
記住我





Bilothorax is an extremely uncommon etiology of exudative pleural effusions that involves direct leakage of bile into the pleural cavity after damage from a traumatic, infectious, or iatrogenic mechanism.1 Rarely, bilothorax can arise as a major complication of percutaneous transhepatic biliary drainage (PTBD), which is a well-established procedure that has been used in the setting of biliary obstruction when endoscopic retrograde cholangiopancreatography (ERCP) is unsuccessful or unfeasible. Only a small number of cases of bilothorax have been reported in the literature, with even fewer being documented as a result of PTBD. We report a case of bilothorax in a patient with primary sclerosing cholangitis following PTBD and document its diagnosis, management, and potential implications.
CASE REPORTA 66-year-old man with history of end-stage liver disease secondary to primary sclerosing cholangitis presented to the emergency department with a 3-week history of fevers, confusion, and dyspnea. On physical examination, the patient was jaundiced with a distended abdomen, minimal ascites, and periumbilical tenderness. Liver magnetic resonance imaging showed diffuse strictures of the proximal common bile duct and common hepatic duct with right and left intrahepatic biliary dilation. Laboratory test results and vitals were concerning for septic shock in the setting of acute cholangitis. The patient was subsequentially transferred to the intensive care unit and started on broad-spectrum antibiotics and pressors. Hepatology and interventional radiology services were consulted as the patient had a history of 2 failed ERCPs due to complex strictures. A rendezvous ERCP procedure was initially recommended; however, given the high risk of further decompensation, it was ultimately decided that the patient undergo an urgent PTBD for biliary decompression and source control. A right external biliary drain was placed, with cultures positive for multidrug-resistant Pseudomonas aeruginosa.
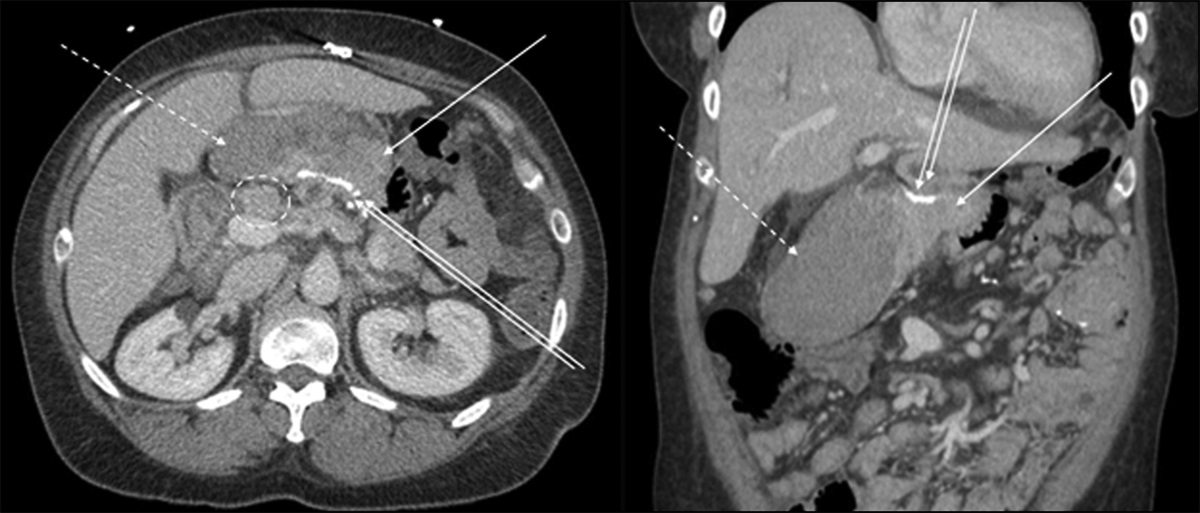
Three days after PTBD, the patient developed dyspnea and right-sided pleuritic chest pain. Chest computed tomography revealed a new right pleural effusion with total collapse of the right lower lobe (Figure 1). Interventional radiology (IR) performed both a diagnostic thoracentesis and subsequent drain exchange/upsize of the PTBD. However, during the procedure, pullback cholangiogram showed contrast extravasating into the right pleural space, indicative of diaphragmatic injury (Figure 2). Pleural studies were consistent with an exudative effusion with the pleural bilirubin level noted to be elevated to 9.8 mg/dL. Thoracic surgery was consulted and placed a 12 French pigtail chest tube. This yielded 1.3 L of dark bilious fluid and confirmed the bilothorax diagnosis. The patient was made status 7 (inactive) on the liver transplant list given subsequent development of empyema and Pseudomonas liver abscess and was recommended to continue piperacillin-tazobactam for 3 weeks. Owing to further clinical deterioration, the patient underwent surgical decortication of the right hemithorax with diaphragmatic repair. Large loculated fluid and bile-tinged debris were noted diffusely in the pleural space during the operation. His postoperative course was complicated by hemorrhagic shock, and despite aggressive measures, the patient suffered cardiopulmonary arrest days later and died.
