
記住我



The link between inflammation and heart disease is well-established. Inflammation and heart disease, however, come in different flavors. Chronic, low-grade inflammation predicts and promotes atherothrombotic events.1 Acute injury to the heart, such as an acute myocardial infarction, induces a local and systemic inflammatory response.2,3 In autoimmune disease, persistent, unresolving inflammation causes injury to the cardiovascular structures.4 In a few instances, the causes for injury or inflammation are obvious, ie, acute myocardial infarction, whereas in most cases, the causes of low-grade chronic smoldering inflammation or nonresolving inflammation are not known. Occasionally, the treatments for inflammation or other conditions, such as cancer, become themselves the cause of cardiovascular injury and inflammation.
The terms cardioimmunology and cardiorheumatology have been used to indicate the fields of research and practice related to immunology, cardiology, and rheumatology (Fig. 1).5–.7 The principles of immunology, ie, the cellular and humoral components of the inflammatory response, are used to investigate and understand how these inflammatory reactive and reparative mechanisms and potentially dysregulated responses can become injurious and detrimental, causing cardiovascular diseases. The classic examples of inflammation becoming the mechanism of disease are postviral myocarditis and pericarditis, in which an initial viral injury and/or antigen molecular mimicry triggers inappropriate persistent inflammation in the heart muscle or pericardium, respectively. However, the connection between inflammation and cardiovascular dysfunction can be part of a systemic, immune-mediated disease. Patients with chronic systemic autoimmune diseases are, in fact, at risk of both direct, disease-related immunological injury to the cardiovascular system and iatrogenic toxicity driven by prescribed treatments. A classic example of cardiovascular effects of rheumatologic disease is systemic lupus erythematosus, in which an autoimmune response to the heart and vascular structures can promote atherothrombotic complications and/or cause both overt autoimmune myocarditis and chronic cardiac damage, and at the same time, prednisone, which is commonly used for its treatment, causes an increased cardiovascular risk. The term cardiorheumatology has been used to refer to the study of how inflammation affects cardiovascular health in the context of connective tissue disorders.7
 FIGURE 1.:
FIGURE 1.: Immunology, cardiology, and rheumatology. Schematic representation of how the study of inflammation contributes to the pathophysiology of cardiovascular diseases and on how systemic inflammatory illnesses or their management affect cardiovascular health and diseases may be viewed as a combination of the fields of immunology, cardiology, and rheumatology.
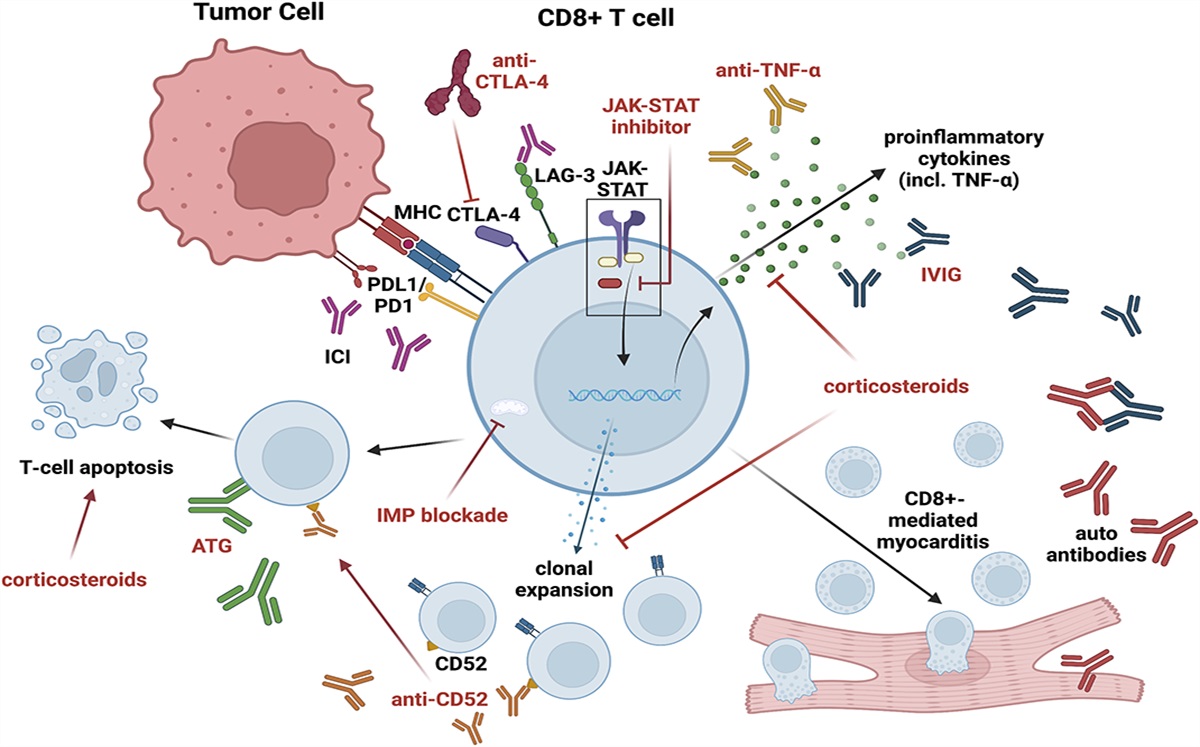
In this issue of the Journal of Cardiovascular Pharmacology, experts in the fields of cardiology, immunology, and rheumatology present an overview of the novelty in the fields. Ferone et al8 from London, United Kingdom, discuss current treatment and immunomodulatory strategies in myocarditis. Despite the long-standing recognition of the syndrome of acute and chronic myocarditis, the treatment remains largely supportive and empirical. Randomized clinical trials are few, and they have largely failed to show efficacy that is consistent across trials. Heemelaar et al9 from Boston, MA, address a specific form of acute myocarditis associated with the use of immune checkpoint inhibitors. In these cases, treatments aimed at inducing an immune response to cancer cells occasionally result in autoimmune reactions to the myocardium, causing heart failure, shock, and life-threatening arrhythmias.
