Herein, we report our institutional experience with the recently introduced integrated molecular-morphological risk classifier for meningiomas [10]. We specifically focused our analysis on grade 2 meningiomas as they comprise a particularly challenging entity with a board variety of clinical courses and limited in-depth data available [4, 6, 7, 24]. The current management of grade 2 meningiomas is primarily based on a safe surgical resection [2]. Then, however, controversies remain regarding the role of adjuvant radiotherapy, particularly in the setting of a gross total resection. According to the recommendations of the European Association of Neuro-Oncology, adjuvant radiotherapy is advised for patients with subtotal resection and an option besides observation after gross total resection [2]. In the light of our observed results, several topics should be addressed. Besides the logistical, financial, and technical requirements of the classifier, i.e., lab infrastructure, technicians, and consumables, its clinical relevance is of particular importance as seen in the reported results. As histological grading may ideally reflect the biological behavior and aggressiveness of tumors, one would assume that histologically defined grade 2 meningiomas mostly display a disease course comparable to tumors that match the criteria of the intermediate risk group as defined by the integrated molecular-morphological risk classifier [10].
The likelihood of patients in this cohort having a meningioma with an intermediate risk profile as suggested by a grade 2 histology, however, was only around 50%. This finding has significant implications for the management of such tumors and highlights the urgent need for the routine implementation of integrated and molecular classifiers. Histopathological grading alone is not sufficient to adequately predict the biological behavior and to guide individual treatment decision-making. The time of local control differed substantially between all three integrated risk groups, most notably between the low risk group (5-year rate: 91.8%) and high risk group (5-year rate: 40.2%). The multivariable Cox regression confirmed the importance of the risk group assignment for local control. Such differences are critical and information from the integrated molecular-morphological risk score will substantially help to counsel patients and guide treatment-related discussions. Considering that all tumors were classified as grade 2 meningiomas according to the current WHO tumor classification, the considerable variety of observed disease courses and risk of disease progression cannot be unmasked by histopathology alone.
This may be of particular relevance for treatment individualization and the implementation of postoperative radiotherapy, an ongoing topic of debate with several, partially contradicting studies published [6, 7, 24]. Previous work investigating the role of radiotherapy in grade 2 meningiomas did not routinely incorporate molecular characteristics, such as methylation profiling and CNV, thereby limiting the comparability of cohorts as biologically and genetically heterogeneous tumors may have been analyzed [9, 10]. Herein, the use of the integrated molecular-morphological risk classifier would have had significant implications for the clinical management of affected patients. A total of only 15 patients in our cohort received adjuvant radiotherapy, reflecting the ongoing uncertainty regarding the regular use of postoperative treatment of grade 2 meningiomas over the past years [2, 25]. The use of the integrated molecular-morphological risk classifier revealed that four of these patients (26.6%) receiving radiotherapy had a low risk of tumor progression, an insight which could have influenced the patients’ decision making. In total, information of the classifier could have informed the treatment decision making process concerning radiotherapy in over 60% of cases. Moreover, the assumed biological behavior of tumors can also be utilized to adjust the follow-up intervals. High risk tumors warrant close monitoring while low risk grade 2 meningiomas may not necessarily need follow-up every six months as suggested by current guidelines [2]. A risk-adapted management could, therefore, reduce the socioeconomic burden on patients, physicians, and healthcare systems.
These clinical implications highlight the necessity of further investigations, particularly concerning the role of the risk-adapted use of adjuvant radiotherapy. Two prospective interventional studies are aiming to ultimately define the role of adjuvant radiotherapy in grade 2 meningiomas after gross total resection. The two trials, the EORTC 1308/ROAM and NRG BN003, however, have been set up using histopathological criteria, i.e., grading, alone to assess tumor aggressiveness [8]. Our results strongly indicate that molecular-based risk stratification of tumors is highly advisable to study homogeneous patient cohorts. Only by doing so, one can adequately assess the efficacy and safety of an experimental treatment. Therefore, retrospective molecular work-up should be considered to determine the actual biological aggressiveness of the included tumors as suggested by others [26]. Thus, future meningioma trials should consider the use of molecular characteristics to stratify patients in the first place to improve comparability and cohort homogeneity [13].
