
記住我


Hepatitis D virus (HDV) is a small, defective virus that requires hepatitis B surface antigen (HBsAg) from hepatitis B virus (HBV) for virion assembly and transmission.1–3 An estimated 10.58% of patients (72.5 million individuals) with chronic HBV infection were coinfected with HDV.4 In Taiwan, HDV infection has been an important etiology of fulminant hepatitis.5 Furthermore, chronic HDV infection may accelerate the progression of liver fibrosis, cause earlier hepatic decompensation, and increase the risk of developing hepatocellular carcinoma (HCC).6–11 Sexual contact with prostitutes followed by needle sharing among injection drug users (IDUs) or injection with contaminated needles were the major transmission routes of HDV.12–14 Since the successful implementation of a universal HBV vaccination program for newborns in 1984 and the sustained education of the general public via mass media and health-care workers after the discovery of the major transmission route of HDV infection, the prevalence of HDV infection has decreased significantly in Taiwan.15 Nevertheless, HDV infection remains notably high within high-risk groups, such as IDUs and patients with human immunodeficiency virus (HIV) infection.13
Even though HDV infection has been decreasing in many parts of the world, its seroprevalence rate remains high in some countries, such as Mongolia.16–20 Moreover, Mongolia has the highest incidence of HCC development in the world, and only 13.8% of patients with HCC have undergone curative resection.17,21–23 The seroprevalence rate of HBV and hepatitis C virus (HCV) infection in Mongolia were 10% and 15%, respectively, and the majority (75%-100%) of the HBV-infected subjects were also coinfected with HDV.16,24,25 In contrast to HBV and HCV infection, for which potent antiviral therapy are available, only bulevirtide has been conditionally approved for the treatment of patients with compensated chronic hepatitis D in Europe as of 2020.26,27 Elucidating the transmission routes of HDV infection and taking effective preventive strategies are key to reducing HDV infection in Mongolia.
In this study, we aimed to elucidate the risk factors associated with HDV infection in Mongolia, propose preventive strategies, and evaluate the secular changes at the end of the collaborative 3-year Taiwan-Mongolia projects.
2. METHODS 2.1. Site visits to MongoliaWith the arrangement of and help from the Mongolian collaborators, Taiwan investigators (including hepatologists, infection control specialists, and officials from the Taiwan Center of Disease Control) visited Mongolia twice, in 2016 and 2018. In 2016, we visited the Third State Central Hospital of Mongolia, the Ministry of Health and the Ministry of Education, Science, and Culture of Mongolia, and the Mongolian Taiwanese Science and Technology Foundation, meeting with the faculties (specialists in gastroenterology, infectious diseases, and internal medicine) and with the Mongolian project team members of the Second Department of the Mongolian National University of Medical Science (MNUMS), the National Center for Communicable Diseases (NCCD), the First Central Hospital of Mongolia, the Dental Center (a private dental clinic), and the University General Hospital. During the 3-day visit, the Taiwanese and Mongolian investigators shared viral hepatitis prevalence status, disease burden, preventive strategies, policy, and experiences by giving talks and conducting discussions. Onsite visits also included the inspection of routine clinical procedures, including blood sampling, injection, dental care, hemodialysis, traditional medicine, disinfection of endoscopies, etc, to evaluate whether the procedures carried out had been standardized and optimized. The team also recorded potential risk factors to be included in the questionnaire design and the lectures and training sessions of infection control workshops to be held in the following years. In 2018, the Taiwan investigators revisited Mongolia. This time, the agenda included participation in the combined meetings of Digestive Diseases Week (DDW) and an infection control workshop based on the training program established in Taiwan in 2017. A site visit was arranged to the primary health-care unit in the countryside, and lectures were given on epidemiology and preventive strategies of viral hepatitis B, C, and D.
2.2. PatientsWe retrospectively collected 216 serum samples of patients with acute hepatitis from the Department of Internal Medicine, University Hospital of MNUMS, Ulaanbaatar, Mongolia, between 2017 and 2019. All enrolled patients were tested for HBsAg, hepatitis B e antigen (HBeAg), anti-HBe, anti-HCV, and anti-HDV. Those who tested positive for HBsAg and anti-HDV were further analyzed for HBV DNA and HDV RNA and genotyped by sequencing of HBV and HDV genomes. Risk factors potentially associated with HDV infection were analyzed using a questionnaire (Supplementary Table S1, https://links.lww.com/JCMA/A241).