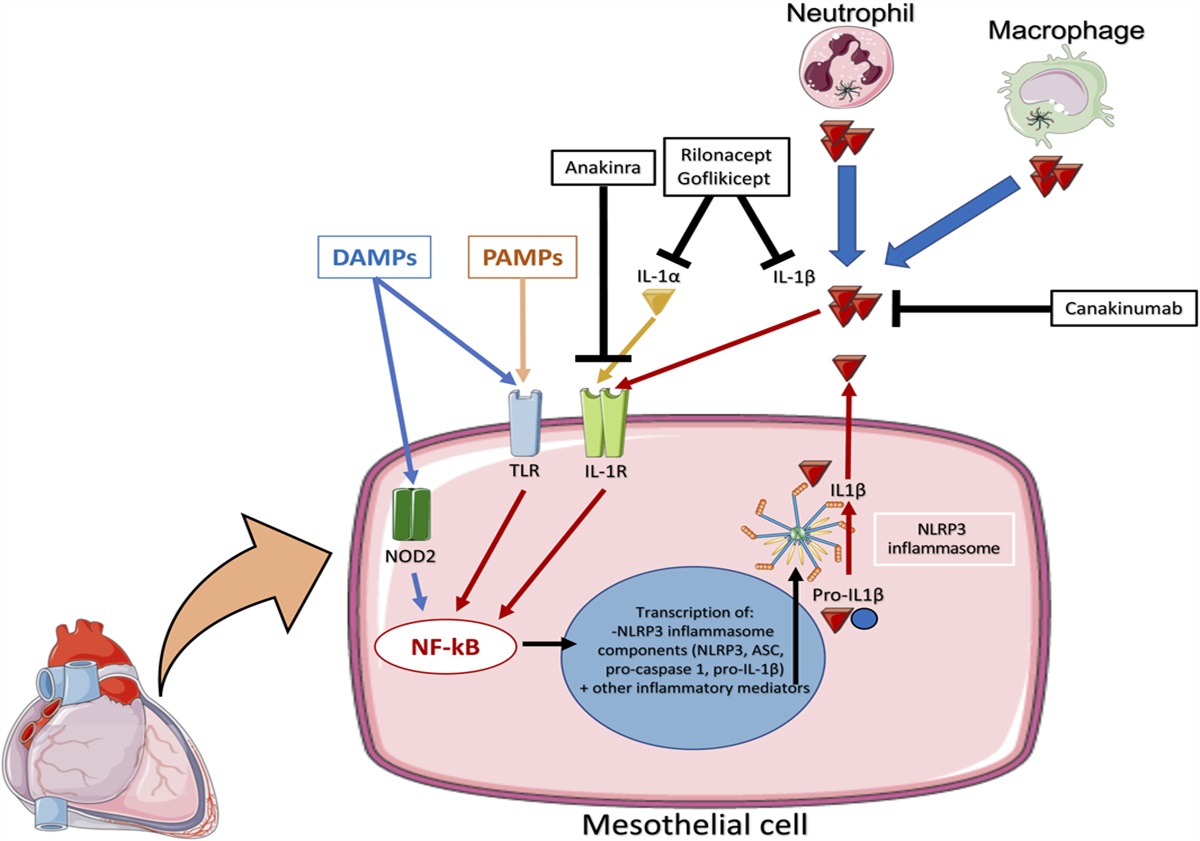
Vecchiè et al10 from Varese, Italy, review the novel therapeutic insights into the treatment of pericarditis. Recent data from experimental and clinical studies have indeed highlighted the central role of innate immunity in recurrent pericarditis. The activation of the inflammasome and release of interleukin-1 (IL-1) β and IL-1α seem central to the autoinflammatory loop seen in recurrent pericarditis, independent of the inciting event. Along these lines, Thomas et al11 from Richmond, VA, review the role of IL-1 blockers in the treatment of recurrent pericarditis and particularly how interrupting the autoinflammatory mechanism affects patient quality of life. Pericarditis can, however, be a symptom and sign of a systemic rheumatologic disease. Kawano et al12 from Boston, MA, discuss how patients with pericarditis associated with rheumatologic diseases should be evaluated and managed.
