
記住我





Celiac disease (CD) is an immune-mediated enteropathy that primarily affects the duodenum and jejunum. It is associated with class II haplotypes of human leukocyte antigen DQ2 (haplotypes DR-17 or DR5/7) and DQ8 (haplotype DR-4). CD is associated with several neurological conditions including neuromyelitis optica, epilepsy, and cerebellar ataxia.1–3 The association between CD and transverse myelitis (TM), however, is not well established in the literature. We present a rare case of CD diagnosed during presentation of TM.
CASE REPORTA 25-year-old man presented to the emergency department with acute onset bilateral lower extremity (BLE) weakness after 1 week of intermittent pain and numbness in both legs. Systemic review was otherwise negative. Patient's medical history was unremarkable except for pericarditis 1 year prior, which occurred after he received his second dose of the mRNA COVID vaccine. He had no history of recent illness or vaccinations. The only medications he was taking at the time were citalopram, melatonin, and testosterone for gender-affirming care.
Neurologic examination revealed 0/5 strength in BLE, complete loss of sensation below T4, and urinary retention. A whole spine magnetic resonance image revealed heterogeneous, cross-sectional abnormal cord signal from C4 to the upper thoracic spine, consistent with TM. Plasma exchange was initiated, and symptom progression halted.
Cerebrospinal fluid work-up was remarkable for mildly elevated protein (62 mg/dL) and significant red blood cells (390 mm3) without evidence of oligoclonal bodies or aquaporin-4 antibodies. Cerebrospinal fluid viral studies, cultures, and Mayo autoimmune myelopathy panel were also negative.