 Figure 1.:
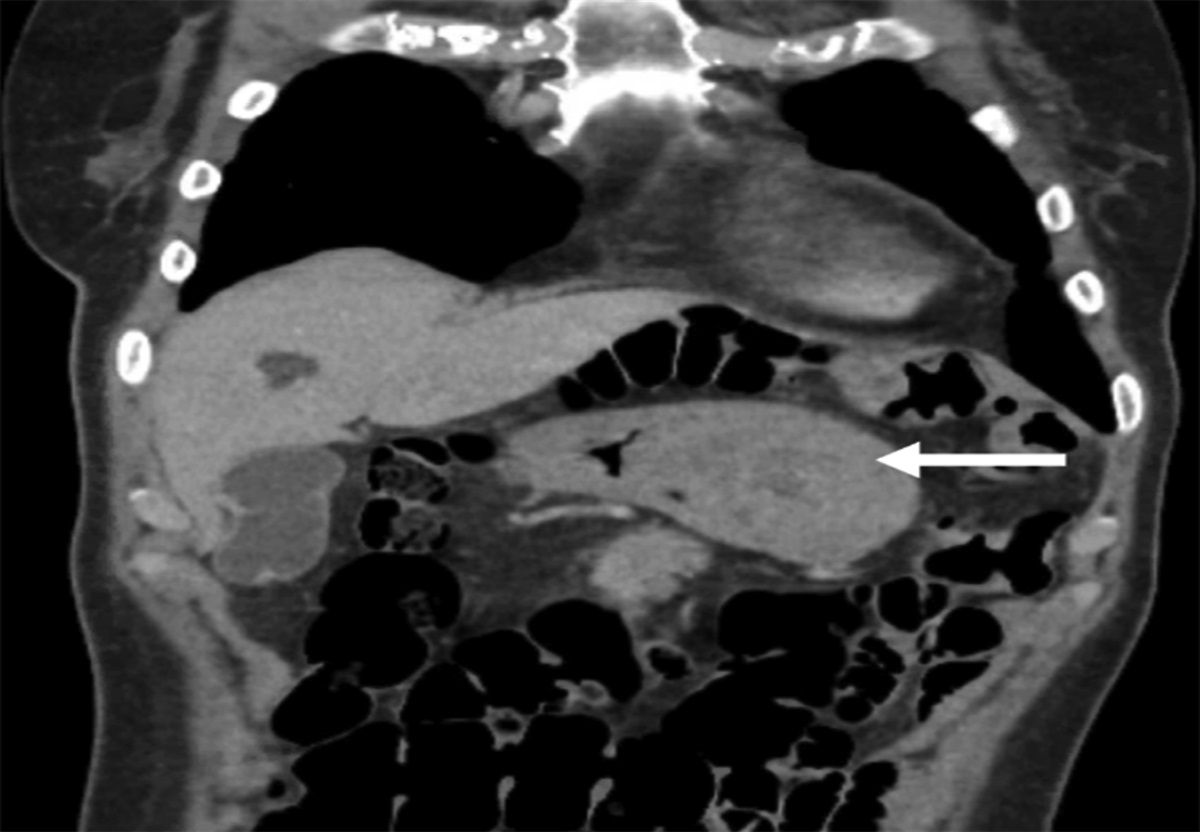
Figure 1.: Chest computed tomography demonstrating patient's lungs on initial presentation to the emergency department (A) vs 3 days subsequent to the initial percutaneous transhepatic biliary drainage procedure (B).
 Figure 2.:
Figure 2.: Cholangiography with good opacification of the biliary tree without leakage at initiation of percutaneous transhepatic biliary drainage (A) vs contrast extravasation into the right pleural space at the end of the procedure (B).