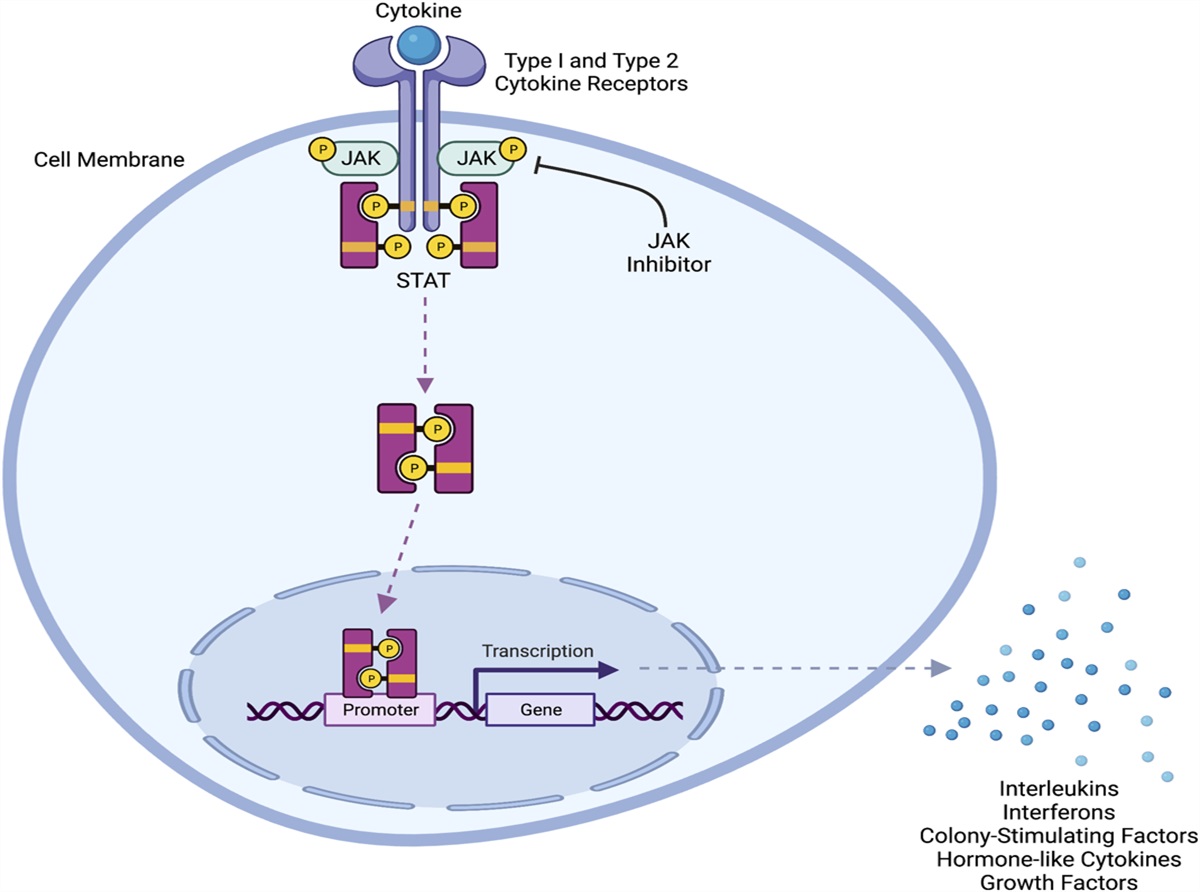
Systemic inflammation also carries consequences for atherothrombosis, as well as for heart failure and kidney failure. The clinical trials with canakinumab and colchicine demonstrate that targeting inflammation with an IL-1β blocker (canakinumab) or an inhibitor of tubulin polymer formation and nonselective inflammasome inhibitor (colchicine) prevents recurrent atherothrombotic events.2,3 In this issue, Jaffree et al13 from Richmond, VA, address the central role of IL-1 in the development and progression of heart failure. A subanalysis of the canakinumab trial and several phase II trials with anakinra, a recombinant IL-1 receptor antagonist, demonstrate that blocking IL-1 has beneficial effects in heart failure.14,15 Huck et al16 from Boston, MA, review the evolving data regarding targeting pharmacotherapies for inflammatory and cardiorenal endpoints in kidney disease. Finally, Shah et al17 from New York, NY, address cardiovascular risk management in patients treated with Janus kinase inhibitors, known to promote arterial and venous thrombotic events.