In addition, to elucidate the secular changes of HDV infection, we reviewed newly diagnosed viral hepatitis patients’ data registered at the NCCD, Mongolia, from 2011 to 2021. The NCCD is a specialized organization responsible for monitoring epidemiology, nationwide immunization, prevention, and management of infectious diseases in Mongolia.
This study fulfilled the standards of the Declaration of Helsinki and current ethical guidelines. It was approved by the Institutional Review Board of the University Hospital of MNUMS. All patients completed the written informed consent form before enrollment.
2.3. Serological viral markers and biochemistry testsSerum HBsAg, antibody against HBsAg (anti-HBs), hepatitis B e antigen (HBeAg), antibody against HBeAg (anti-HBe), IgM anti-HBc, and anti-HCV were tested using radioimmunoassay kits (HISCL-5000; Sysmex, Japan). An enzyme immunoassay (EIA) kit was used to detect IgM anti-HDV (Sorin Biomedica Diagnostics, Italy; DRG Instruments GmbH, Marburg, Germany, for anti-HDV IgM; Fortress Diagnostics HDV IgG UK for anti-HDV IgG). Serum albumin, alanine aminotransferase (ALT), and total bilirubin levels were measured with a systemic multiautoanalyzer (Chemix 180; Sysmex).
2.4. Detection, genotyping, and sequencingSerum HBV DNA was detected by polymerase chain reaction (PCR) using primers synthesized according to the consensus sequence of the precore region.28 The quantification of HBV DNA was measured based on a Cobas Amplicor HBV monitor (Roche Diagnostic System, Basel, Switzerland). The limit of detection for this assay was 300 copies/mL. Genotyping of HBV was performed by PCR, followed by sequencing of the surface gene of HBV.28,29 Serum HDV RNA was detected using reverse transcription followed by PCR.30–32 Thus, according to the dilution factors used during the RNA extraction and RT procedures, the sensitivity of the assay to detect HDV RNA in clinical samples was 400 copies/mL of serum, and the linearity of quantification ranged from 2 × 103 to 2 × 109 copies/mL.31 The sensitivity of the assays was about 100 viral genomes per mL. HDV genotypes were determined by restriction fragment length polymorphism (RFLP).33 To confirm the genotyping results, sequencing of PCR products was also performed. Sequences of the PCR products of HBV or HDV were determined by the dye terminator cycle sequencing reaction according to the standard protocol provided by the manufacturer (Dye Terminator Cycle Sequencing Core Kit 402117; Perkin Elmer Cetus Corp., Norwalk, CT). The sequencing products were precipitated with alcohol and analyzed in an ABI 373A sequencer (Perkin Elmer Cetus Corp.).
2.5. Statistical analysisCategorical variables were compared using Pearson’s chi-square analysis or Fisher’s exact test, and continuous variables were compared using the Mann-Whitney U test. A two-tailed p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY).