DISCUSSIONEndoscopic interventions for biliary obstructions fail in approximately 5%–10% of cases due to altered biliary anatomy or difficult biliary cannulation, requiring the utilization of PTBD as an alternative for biliary decompression.2 The complication rate of PTBD ranges between 3% and 10%, with reported complications such as infection, bile leakage, and hemorrhage being well reported in the literature.3 However, bilothorax is a rare complication of this procedure that has scarcely been described, except in isolated case reports. In our literature review of bilious pleural effusions, approximately 23 cases were published in the literature from 1971 to 2023, with only 4 cases reported as a result of PTBD. Other documented etiologies of bilothorax in these cases include thoracoabdominal/diaphragmatic trauma, biliopleural fistula, infection, inflammation, and gastrointestinal malignancy.4,5 The mechanism of bilothorax formation in our patient was likely secondary to diaphragmatic injury from the PTBD catheter during the procedure. The PTBD catheter crosses from the high-pressure obstructed biliary system into the low-pressure pleural space. This pressure differential, augmented by the pump action of the negative pleural pressure of the respiratory cycle, subsequently leads to retrograde flow of bile into the right thorax.1,5
The clinical presentation of bilothorax usually involves ipsilateral pleuritic chest pain and respiratory distress in a patient with recent gastrointestinal manipulation or a hepatobiliary procedure.6 Diagnosis of bilothorax involves a high degree of clinical suspicion and chest imaging to confirm the presence of a pleural effusion. Most cases in the literature usually present as a right-sided pleural effusion given the anatomical location of the liver and biliary tree; however, 2 cases of left-sided bilothorax and 1 case of bilateral bilothorax have also been reported.1,7-9 Observation of a pleural effusion should be followed by diagnostic thoracentesis with measurement of pleural total bilirubin. Visually, the pleural fluid will appear green-black, with an exudative profile on fluid studies. In various case reports, pleural-to-serum total bilirubin (P/S) ratio >1.0 has been reported as an indicator of the presence of bilothorax.
A case review of 12 patients reported the sensitivity of bilothorax detection when the P/S ratio is >1 to be 76.9%.4 However, similar to this case presentation, 2 patients in the case review did not satisfy this criterion despite having a diagnosis of bilothorax. There is no established guideline for the management of bilothorax, and treatment recommendations are largely anecdotal using case reports. However, management typically involves prompt initiation of antibiotics and immediate drainage of the bilious effusion by tube thoracostomy or, less commonly, surgical intervention for complex effusions.
Prompt recognition of bilothorax is important as bile is a potent chemoirritant that can lead to a severe inflammatory response, such as acute respiratory distress syndrome.10 In addition, given that bile is a medium conducive for bacterial growth, bilothorax places patients at higher risk for the development of bacterial empyema, especially those with chronic liver disease and cirrhosis given their immunocompromised state.4 Infections such as empyema can increase mortality 4-fold in patients with cirrhosis.11,12
In summary, bilothorax is a rare complication of hepatobiliary procedures that can result in rapid clinical deterioration. Prompt recognition and management of this condition is imperative, especially in patients with chronic liver disease and cirrhosis.
DISCLOSURESAuthor contributions: T. Olasehinde drafted the article, reviewed the present literature, and edited the article. N. Stehouwer edited and revised the article. T. Olasehinde is the article guarantor. All authors approved the final version of the manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Vrachliotis TG, Spiliopoulos S, Voros D. Management of massive bilothorax post-percutaneous trans-hepatic biliary drainage. Egypt J Radiol Nucl Med. 2022;53(1):59. 2. Bapaye A, Dubale N, Aher A. Comparison of endosonography-guided vs. percutaneous biliary stenting when papilla is inaccessible for ERCP. United Eur Gastroenterol J. 2013;1(4):285–93. 3. Lee YT, Yen KC, Liang PC, Wu CH. Procedure-related risk factors for bleeding after percutaneous transhepatic biliary drainage: A systematic review and meta-analysis. J Formos Med Assoc. 2022;121(9):1680–8. 4. Saraya T, Light RW, Sakuma S, et al. A new diagnostic approach for bilious pleural effusion. Respir Investig. 2016;54(5):364–8. 5. Petri CR, Majid A, Anandaiah A. A man with biliary sepsis and an enlarging pleural effusion. Ann Am Thorac Soc. 2019;16(4):496–8. 6. Karnik NP, Shair KA. Iatrogenic bilothorax: A rare complication of orthotopic liver transplant. ACG Case Rep J. 2019;6(7):e00137. 7. Soler-Sempere M, Vicente-Ibarra N, Heredia-Oliva L. An unusual case of left-sided massive biliothorax. Int J Respir Pulm Med. 2015;2(4). 8. Reddy VD, Al-Khateeb A, Hussain M, et al. Case report: Kryptonite-A rare case of left-sided bilothorax in a sickle cell patient. Case Rep Pulmonol. 2019;2019:8658343. 9. Shah K, Ravikumar N, Uddin QK, McGee W, Farmer MJS. Bilateral bilothorax: An unusual cause of bilateral exudative pleural effusion. Cureus. 2019;11(7):e5185. 10. Basu S, Bhadani S, Shukla VK. A dangerous pleural effusion. Ann R Coll Surg Engl. 2010;92(5):W53–W54. 11. Shen TC, Chen CH, Lai HC, et al. Risk of empyema in patients with chronic liver disease and cirrhosis: A nationwide, population-based cohort study. Liver Int. 2017;37(6):862–70. 12. Arvaniti V, D'Amico G, Fede G, et al. Infections in patients with cirrhosis increase mortality four-fold and should be used in determining prognosis. Gastroenterology. 2010;139(4):1246–56.e12565.
留言 (0)