Although not a comprehensive list, these reports show the breadth and complexity of addressing inflammation as a marker and mediator of risk for cardiovascular diseases. The recent approval of colchicine to reduce the risk of myocardial infarction, stroke, coronary revascularization, and cardiovascular death in adult patients with established atherosclerotic disease or with multiple risk factors of cardiovascular disease by the US Food and Drug Administration in 202318 marks an important step forward in Cardiology by establishing a novel paradigm shift by which inhibiting inflammation is as important and synergistic to treating other established clinical risk factors. For cardioimmunologists, the time is prime for clinical trials of targeted immunomodulatory drugs to prevent or treat cardiovascular diseases. For cardiorheumatologists, understanding the mechanism of cardiac involvement and/or toxicity will be necessary to guide disease-modifying therapies that can reduce cardiovascular risk in patients with systemic rheumatologic diseases. And as we move forward, the boundaries between cardiorheumatology and cardioimmunology will likely fade because both terms refer to the study of the interaction between the immune and cardiovascular system, with the ultimate goal of understanding and treating cardiovascular disease. There are numerous ongoing clinical trials using various anti-inflammatory drugs, and we eagerly await their results to better understand disease processes and optimize clinical care.
1. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105:1135–1143. 2. Abbate A, Toldo S, Marchetti C, et al. Interleukin-1 and the inflammasome as therapeutic Targets in cardiovascular disease. Circ Res. 2020;126:1260–1280. 3. Toldo S, Abbate A. The role of the NLRP3 inflammasome and pyroptosis in cardiovascular diseases. Nat Rev Cardiol. 2023. doi:10.1038/s41569-023-00946-3. 37923829. 4. Weber BN, Garshick M, Abbate A, et al. Acute cardiovascular complications of immune-mediated systemic inflammatory diseases. Eur Heart J Acute Cardiovasc Care. 2023;12:792–801. 5. Cohen CD, Rousseau ST, Bermea KC, et al. Myocardial immune cells: the Basis of cardiac immunology. J Immunol. 2023;210:1198–1207. 6. Swirski FK, Nahrendorf M. Cardioimmunology: the immune system in cardiac homeostasis and disease. Nat Rev Immunol. 2018;18:733–744. 7. Weber B, Garshick M, Liao KP, et al. Sore, hot, and at risk: the emerging specialty of cardio-rheumatology. J Am Heart Assoc. 2023;12:e027846. 8. Ferone E, Segev A, Tempo E, et al. Current treatment and immunomodulation strategies in myocarditis. J Cardiovasc Pharmacol. 2024. In press. 9. Heemelaar JC, Antoni ML, Neilan TG. Review: Treatment of immune checkpoint inhibitor-associated myocarditis. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001456. Epub ahead of print. 10. Vecchiè A, Bonaventura A, Golino M, et al. Novel therapeutic insights into the treatment of pericarditis: targeting the innate immune system. J Cardiovasc Pharmacol. 2024. Current issue. 11. Thomas GK, Bonaventura A, Vecchié A, et al. Interleukin-1 blockers for the treatment of recurrent pericarditis: pathophysiology, patient reported outcomes and perspectives. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001435. Epub ahead of print. 12. Kawano Y, Pabón MA, Feldman CH, et al. Evaluation and management of pericarditis in rheumatic diseases. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001494. Epub ahead of print. 13. Jafree E, Del Buono MG, Canada JM, et al. Interleukin-1 inhibition for the prevention and treatment of heart failure. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001497. Epub ahead of print. 14. Trankle CR, Canada JM, Cei L, et al. Usefulness of canakinumab to improve exercise capacity in patients with long-term systolic heart failure and elevated C-reactive Protein. Am J Cardiol. 2018;122:1366–1370. 15. Everett BM, Cornel JH, Lainscak M, et al. Anti-inflammatory Therapy with canakinumab for the prevention of Hospitalization for heart failure. Circulation. 2019;139:1289–1299. 16. Huck DM, Buckley LF, Chandraker A, et al. Targeting pharmacotherapies for inflammatory and cardiorenal endpoints in kidney disease. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001482. Epub ahead of print. 17. Shah JT, Shah KT, Femia AN, et al. Cardiovascular risk management in patients treated with JAK inhibitors. J Cardiovasc Pharmacol. 2023. doi: 10.1097/FJC.0000000000001470. Epub ahead of print. 18. AGEPHA Pharma FZ L. LODOCO Prescribing Information. 2023. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215727s000lbl.pdf. Accessed December 7, 2023.
留言 (0)