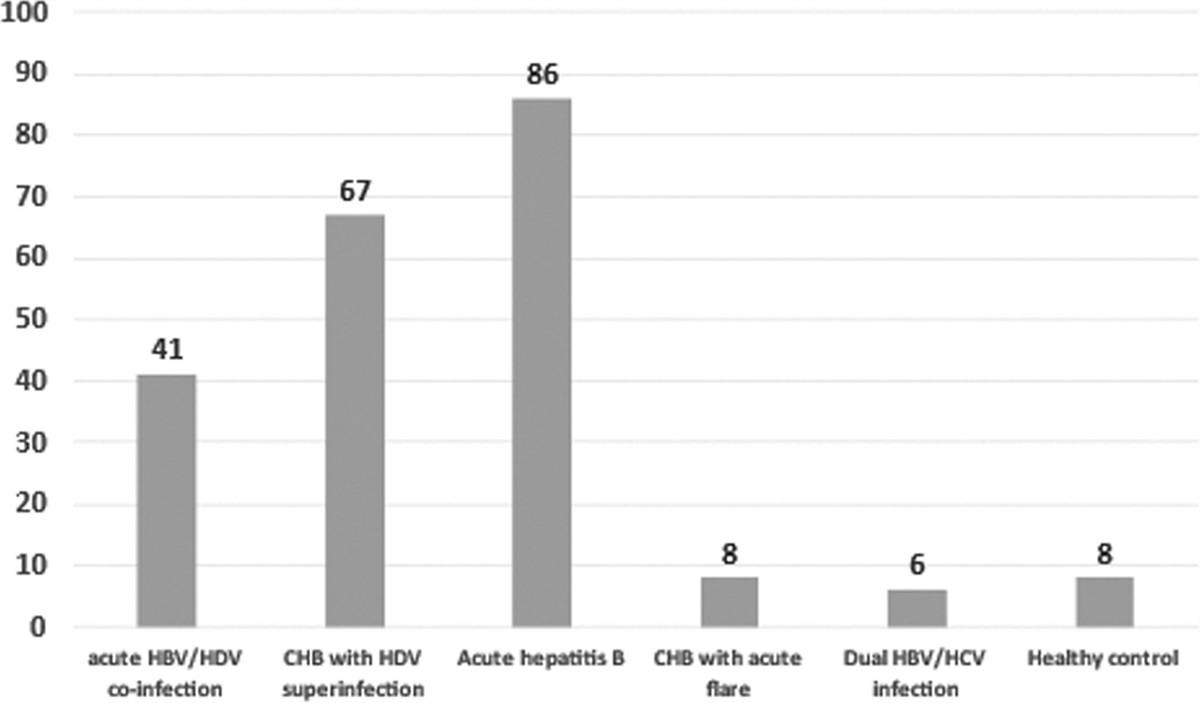
3. RESULTS 3.1. Demographic characteristics of the study cohort in MNUMSAmong 216 patients enrolled in the cohort from MNUMS, 116 were males and 100 were females. The mean age was 27.3 (SD 9.7) years. The number of patients in each diagnosis is shown in Fig. 1. For the final analysis, we enrolled 194 patients, including 86 with acute hepatitis B (AHB) and 108 with HBV and HDV dual infection. Among the patients with HBV and HDV infection, 41 had acute HBV and HDV coinfection and 67 patients had chronic hepatitis B (CHB) with HDV superinfection.
 Fig. 1:
Fig. 1: The number of subjects in each diagnosis. CHB = chronic hepatitis B; HBV = hepatitis B virus; HCV = hepatitis C virus; HDV = hepatitis D virus.
3.2. Comparison of demographic characteristics and potential transmission routes between acute hepatitis B and HBV/HDV dual infectionAs shown in Table 1, patients with HBV and HDV dual infection were older (28.6 ± 11.0 vs 25.5 ± 8.1 years, p = 0.030) and had lower rates of positive HBeAg in sera (21.4% vs 39.4%, p = 0.027) and lower rates of serum HBV DNA > 2000 IU/mL (43.6% vs 82.4%, p < 0.001) compared with those with AHB. Moreover, patients with HBV and HDV dual infection had a higher rate of having received dental treatment (59.4% vs 40.5%, p = 0.014) or injection therapy (64.2% vs 44.0%, p = 0.009) than their counterparts.