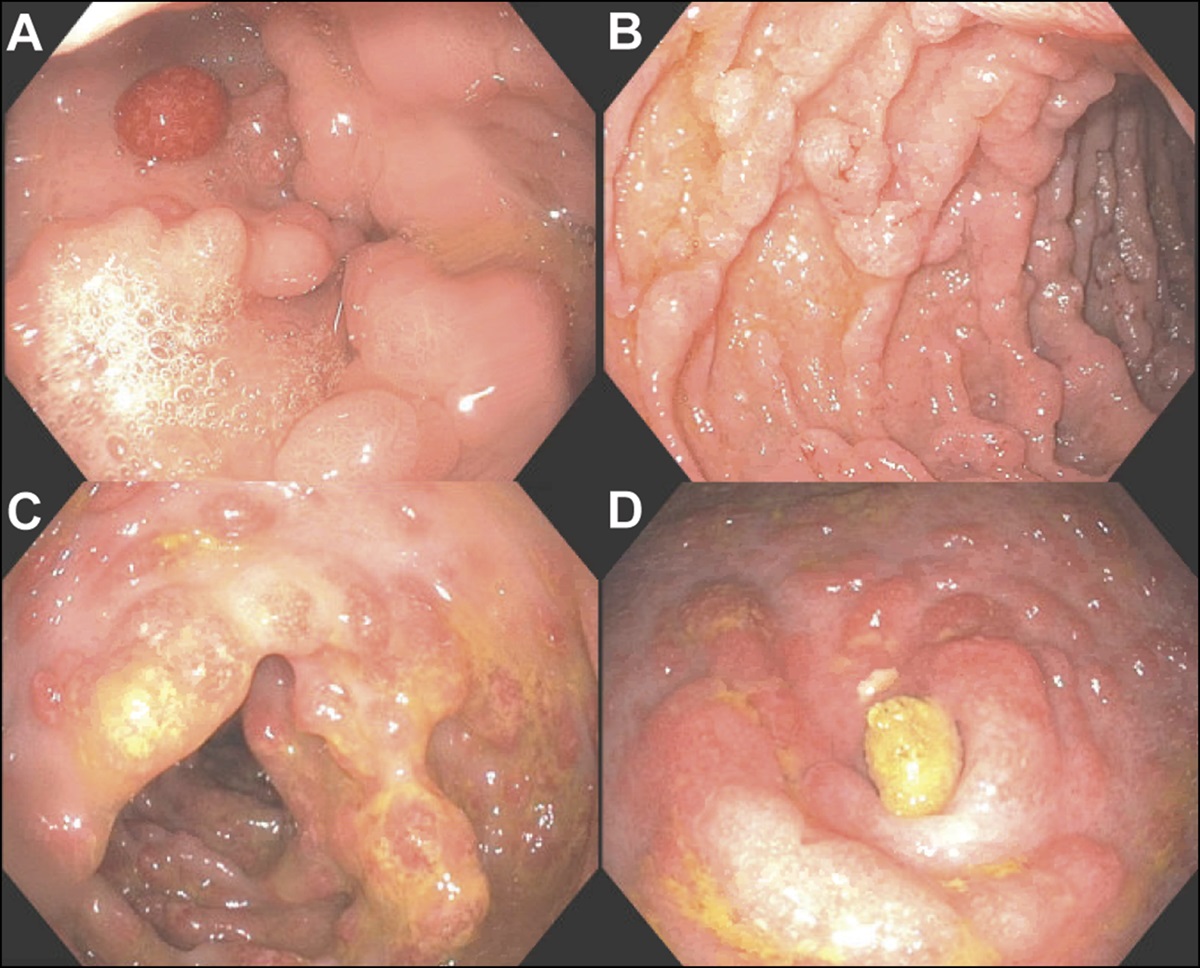
Serologic work-up included infectious, immunologic, nutritional, endocrine, and autoimmune studies. Testing was unremarkable except for positive anti-tissue transglutaminase antibody (TTG IgA) and anti-gliadin IgA with low copper (43 mcg/dL) and vitamin E (4.6 μg/mL) levels. Endomysial antibody was not obtained. A 2008 study comparing serologic markers of CD found that TTG IgA was 78% sensitive and 98% specific for detecting CD and anti-gliadin IgA was 63% sensitive and 90% specific for CD before treatment initiation; however, histopathology was still found to be the gold standard.4 Our patient thus underwent esophagogastroduodenoscopy (EGD) for definitive diagnosis. EGD revealed scalloping, loss of folds, and mucosal atrophy in the duodenal bulb and second portion of the duodenum (Figure 1). Duodenal biopsy revealed mild villous blunting, crypt hyperplasia, and patchy increase of intraepithelial lymphocytes, consistent with active CD (Figure 2). Family history was significant for CD in a maternal aunt and lymphocytic colitis in his mother.
 Figure 1.:
Figure 1.: Endoscopic image showing scalloping and mucosal atrophy in the second portion of duodenum.
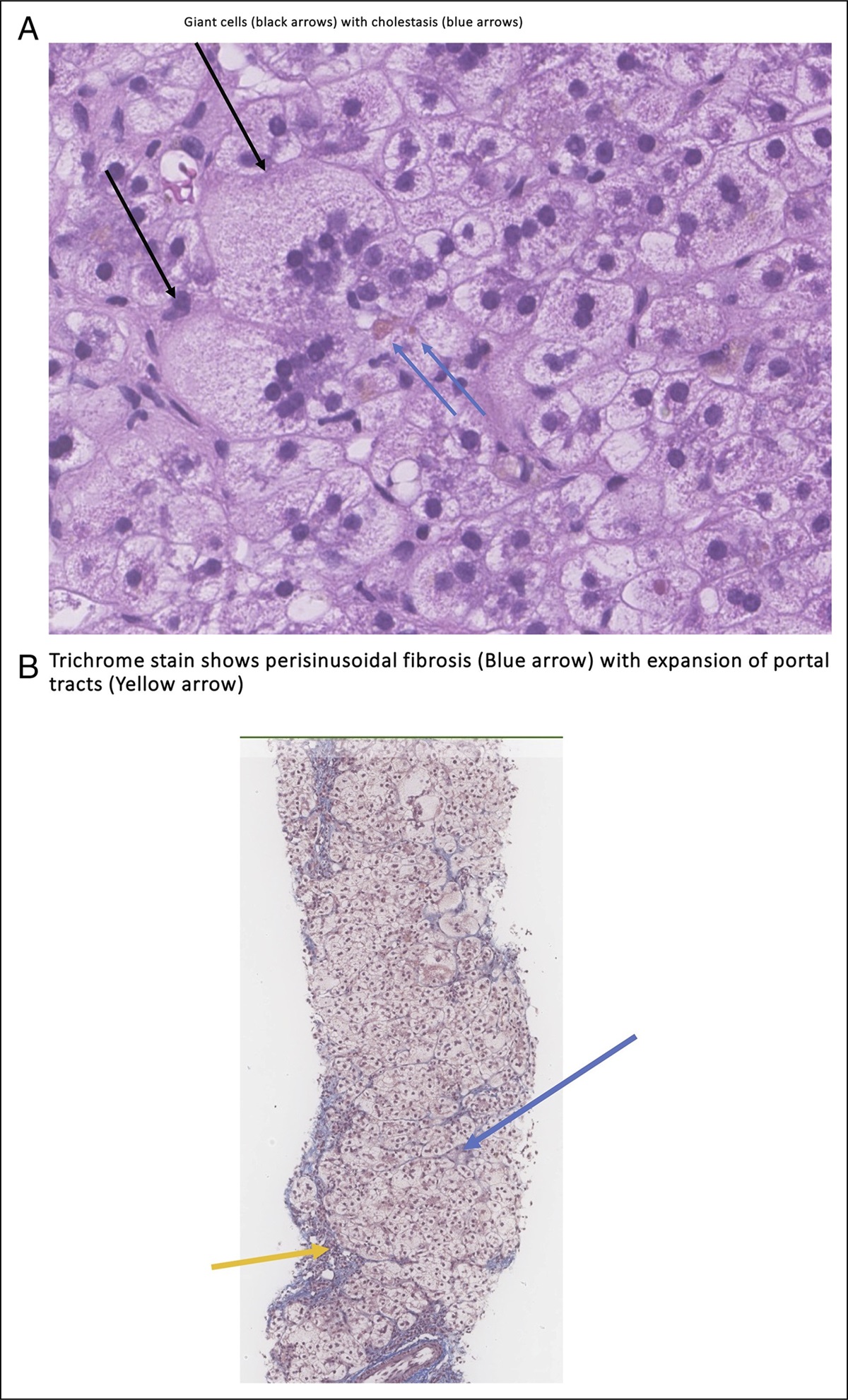
 Figure 2.:
Figure 2.: H&E stain (20×) of the second portion of the duodenum, demonstrating mucosa with patchy increase of intraepithelial lymphocytes, mild villous blunting, crypt hyperplasia, and increase of lymphoplasmacytic cells in the lamina propria. In this patient with elevated TTG antibody, the histologic findings are supportive of celiac disease. TTG, tissue transglutaminase.
