
記住我





The Dieulafoy arteriole in the submucosa can be exposed to the surface due to atrophy or thinning of the mucosa from various causes such as ischemia, radiation, and senility. Rectal Dieulafoy accounts for 2% of all gastrointestinal Dieulafoy bleeding, but can present with massive hemorrhage in up to 47% of cases.1 Because of the intermittent bleeding and lack of an ulcerated bed, identification of the lesion can be challenging on endoscopy and often multiple colonoscopies are required.2 Various endotherapy modalities were reported in the literature with a primary hemostasis success up to 87%.1,3–5 We report a case of recurrent rectal Dieulafoy bleeding despite multiple conventional endoscopic treatments, which subsequently responded to endoscopic ultrasound (EUS)-guided coil embolization of the feeding arteriole.
CASE REPORTAn 87-year-old man with history of cirrhosis and hepatocellular carcinoma (HCC) with partial hepatectomy and multiple transarterial embolization (TACE) sessions presented with recurrent hematochezia. He also had rectal cancer status post low anterior resection with primary end-to-end colorectal anastomosis and local radiation therapy 14 years ago. He had an unremarkable upper endoscopy (EGD). Colonoscopy on the first bleeding episode revealed brisk bleeding at the colorectal anastomosis (Figure 1). There was no ulceration, visible vessel, rectal varices, or radiation-induced proctitis. The bleeding sites, which occurred at above and below the anastomosis, were treated successfully with epinephrine injection followed by endoclipping. The patient was discharged, but came back on multiple occasions subsequently due to recurrent significant rectal bleeding. There was a 10-month lapse between the first and last episodes of profuse rectal bleeding. Rebleeding occurred at an average of a 5–6-week interval; hemoglobin drop on the first episode was 12.0 to 8.9 gm/dL and 11.0 to 8.5 on the last episode. Each time he was treated endoscopically with epinephrine injection, argon plasma coagulation, endoclips placement, and/or bipolar cautery. He had a total of 4 colonoscopies and 5 sigmoidoscopies as well as 9 packed RBC transfusions. Owing to his comorbidities and advanced age, the surgical option was not recommended. We could attempt endoscopic suturing, but the mucosa was friable and the wall was fibrotic due to previous surgery and radiation. On endoscopy, bleeding was seen from a nonulcerated area in the vicinity of the colorectal anastomosis, which was not treated previously (Figure 2). A decision was made to proceed with EUS evaluation for possible coil embolization. Multiple Dieulafoy vessels were seen closely underneath the rectal mucosa in the bleeding area (Figure 3). A feeding Dieulafoy arteriole was identified on sonography with a typical arterial Doppler pattern and was punctured with a 22-gauge fine-needle aspiration needle and then was embolized with 2 coils (Nester Embolization Coil, 0.018 in diameter-2 cm length, by Cook Medical) (Figures 3 and 4). Cessation of blood flow in the feeding arteriole and peripheral vessels was observed on Doppler (Figure 5). Endoscopy confirmed a complete hemostatic effect (Figure 6). The site and source of active bleeding as well as the cessation of hemorrhage after coil embolization were visualized endoscopically. Since the EUS guided coil embolization, there was no further recurrent rectal bleeding event for more than 6 months.