Table 1 - Comparison of demographic characteristics and potential transmission routes between patients with acute hepatitis B and patients with HBV/HDV dual infection Parameters All Acute hepatitis B HBV/HDV dual infections p (n = 194) (n = 86) (n = 108) Age, y (mean ± SD) 27.3 ± 9.9 25.5 ± 8.1 28.6 ± 11.0 0.030 Male, n (%) 105/89 (54.1/45.9) 40/46 (46.5/53.5) 65/43 (60.2/39.8) 0.079 HBeAg (+)/(−), n (%) 44/106 (29.3/70.7) 26/40 (39.4/60.6) 18/66 (21.4/78.6) 0.027 HBsAg, log10 IU/mLa 4.05, 3.09-4.45 3.98, 2.99-4.41 4.15, 3.09-4.50 0.820 HBsAg > 1000/≤1000 IU/mL, n (%) 126/36 (77.8/22.2) 51/17 (75.0/25.0) 75/19 (79.8/20.2) 0.595 HBsAg > 10 000/≤10 000 IU/mL, n (%) 85/77 (52.5/47.5) 32/36 (47.1/52.9) 53/41 (56.4/43.6) 0.311 HBV DNA, log10 IU/mLa 3.87, 2.69-5.07 4.62, 3.96-5.46 2.98, 2.58-4.43 0.868 HBV DNA > 2000/≤2000 IU/mL, n (%) 97/65 (59.9/40.1) 56/12 (82.4/17.6) 41/53 (43.6/56.4) <0.001 ALT, U/La 2073.6, 1394.5-2980.0 2181.2, 1372.6-2832.0 2008.5, 1400.8-3038.0 0.961 AST, U/La 1223.7,750.7-2196.0 1253.3, 823.8-2150.5 1157.6, 673.9-2315.5 0.703 Total bilirubin mg/dLa 7.08, 4.92-10.05 6.63, 4.92-9.26 7.75, 4.93-10.68 0.549 Albumin, g/dLa 4.02, 3.63-4.22 4.03, 3.59-4.20 3.99, 3.64-4.29 0.348 Platelet, ×1000/mm3a 217.0,164.7-268.0 220.0, 167.5-278.0 211.0, 161.0-265.8 0.667 Dental treatment (+)/(−), n (%) 97/93 (51.1/48.9) 34/50 (40.5/59.5) 63/43 (59.4/40.6) 0.014 Surgery (+)/(−), n (%) 57/136 (29.5/70.5) 20/66 (23.3/76.7) 37/70 (34.6/65.4) 0.120 Acupuncture (+)/(−), n (%) 20/172 (10.4/89.6) 6/79 (7.1/92.9) 14/93 (13.1/86.9) 0.263 Blood transfusion (+)/(−), n (%) 8/182 (4.2/95.8) 2/82 (2.4/97.6) 6/100 (5.7/94.3) 0.305 Blood donation (+)/(−), n (%) 12/179 (6.3/93.7) 4/82 (4.7/95.3) 8/97 (7.6/92.4) 0.588 Dialysis (+)/(−), n (%) 2/189 (1.0/99.0) 1/85 (1.2/98.8) 1/104 (1.0/99.0) 1.000 Tattoo (+)/(−), n (%) 44/148 (22.9/77.1) 21/65 (24.4/75.6) 23/83 (21.7/78.3) 0.785 Piercing (+)/(−), n (%) 51/143 (26.3/73.7) 22/64 (25.6/74.4) 29/79 (26.9/73.1) 0.972 Injection (+)/(−), n (%) 105/85 (55.3/44.7) 37/47 (44.0/56.0) 68/38 (64.2/35.8) 0.009 Shared syringe (+)/(−), n (%) 4/190 (2.1/97.9) 2/84 (2.3/97.7) 2/106 (1.9/98.1) 1.000 Shared toothbrush (+)/(−), n (%) 27/167 (13.9/86.1) 13/73 (15.1/84.9) 14/94 (13.0/87.0) 0.825 Shared razor (+)/(−), n (%) 49/143 (25.5/74.5) 28/57 (32.9/67.1) 21/86 (19.6/80.4) 0.053 Boiled syringe (+)/(−), n (%) 23/153 (13.1/86.9) 9/70 (11.4/88.6) 14/83 (14.4/85.6) 0.711 Mother HBV carrier (+)/(−), n (%) 21/109 (16.2/83.8) 7/56 (11.1/88.9) 14/53 (20.9/79.1) 0.202ALT = alanine aminotransferase; AST = aspartate aminotransferase; HBeAg = hepatitis B e antigen; HBsAg = hepatitis B surface antigen; HBV = hepatitis B virus; HDV = hepatitis D virus.
aExpressed as median, interquartile range.
Among the 108 patients with HBV and HDV dual infection, those with HBV/HDV coinfection had a higher rate of positive HBeAg in sera, a higher rate of serum HBV DNA > 2000 IU/mL but a lower rate of HDV viremia than those with HDV superinfection on CHB (Table 2). The potential transmission routes were similar between these two groups of patients.