While the assessment of the methylation profile and incorporation of CNV and histopathological grading have proven valuable in determining the biological aggressiveness and recurrence risk of meningiomas, the broad and consistent implementation of the integrated molecular classifier is resource-intensive [10]. Therefore, alternative methods and prognostic markers that are cost-effective and comparably sensitive are needed. Specific CNV can be a potential solution. Herein, the 1p status demonstrated an excellent correlation with the risk stratification of low and intermediate/high risk tumors per integrated risk grouping (Additional file 1: Fig. S2). This is in accordance with recent analyses, including a retrospective evaluation of patients enrolled in the EORTC 22042–26042 trial [10, 27,28,29]. This growing evidence should be considered and validated in future research, particularly in prospective clinical trials. While several integrated molecular classifiers for meningiomas exist, there is a distinct need for classifier harmonization and further investigations in distinct subgroups like grad 2 tumors [13].
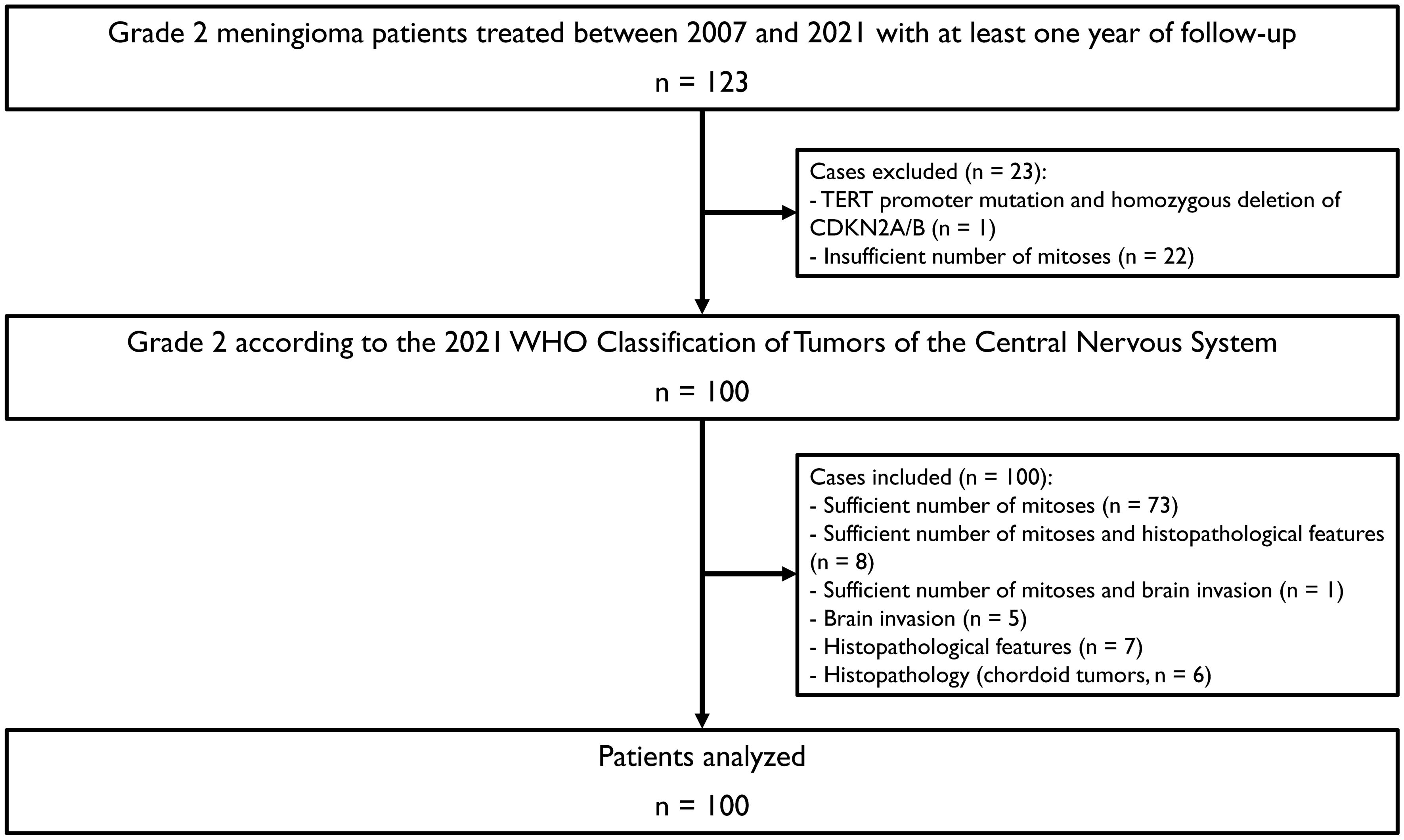
Moreover, risk factors beyond the methylation class and CNV are well known, such as TERT promoter mutations or homozygous and heterozygous deletions of CDKN2A/B [17, 30,31,32,33]. However, the distinct frequencies of such genetic risk factors in the subgroup of grade 2 meningiomas remain of interest. The optimal approaches when to determine these markers are still not clear or debatable [21]. Herein, we screened histologically defined grade 2 meningiomas and only found one TERT promoter mutation and one homozygous CDKN2A/B deletion during our molecular testing (< 1% of analyzed tumors). Notably, both alterations were found in the same high risk tumor (methylation family malignant) which recurred locally only 7.4 months after initial resection. The reported frequency of TERT promoter mutations in histopathologically defined grade 2 tumors was noticeably higher with 5.7% [30]. Likewise, the rate of homozygous CDKN2A/B deletions was approximately 7% in grade 2 meningiomas in another cohort [9, 21]. However, it is important to acknowledge that the observed differences may be attributed to variations in the application of different WHO tumor classifications. In particular, we had to exclude 22 tumors (22/123, 17.8%) during our grading reassessment due to an insufficient number of mitoses, as the specific microscope field size used for assessment must be taken into consideration according to the WHO 2021 classification.