The patient was diagnosed with TM, presumed secondary to untreated CD. He was initiated on a gluten-free diet and rituximab for TM before discharge to a rehabilitation facility where he continues to have slow recovery of BLE strength and sensation. Repeat EGD 3 months later showed some healing of the duodena mucosa but persistent mild changes of CD on histology (Figure 3). TTG IgA antibodies decreased to 42, from >128 on initial presentation.
 Figure 3.:
Figure 3.: Endoscopic image showing decreased scalloping and improvement in mucosal atrophy in the second portion of duodenum.
DISCUSSIONTo our knowledge, this is one of few case reports of TM as a presenting symptom of CD in an adult.1,5
CD is an autoimmune disease characterized by gluten hypersensitivity. The association of CD with other neurological diseases such as neuromyelitis optica, epilepsy, cerebellar ataxia, and peripheral neuropathy is well described.1–3 These neurological disorders have been reported as both presenting symptoms and complications of CD.2 The strong association of these diseases with CD has led some authors to consider them a red flag for undiagnosed CD.2 Studies have shown that up to 7% of adult patients with CD present with neurological changes.3
TM is an inflammatory disorder characterized by bilateral sensory, motor, or autonomic dysfunction associated with the spinal cord. It can be idiopathic or associated with other diseases, especially autoimmune disorders such as systemic lupus erythematous, sarcoidosis, and Sjogren syndrome.6 In our case, no cause of TM was established despite extensive investigations. This case adds to a sparse evidence base supporting an association between CD and TM.