Table 2 - Comparison of demographic characteristics and potential transmission route between HDV patients with HBV/HDV co-infection and HDV superinfection on chronic hepatitis B Parameters HBV/HDV co-infection HDV superinfection on CHB p (n = 41) (n = 67) Age, y (mean ± SD) 27.7 ± 0.9 29.2 ± 11.0 0.497 Male, n (%) 25/16 (61.0/39.0) 40/27 (59.7/40.3) 1.000 HBeAg (+)/(−), n (%) 13/21 (38.2/61.8) 5/45 (10.0/90.0) 0.005 HBsAg, log10 IU/mLa 4.05, 2.96-4.36 4.19, 3.17-4.54 0.521 HBsAg > 1000/≤1000 IU/mL, n (%) 28/10 (73.7/26.3) 47/9 (83.9/16.1) 0.341 HBV DNA, log10 IU/mLa 3.73, 3.02-4.65 2.67, 2.50-3.74 0.239 HBV DNA > 2000/≤2000 IU/mL, n (%) 25/13 (65.8/34.2) 16/40 (28.6/71.4) 0.001 HDV RNA (+)/(−), n (%) 21/17 (55.3/44.7) 50/6 (89.3/10.7) <0.001 HDV RNA log10 copies/mLa 3.50, 2.89-7.00 6.56, 5.31-7.93 0.239 ALT, U/La 1941.9, 1447.6-2609.3 2030.6, 1111.4-3457.1 0.134 AST, U/La 1097.1, 623.7-1897.7 1158.2, 685.3-2612.6 0.613 Total bilirubin, mg/dLa 8.34, 5.77-12.57 7.03, 4.54-10.04 0.155 Albumin, g/dLa 4.00, 3.20-4.18 3.97, 3.75-4.32 0.860 Platelet, ×1000/mm3a 220, 164.5-266 187, 160-267 0.171 Dental treatment (+)/(−), n (%) 17/22 (43.6/56.4) 46/21 (68.7/31.3) 0.020 Surgery (+)/(−), n (%) 14/26 (35.0/65.0) 23/44 (34.3/65.7) 1.000 Acupuncture (+)/(−), n (%) 4/36 (10.0/90.0) 10/57 (14.9/85.1) 0.664 Blood transfusion (+)/(−), n (%) 1/39 (2.5/97.5) 5/61 (7.6/92.4) 0.405 Blood donation (+)/(−), n (%) 3/36 (7.7/92.3) 5/61 (7.6/92.4) 1.000 Dialysis (+)/(−), n (%) 0/39 (0/100) 1/65 (1.5/98.5) 1.000 Tattoo (+)/(−), n (%) 8/32 (20.0/80.0) 15/51 (22.7/77.3) 0.931 Piercing (+)/(−), n (%) 12/29 (29.3/70.7) 17/50 (25.4/74.6) 0.826 Injection (+)/(−), n (%) 26/14 (65.0/35.0) 42/24 (63.6/36.4) 1.000 Shared syringe (+)/(−), n (%) 1/40 (2.4/97.6) 1/66 (1.5/98.5) 1.000 Shared toothbrush (+)/(−), n (%) 6/35 (14.6/85.4) 8/59 (11.9/88.1) 0.913 Shared razor (+)/(−), n (%) 12/29 (29.3/70.7) 9/57 (13.6/86.4) 0.084 Boiled syringe (+)/(−), n (%) 4/33 (10.8/89.2) 10/50 (16.7/83.3) 0.617 Mother HBV carrier (+)/(−), n (%) 4/22 (15.4/84.6) 10/31 (24.4/75.6) 0.565CHB = chronic hepatitis B; ALT = alanine aminotransferase; HBeAg = hepatitis B e antigen; HBsAg = hepatitis B surface antigen; HBV = hepatitis B virus; HDV = hepatitis D virus.
aExpressed as median, interquartile range.
