hydrodissection: magenta, GTV; yellow, stomach; green, colon. B, CT-guided injection of sodium hyaluronate successfully pushed the stomach away from the GTV. CT = computed tomography; GTV = gross tumor volume.
In this study, we found that 24% of the patients had a distance of at least 1 cm between the GTV and adjacent GI tract. Modeling studies have shown that a separation of 8 mm is sufficient to facilitate irradiating the pancreatic head via SBRT with a prescribed dose of 33 Gy in five fractions.9 Thus, SBRT with further escalation in the dose may be prescribed if the patient can undergo pre-RT hydrodissection.
While our study provides valuable insights into the potential of hydrodissection for separating the GTV from adjacent tissues before RT for pancreatic adenocarcinoma, there are some limitations that should be considered. Feasibility was assessed based solely on medical records and imaging, and actual testing may be necessary to confirm whether hydrodissection is possible, although a recently published study using endoscopic injections of hydrogel showed promising results in six patients.17 In addition, a previous study on CT-guided hydrodissection before biopsy showed a technical success rate of 86%.18 However, even if the injection point is successfully accessed, the efficacy of the hydrodissection may be limited by the ability of the fluid to stay in place, which could compromise its utility. We will conduct further clinical studies to verify this issue. Finally, the benefit on pancreatic cancer is still theoretical, because a clinical trial of endoscopic hydrodissection has just been performed and published.17 Moreover, there may not be a randomized controlled study to confirm the benefit in the near future. However, the benefit of hydrogel spacer injection between the prostate and rectum before RT for prostate cancer was shown in a phase 3 randomized controlled trial of 222 patients, which showed reduced rectal toxicity and better quality of life.19
In conclusion, based on our review of medical images from 50 inoperable pancreatic adenocarcinoma patients undergoing RT at TVGH, we determined that a hypothetical hydrodissection procedure before RT could have been beneficial for about half of these patients. By increasing the distance between the tumor and adjacent GI tract through either CT-guided or endoscopic injection, these patients could potentially receive a higher radiation dose during treatment. The majority of patients deemed not feasible for hydrodissection were found to be ineligible due to suspected tumor invasion, rather than a lack of suitable injection trajectory. With the identification of a suitable fluid spacer, many patients with pancreatic cancer in close proximity to the GI tract could potentially receive a minimally invasive needle-based hydrodissection procedure before RT, negating the need for surgically inserted spacers, to achieve escalated RT dose and potentially better survival outcomes.
ACKNOWLEDGMENTSThe authors acknowledge the Taipei Veterans General Hospital Cancer Registry Database for providing some of the data used in this study. The authors also like to express our gratitude to ChatGPT for its assistance in optimizing the English grammar of this manuscript.
APPENDIX A. SUPPLEMENTARY DATASupplementary data related to this article can be found at https://links.lww.com/JCMA/A242 and https://links.lww.com/JCMA/A243.
REFERENCES 1. Taiwan Cancer Registry Center [2022-07-27]. Available at: https://twcr.tw/?page_id=1843&lang=en. 2. Lippi G, Mattiuzzi C. The global burden of pancreatic cancer. Arch Med Sci. 2020;16:820–4. 3. Hammel P, Huguet F, van Laethem J-L, Goldstein D, Glimelius B, Artru P, et al.; LAP07 Trial Group. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: the LAP07 randomized clinical trial. JAMA. 2016;315:1844–53. 4. Ma SJ, Prezzano KM, Hermann GM, Singh AK. Dose escalation of radiation therapy with or without induction chemotherapy for unresectable locally advanced pancreatic cancer. Radiat Oncol. 2018;13:214. 5. Guidelines N. NCCN guidelines pancreatic adenocarcinoma Version 1.2022 2022. Available at: https://www.nccn.org/guidelines/category_1. 6. Hiroshima Y, Fukumitsu N, Saito T, Numajiri H, Murofushi KN, Ohnishi K, et al. Concurrent chemoradiotherapy using proton beams for unresectable locally advanced pancreatic cancer. Radiother Oncol. 2019;136:37–43. 7. Shinoto M, Yamada S, Terashima K, Yasuda S, Shioyama Y, Honda H, et al.; Working Group for Pancreas Cancer. Carbon ion radiation therapy with concurrent gemcitabine for patients with locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2016;95:498–504. 8. Rudra S, Jiang N, Rosenberg S, Olsen J, Parikh P, Bassetti M, et al. High dose adaptive MRI guided radiation therapy improves overall survival of inoperable pancreatic cancer. Int J Radiat Oncol Biol Phys. 2017;99:E184. 9. Rao AD, Feng Z, Shin EJ, He J, Waters KM, Coquia S, et al. A novel absorbable radiopaque hydrogel spacer to separate the head of the pancreas and duodenum in radiation therapy for pancreatic cancer. Int J Radiat Oncol Biol Phys. 2017;99:1111–20. 10. Lee SJ, Choyke LT, Locklin JK, Wood BJ. Use of hydrodissection to prevent nerve and muscular damage during radiofrequency ablation of kidney tumors. J Vasc Interv Radiol. 2006;17:1967–9. 11. Yanoff M, Duker JS. Ophthalmology. Netherland: Elsevier Health Sciences; 2008. 12. Acton QA. Issues in surgical research, techniques, and innovation: 2011 edition. USA: ScholarlyEditions; 2012. 13. Armstrong N, Bahl A, Pinkawa M, Ryder S, Ahmadu C, Ross J, et al. SpaceOAR hydrogel spacer for reducing radiation toxicity during radiotherapy for prostate cancer. A systematic review. Urology. 2021;156:e74–85. 14. Nagai S, Nagayoshi K, Mizuuchi Y, Fujita H, Ohuchida K, Ohtsuka T, et al. Laparoscopic spacer placement for recurrent sacral chordoma before carbon ion radiotherapy: a case report. Asian J Endosc Surg. 2020;13:582–5. 15. Cobianchi L, Peloso A, Vischioni B, Panizza D, Fiore MR, Fossati P, et al. Surgical spacer placement prior carbon ion radiotherapy (CIRT): an effective feasible strategy to improve the treatment for sacral chordoma. World J Surg Oncol. 2016;14:1–9. 16. Serizawa I, Kusano Y, Kano K, Shima S, Tsuchida K, Takakusagi Y, et al. Three cases of retroperitoneal sarcoma in which bioabsorbable spacers (bioabsorbable polyglycolic acid spacers) were inserted prior to carbon ion radiotherapy. J Radiat Res. 2022;63:296–302. 17. Narang AK, Hong TS, Ding K, Herman J, Meyer J, Thompson E, et al. A multi-institutional safety and feasibility study exploring the use of hydrogel to create spatial separation between the pancreas and duodenum in patients with pancreatic cancer. Pract Radiat Oncol. 2023:S1879–8500(23)00340. 18. Asvadi NH, Arellano RS. Hydrodissection-assisted image-guided percutaneous biopsy of abdominal and pelvic lesions: experience with seven patients. AJR Am J Roentgenol. 2015;204:865–7. 19. Mariados N, Sylvester J, Shah D, Karsh L, Hudes R, Beyer D, et al. Hydrogel spacer prospective multicenter randomized controlled pivotal trial: dosimetric and clinical effects of perirectal spacer application in men undergoing prostate image guided intensity modulated radiation therapy. Int J Radiat Oncol Biol Phys. 2015;92:971–7.
留言 (0)