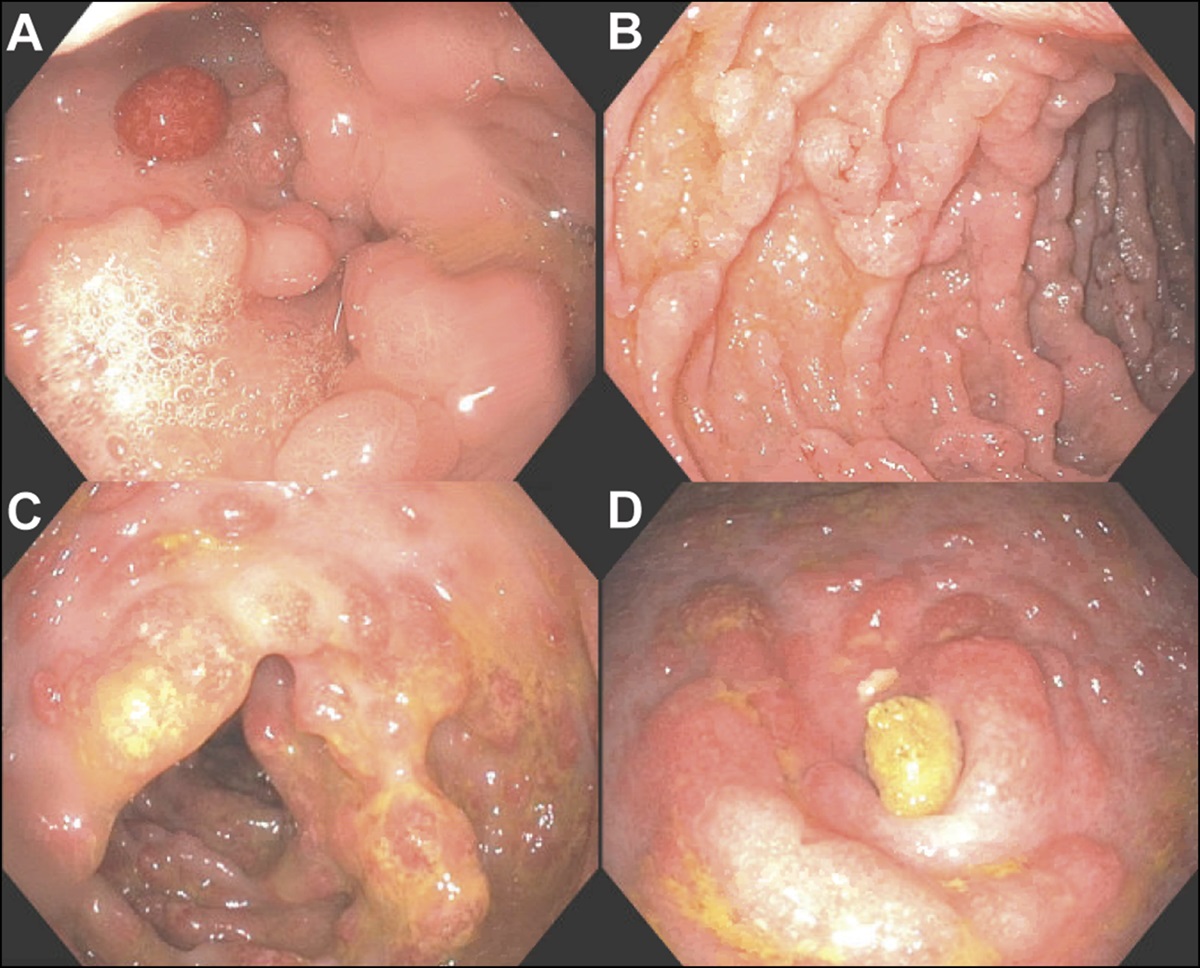
 Figure 1.:
Figure 1.: Index Dieulafoy bleeding just above the colorectal anastomosis.
 Figure 2.:
Figure 2.: Ulcer base (U) and clips (C) were from endotherapy of recent multiple bleeding sites. New active Dieulafoy bleeding site was marked with (*).
 Figure 3.:
Figure 3.: Color Doppler to highlight blood flow in vessels. *Superficial arterioles as the cause of recurrent Dieulafoy bleeding. The arrow shows the feeding arteriole in the submucosa. M, mucosa; MM, muscularis mucosa; SM, submucosa.
 Figure 4.:
Figure 4.: Magnified EUS view of the feeding arteriole (color Doppler with yellow bar—left panel) confirmed by an arterial pattern on Doppler (right panel). EUS, endoscopic ultrasound.
 Figure 5.:
Figure 5.: Left panel: (Arrow) 22G fine aspiration needle aiming at the feeding arteriole (*). Right panel: 2 coils were deployed in the feeding arteriole (faintly seen due to their small size, in the blue circle). Immediate cessation of blood flow was observed on Doppler in both feeding vessels and peripheral vessels.
 Figure 6.:
Figure 6.: Endoscopic resolution of active bleeding immediately after EUS-guided coil embolization. *Site of Dieulafoy bleeding treated with coil embolization and mild blanching in the area. (C) Clips used in previous endotherapy; (U) ulcer base from recent bipolar coagulation of a different site of Dieulafoy bleeding. EUS, endoscopic ultrasound.