Subsequently, we compared the demographic characteristics and the potential transmission routes between patients with AHB and those with HDV superinfection on CHB (Supplementary Table S2, https://links.lww.com/JCMA/A241). The results showed that patients with HDV superinfection were older, had a lower rate of positive HBeAg in sera, a lower rate of serum HBV DNA > 2000 IU/mL, a higher rate of having received dental treatment and injection therapy, but a lower rate of shared razor than those with AHB.
In addition, the demographic characteristics, HBV viral factors, and risk factors were comparable between patients with AHB and those with acute HBV/HDV coinfection, except that coinfection patients had a higher rate of having received injection therapy (Supplementary Table S3, https://links.lww.com/JCMA/A241).
3.3. The risk factors and clinical manifestations associated with HDV viremiaAmong the 94 patients with HBV/HDV dual infection and with available HDV RNA data, 71 (75.5%) had positive HDV RNA in sera, and the remaining 23 (24.5%) did not have HDV viremia tested by real time polymerase chain reaction (RT-PCR). All of these patients were infected by genotype 1 HDV; genotypes C and D were the major genotypes of HBV infection.
As shown in Supplementary Table S4, https://links.lww.com/JCMA/A241, the potential risk factors were comparable between patients with and without HDV viremia. Also, the clinical manifestations were similar between the two groups of patients, except that patients with HDV viremia had a lower rate of serum HBV DNA > 2000 IU/mL but had higher serum ALT levels than their counterparts.
3.4. Infection control workshop and preventive strategiesDuring the site visits to Mongolia, we found that neither dentists nor patients had adequate protection (Supplementary Fig. 1, https://links.lww.com/JCMA/A239), and dental chair tables and buttons lacked protective covers that should be changed for every patient. Although disposable needles and syringes were used in the medical center and provincial hospital, the situation in small private clinics was unclear. Moreover, safe needles were not used, even in medical centers and provincial hospitals. Multivariate analyses indicated dental procedures and injections were significantly associated with acute HDV infection, supporting the observations from the site visit. Therefore, we organized two 5-day infection control workshops, including lectures and site visits to different clinical departments at the Taipei Veterans General Hospital (one of the two national medical centers in Taiwan), the Cathay General Hospital (a private medical center), and the Center for Disease Control (CDC) in Taiwan (Supplementary Tables 5 and 6, https://links.lww.com/JCMA/A241). The infection control workshop included comprehensive courses, not only for viral hepatitis but also for the prevention and control of airborne infectious diseases (Supplementary Tables 1 and 2, https://links.lww.com/JCMA/A241). The trainees were exclusively experienced Mongolian medical personnel (doctors, dentists, nurses, and experts in infectious diseases), officers of the Health Authority and Department of Health, and members of parliament. A total of 19 seed teachers of infection control participated in the infection control workshop. After their return to Mongolia, they trained another 400-plus personnel who are in charge of infection control.
3.5. Secular changes in the diagnosis and mortality of HDV infection in MongoliaFrom 2011 to 2021, a total of 884 patients were diagnosed with HDV infection in NCCD, Mongolia (Fig. 2). Data stratified by the time period of HDV diagnosis showed that cases of newly diagnosed HDV infection were more prevalent between 2011 and 2015 (111.20 ± 29.79 cases/y) and declined to 54.67 ± 27.34 cases/y between 2016 and 2021 (p = 0.010). Moreover, the incidence rate of HDV infection also decreased from 0.38 ± 0.13 per 100 000 per year between 2011 and 2015 to 0.19 ± 0.10 per 100 000 per year between 2016 and 2021 (p = 0.025).
 Fig. 2:
Fig. 2: Secular changes of HDV infection in Mongolia. New case (A) and incidence rates (B) of HDV infection in NCCD, Mongolia. HDV = hepatitis D virus; NCCD = National Center for Communicable Disease.
4. DISCUSSIONOur study had several major findings. First, the incidence rate of HDV infection in Mongolia has declined in recent years. However, the patients with HDV infection were young, with a mean age of 28.6 years. Second, patients with HBV/HDV dual infections had a significantly higher rate of having received dental treatment and injection therapy compared with those with AHB.