There are case reports of TM in patients with underlying gastrointestinal (GI) diseases, including ulcerative colitis.7 Some gastrointestinal infections such as Campylobacter jejuni, Salmonella, Hepatitis, and Helicobacter pylori are also associated with TM. There is additionally 1 case report of TM as a presenting symptom of CD in the pediatric age group.6 The pathogenesis linking CD with neurological manifestations is unknown; however, several theories are proposed, including invasion of CD8-positive T cells into the nervous system, autoantibodies directed against neuronal cells, and celiac-associated vitamin deficiencies such as folic acid, vitamin E, copper, and biopterin.2 Copper deficiency, likely secondary to CD, was present in our patient; however, neurologic manifestations from copper deficiency tend to mirror B12 deficiency and primarily affect the dorsal columns of the spine, which is inconsistent with our patient's presentation.8 We therefore believe CD itself, not a secondary vitamin deficiency, was primarily contributing to the patient's TM.
A notable aspect of this case is that the patient did not have prior signs or symptoms of CD. In subsequent clinic visits, the patient noted that he had always avoided “highly bready foods, like pizza,” because they make him feel sick, but he did not have typical symptoms of bloating or diarrhea.
There is conflicting evidence regarding the efficacy of gluten-free diet in controlling the symptoms of neurological diseases associated with CD.3 One study showed improvement of neurological symptoms such as gluten ataxia; celiac, epilepsy, and cerebral calcification syndrome; headache; and peripheral neuropathy with gluten-free diet.2 Similarly, studies indicate that gluten-free diet allows for better control of seizures in celiac-associated epilepsy.3
The role of celiac serologies in predicting recovery from neurologic disease is also unclear. One mid-sized study in Brazil found no relationship between serologic presence of celiac antibodies and multiple sclerosis, neuromyelitis optima, and inflammatory myelitis in patients with established CD.9
Our patient started gluten-free diet during his hospitalization for TM. At 6-week follow-up, his lower extremity strength improved to 2/5 from 0/5. This level of improvement is consistent with the natural course of TM, so it is difficult to determine the impact of gluten-free diet on his recovery.
DISCLOSURESAuthor contributions: ME Moore wrote the case presentation, revised the final manuscript, and treated the patient. F. Talat worked on the case discussion and abstract. M. Talanian helped revise the manuscript and treated the patient. The entire article was proofread by H. Allison who made the required corrections in the complete manuscript. ME Moore is the article guarantor.
Financial disclosure: None to report.
Informed consent could not be obtained for this case report. All identifying information has been removed.
REFERENCES 1. Iyer A, Rathnasabapathi D, Elsone L, et al. Transverse myelitis associated with an itchy rash and hyperckemia: Neuromyelitis optica associated with dermatitis herpetiformis. JAMA Neurol. 2014;71(5):630–3. 2. Trovato CM, Raucci U, Valitutti F, et al. Neuropsychiatric manifestations in celiac disease. Epilepsy Behav. 2019;99:106393. 3. Shapiro M, Blanco DA. Neurological complications of gastrointestinal disease. Semin Pediatr Neurol. 2017;24(1):43–53. 4. Rashtak S, Ettore MW, Homburger HA, Murray JA. Comparative usefulness of deamidated gliadin antibodies in the diagnosis of celiac disease. Clin Gastroenterol Hepatol. 2008;6(4):426–370. 5. Jacob S, Zarei M, Kenton A, Allroggen H. Gluten sensitivity and neuromyelitis optica: Two case reports. J Neurol Neurosurg Psychiatry. 2005;76(7):1028–30. 6. Krom H, Sprangers F, van den Berg R, Benninga MA, Kindermann A. Transverse myelitis as manifestation of celiac disease in a toddler. Pediatrics. 2017;139(3):e20161381. 7. Yang Y, Zhang Y. Acute transverse myelitis in an adult-patient with underlying ulcerative colitis: A case report. BMC Gastroenterol. 2022;22(1):161. 8. Kumar N. Copper deficiency myeloneuropathy. UpToDate (www.uptodate.com/contents/copper-deficiency-myeloneuropathy). Accessed July 27, 2023. 9. de Oliveira P, de Carvalho DR, Brandi IV, Pratesi R. Serological prevalence of celiac disease in Brazilian population of multiple sclerosis, neuromyelitis optica and myelitis. Mult Scler Relat Disord. 2016;9:125–8.
留言 (0)