DISCUSSIONRectal Dieulafoy bleeding is usually intermittent but can be profuse. Once identified on endoscopy, conventional endoscopic hemostatic maneuvers are effective to stop the bleeding as reported in the literature as well as in our case. However, our patient had surgical anastomosis and radiation therapy in the area, and he had multiple sites of Dieulafoy bleeding instead of just one. Every time he came in due to recurrent bleeding, we were effective in controlling the hemorrhage. To prevent recurrent bleeding, we had to embolize the submucosal arteriole that fed these smaller Dieulafoy vessels, which were found underneath and close to the mucosa at multiple sites. Angiographic embolization of a rectal vessel by interventional radiology could be considered, but there was a risk of causing further ischemia in the area because usually a larger arterial vessel that feeds the rectum would be targeted. We believe that EUS-guided coil embolization of the submucosal feeding arteriole may be as effective, yet a safer approach. Over-the scope clip has been used to treat a single Dieulafoy bleeding site in the upper gastrointestinal tract; however, in this case, because of recurrent hemorrhage from multiple sites, coil embolization of a feeding vessel deep in the submucosa may have a better outcome.
Vila et al previously reported a successful off-label use of 2% polidocanol to embolize rectal Dieulafoy bleeding under EUS guidance.6 Polidocanol was Food and Drugs Administration approved for the treatment of a varicose vein but had been used off label for esophageal varices sclerotherapy; N-butyl-2-cyanoacrylate was approved by the Foods and Drugs Administration for embolization of cerebral arteriovenous malformations and has been used off label for EUS-guided embolization of gastric varices. These 2 agents have not been applied in the treatment of arterial bleeding. Coil embolization, however, has been routinely used by interventional radiology (IR) for the treatment of arterial bleeding. Coil embolization has been used off label for EUS-guided embolization of gastric varices and recently rectal varices.5,7 EUS-guided coil embolization was also reported as a successful salvage therapy for visceral arterial aneurysm and pseudoaneurysm.7 Coil embolization of the submucosal arteriole does not have the potential risk of systemic embolization as in the case of venous or variceal coil deployment and may have less risk of ischemia followed by fibrosis and luminal stricture as with IR embolization of a feeding artery to a larger segment of the GI tract. We report the first case of successful EUS-guided coil embolization of a feeding arteriole to prevent recurrent rectal Dieulafoy bleeding. Further study may be needed to confirm the effectiveness of this approach in this rare condition. In addition, the success of this case suggests that EUS-guided coil embolization may also be effective in treating refractory arteriolar bleeding in the stomach and the duodenum, an alternative to angiographic embolization by IR and a new application for therapeutic EUS in addition to treating gastric varices.
DISCLOSURESAuthor contributions: Beside the main author, the other authors have involved in care of and have performed previous endoscopic procedures on the patient in this case report. They are also involved in the discussion and drafting of the report. HD Mai is the article guarantor.
Acknowledgments: The authors thank the dedicated work of our endoscopy and anesthesiology staff involved in this case: Heidi Francis, RN; Jennifer Pizarras-Rebosura, RN; and Maria Inton-Santos, MD.
Financial disclosure: This material is the result of work supported with resources and the use of facilities at the West Palm Beach VA Health Care System, Florida.
Disclaimer: The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Informed consent was obtained for this case report.
REFERENCES 1. Inayat F, Hussain A, Yahya S, et al. Rectal Dieulafoy's lesion: A comprehensive review of patient characteristics, presentation patterns, diagnosis, management, and clinical outcomes. Transl Gastroenterol Hepatol. 2022;7:10. 2. Dogan U, Gomceli I, Koc U, Habibi M, Bulbuller N. Rectal Dieulafoy lesions: A rare etiology of chronic lower gastrointestinal bleeding. Case Rep Med. 2014;2014:180230. 3. Pineda-De Paz MR, Rosario-Morel MM, Lopez-Fuentes JG, Waller-Gonzalez LA, Soto-Solis R. Endoscopic management of massive rectal bleeding from a Dieulafoy's lesion: Case report. World J Gastrointest Endosc. 2019;11(7):438–42. 4. Iwai N, Okuda T, Tsuji T, Kagawa K. Endoscopic band ligation for a rectal Dieulafoy's lesion. Ann Gastroenterol. 2020;33(2):220. 5. Rana SS, Sharma R, Gupta R. Refractory rectal variceal bleeding treated with EUS-guided coil embolization. Endoscopic Ultrasound. 2021;10(2):141–2. 6. Vila JJ, Pérez-Miranda M, Basterra M, Gómez M, Fernández-Urién I, Jiménez FJ. Endoscopic ultrasound-guided therapy of a rectal Dieulafoy lesion. Endoscopy. 2014;46(Suppl 1 UCTN):E84–5. 7. Ryou M, DeWitt JM, Das KK, Shami VM. AGA clinical practice update on interventional EUS for vascular investigation and therapy: Commentary. Clin Gastroenterol Hepatol. 2023;21(7):1699–705.e2.
留言 (0)