Mongolia has the highest prevalence of HCC in the world.17 However, most patients are diagnosed with HCC at an advanced stage. Baatarkhuu et al23 showed that only 12.3% of patients with HCC in Mongolia were at the Barcelona Clinic Liver Cancer (BCLC) stage A. Hence, the outcomes of Mongolian HCC patients were very poor, with 3- and 5-year overall survival rates of 9.5% and 1.3%, respectively. Viral hepatitis is the major etiology of liver cirrhosis and HCC in Mongolia.23,25 Moreover, HCC in Mongolia seems to have unique genomic characteristics and driver genes, such as SPTA1, which is associated with HDV infection.34,35 This suggests a close link between HDV infection and HCC in Mongolia. It is crucial to implement preventive strategies for HDV infection to reduce the prevalence of HCC in Mongolia.
A nationwide HBV immunization program for all newborn babies was launched in Mongolia in 1991. There was little breakthrough infection due to the presence of immune-escape HBV mutant in the follow-up study in vaccinated children by Ijaz et al36; however, 85% of the vaccinated children had anti-HBs titers less than 100 IU/L, 46% of whom had levels less than 10 IU/L. In our current study, the mean age of the patients was 25.5 and 28.6 years for patients with AHB and HBV/HDV dual infections, respectively. This indicates that most of them might have received HBV vaccination at birth. However, they still bore a risk of acquiring acute HBV infection or developing CHB, and some got an HBV/HDV dual infection. This might be attributed to a few factors. First, the coverage rate of the HBV vaccine in Mongolia remains unsatisfactory. Davaalkham et al37 showed that the rate of complete HBV vaccination in Mongolia was only 60.1%. Of note, the coverage rates were 55.7% and 59.1% in the province centers and rural areas, respectively, which was significantly lower than that of 75.2% in the metropolitan regions. There is still room to increase the coverage rate of the HBV vaccine in Mongolia.
Second, there is concern that the protective effects of the HBV vaccine might not be optimal in preventing HBV infection in the Mongolian population. One previous survey in Mongolia showed that about 16.2% of immunized children were positive for anti-HBc, and 9.3% had positive HBsAg and/or HBV DNA in sera.38 Thus, the anti-HBs titers might not be persistently high enough to protect individuals from HBV infection. It is crucial to elucidate the risk factors associated with HBV vaccine failure in Mongolian subjects born after the HBV vaccine era. In Taiwan, testing of anti-HBs titers for 1-year-old children of HBV-carrier mothers is routinely carried out, and supplementary HBV vaccines are provided for those with anti-HBs <10 IU/mL. We suggested that our Mongolian collaborators recommend that their government adopt the same strategy. HBV vaccine is relatively heat-stable but vulnerable to extremely cold temperatures. One study reported that freezing temperatures during provincial-to-rural vaccine transportation destroys HBV vaccine and may account for the poor vaccine response in the Mongolian countryside.39 The suboptimal temperatures of the HBV vaccine during storage and delivery might also be an important cause of vaccine failure in Mongolia. A more effective strategy, such as a cold chain system for storage and delivery, may improve the efficacy of HBV vaccine immunization. In addition, catch-up vaccination for the children of HBV-carrier mothers at 1 year old or in preschool may be needed to keep anti-HBs titers at protective levels in children. Also, the prescription of antiviral therapy for high HBV viremia pregnant women could interrupt the risk of mother-to-infant vertical transmission of HBV for newborns.40 Hopefully, the prevalence of HBV and HDV infection could decrease significantly through these efforts in the near future.
Of note, our study disclosed that dental treatments and injections were associated with a higher risk of individuals acquiring HDV infection. This suggests that the current disinfection methods and infection control strategy in Mongolia cannot effectively prevent the spread of HDV. In 2016, we joined with the experts from Mongolia to form a collaborative team to observe infection control programs in hospitals, dental clinics, and local clinics. We found that neither dentists nor patients had protective face masks or surgery hole towels for use during dental procedures, and the dental chairs and instruments did not have protective membranes to be changed between patients or adequate disinfection, as the dentists of Taiwan do. Data on sexual exposure to new contacts were missing because the participating patients were reluctant to disclose this history. However, the high prevalence of viral hepatitis B, C, and D in Mongolia and surprisingly high prevalence of hepatitis B and C virus infection in nurses of a tertiary hospital in Mongolia suggests that iatrogenic causes are the most likely sources for the high prevalence of hepatitis D infection in Mongolia.41 After the visits, we recommended some strategies and arranged infection control workshops in Taiwan and Mongolia to decrease the risk of HDV infection from these important transmission routes. Our study disclosed that the rate of HDV infection had declined in recent years, probably due to collective efforts and more strict infection control implemented in 2019 with the COVID-19 pandemic (Fig. 2). Hopefully, the incidence and prevalence of HDV infection will decrease more substantially in the near future through the collaborative efforts and strategies.