As we have not identified any TERT promoter mutation or homozygous CDKN2A/B deletion in the full intermediate risk group meningiomas (62 cases, data not shown), we share the view of Hielscher and colleagues and do not recommend routine testing for TERT promoter mutations or dedicated assessment of homozygous CDKN2A/B deletions, the latter especially in the absence of methylation analysis [21]. Another topic of interest is the use of different methylation family classifiers, namely the brain tumor classifier v12.5 and the meningioma classifier v2.4. As the methylation family has impact on the final risk group according to the integrated molecular-morphological risk score, its classification is particularly important [10]. We tested both classifiers and found minor differences concerning the subgroups benign and intermediate (Additional file 1: Figs. S11 and 12). However, differences were small and in the final risk group assessment, only six cases differed (6.0%). This finding is in general agreement with previous studies [21]. Therefore, both methylation family classifiers may be used as the chance of a clinically meaningful difference between classifiers is low.
As multiple different genetic and molecular classifiers for meningiomas have been introduced, it will be crucial to combine their characteristics and advantages to ultimately establish one comprehensive classifier which can be prospectively validated and routinely implemented [13]. Meningiomas remain a challenging tumor entity, especially in case of grade 2 and 3 tumors and in the absence of established targeted therapies [2, 3]. The need for treatment individualization remains with various unanswered questions, especially concerning the use of radiotherapy (timing, dose escalation, safety margins, functional imaging for target delineation). This work highlights the fundamental role of the integrated molecular-morphological risk score to unravel and clinically stratify the heterogenous group of grade 2 meningiomas into risk groups. As a consequence of our observed findings, we aim to prospectively integrate risk stratification into daily clinical routine to guide our treatment, patient counseling, and follow-up schedules. Nevertheless, this study has limitations, pertinent to its design. First, the retrospective nature and single-center design of this work may have influenced the included samples and data quality as some clinical data were missing, e.g., the resection status in 8 cases. Moreover, the decision of using adjuvant radiotherapy in this patient cohort was most likely affected by distinct patient preferences or tumor characteristics, e.g., subtotal resection. In addition, the relative lack of patients receiving radiotherapy impairs the adequate assessment of the effect on local control in a homogeneous subgroup. Finally, a longer follow-up is necessary to confirm the long-term implications of the classifier.



留言 (0)