In Taiwan, the incidence of HDV infection has been markedly reduced via continuous and widespread education by mass media and medical societies.15 Our previous study indicated that acute HDV infection decreased from 15% before 1999 to 1.6% in HBeAg-positive CHB with acute exacerbation (AE) and 5.4% in HBeAg-negative CHB with AE.13,42,43 Moreover, the rate of HDV infection was about 4.4% in the general population of patients with CHB.13 In fact, there have been very few new acute HDV infections since 1995, as evidenced by our study and the annual report of the Ministry of Health and Welfare of Taiwan.14,15 Nevertheless, the prevalence of HDV infection in IDUs was 63.0% and rose to 74.9% in HIV-infected IDUs. Of note, in the HIV cohort born after 1987 who were HBsAg-negative, over half (52.9%) had anti-HBs Ab levels of <10 mIU/mL, and there was a significantly higher HBsAg seroprevalence in the HIV cohort compared with the control group (8.1% vs 0.0%, p = 0.02). In the era of HBV vaccination, IDU and HIV-infected individuals have been high-risk groups and a reservoir for HDV infection. HBV vaccinations and boosters are highly recommended to these high-risk groups, and catch-up vaccinations were approved after our proposal based on evidence-based study became the preventive policy in Taiwan in 2023.13 Because IDUs are repeatedly exposed to injections with inadequately disinfected and reused needles, the risk of HBV infection is much higher than in general population. The immuno-suppressed status due to HIV infection results in a higher chronicity rate of acute HBV infection, which, in turn, results in higher rates of HDV superinfection and the progression of HDV superinfection to chronic hepatitis D. Of note, these high-risk groups are both HBV and HDV reservoirs and may spread these viruses to the general population. In contrast to more effective HIV and HCV therapy, there has been no effective treatment with long-term sustained virological response for CHD until recently.3,44–46 Many members of these high-risk groups may die of CHD and its sequelae. Prevention is, thus, crucial. Our study suggests that the implementation of HBV vaccination and booster vaccines among these high-risk groups is an essential strategy and is worthy of consideration from Taiwan and the world, including Mongolia.
Recent decades have seen much improvement in the immunization coverage rate (post-2000), utilization of single-use needles (but not safe needles) and syringes (since 1995), catch-up HBV vaccinations in health workers (since 1996), and blood donor screening for HBsAg and anti-HCV (since 1997), etc. However, the hepatitis reporting system covers only acute jaundice cases; transmissions via medical injections, dental procedures, and invasive surgery are still issues to be improved; and occupational accidental exposures are still common in Mongolia. Although hospitals up to the district level have designated infection control practitioners and guidelines from the Ministry of Health and Sports, several studies have indicated that the management of the system is weak for various reasons. More updated epidemiology data are urgently needed. Injections are over-prescribed, safe needles are rare, disposal boxes are not universally available, and surgical (in particular, obstetrics and gynecology) and dental practices in private clinics do not practice appropriate infection control. These factors still account for some HDV infections, and transmission routes remain obscure in many HDV infections.17 Taiwan was the first country to implement a national HBV vaccination program (in 1984), to screen blood donors and for use of disposable needles, to establish an acute hepatitis reporting system, and to implement national insurance reimbursement for the treatment of hepatitis B and C. Medical centers and hospitals in Taiwan receive strict infection control inspections and evaluations regularly. These experiences may be of value in controlling viral hepatitis and other communicable diseases in Mongolia.
There are still several limitations in this study. First, sexual transmission is an important r
留言 (0)