
記住我



The dynamic stages of chronic hepatitis B infection are affected by interaction between the hepatitis B virus (HBV) and host immune system.1 Host immune response, comprising of B and T cells, is responsible for controlling active viral replication. However, achieving true sterile cure from HBV infection is usually impossible, despite appropriate seroconversion of HBV E-antigen (HBeAg) or HBV surface antigen (HBsAg). With current therapeutic approaches, functional cure is the goal, which means undetectable hepatitis B viral load in serum and absence of liver injury based on biochemical or histological assessment. Even when HBV is undetected in serum, covalently closed circular DNA belonging to HBV still survives inside nuclei of hepatocytes. In addition, HBV can replicate inside hepatocytes at a level undetectable by serological testing.2,3 Clinical settings that can suppress the host immune system are associated with risk of hepatitis B reactivation (HBVr) manifesting as rebound of HBV DNA in serum and HBsAg seroreversion.4
HBVr was first associated with anticancer therapy.5 There has been an increase in documented cases of HBVr with newer immunosuppressive regimens. In patients receiving immunosuppressive therapies associated with rheumatoid conditions, HBVr in HBsAg-positive and hepatitis B core antibody (HBcAb)-positive patients has been reported to be 12.3%, whereas it is 1.7% in HBsAg-negative and HBcAb-positive patients.6
Three Janus kinase (JAK) inhibitors, including tofacitinib, baricitinib, and upadacitinib, have been approved for treatment of rheumatoid arthritis (RA).7 Our case discusses a patient who received upadacitinib as therapy for RA and developed HBVr in the absence of antiviral prophylaxis.
CASE REPORTWe present a case of a 55-year-old Asian woman with medical history significant for RA and immune-controlled HBeAg-negative chronic HBV infection. She was diagnosed with HBV infection at age 27 years and never required treatment, given persistently normal alanine aminotransferase (ALT) levels and biochemical fibrosis scores. Her previous medications for RA were hydroxychloroquine, methotrexate, and tofacitinib. Five months before the current presentation, she was started on upadacitinib. She presented to an outside hospital with 1-week history of right upper-quadrant pain, nausea, and vomiting. Her total bilirubin (TB) level was 4.7 mg/dL, (ALT 1,015 U/L, international normalized ratio (INR) 1.60, and HBV DNA > 1,000,000,000 IU/mL. Hence, she was diagnosed with HBVr, and tenofovir alafenamide was initiated on discharge. A day after discharge, she had further worsening of hepatic parameters (ALT 1,501 U/L and total bilirubin (TB) 6.8 mg/dL) after which she was referred to our liver transplant center.
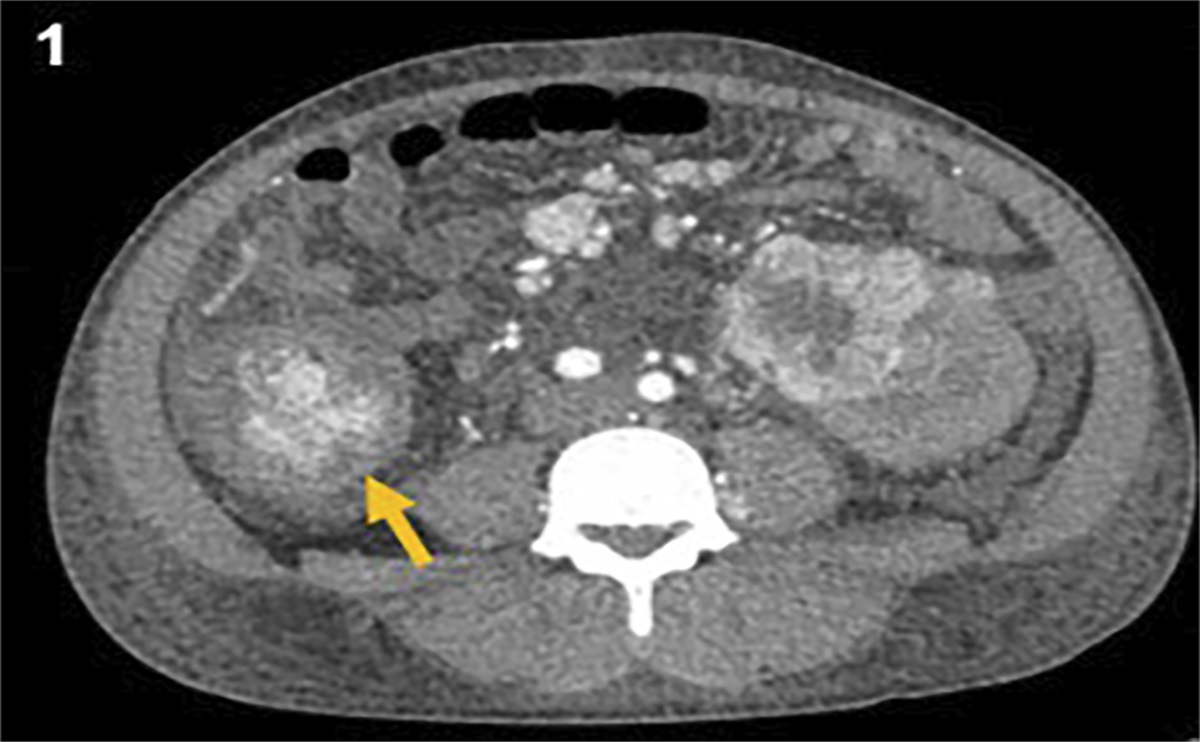
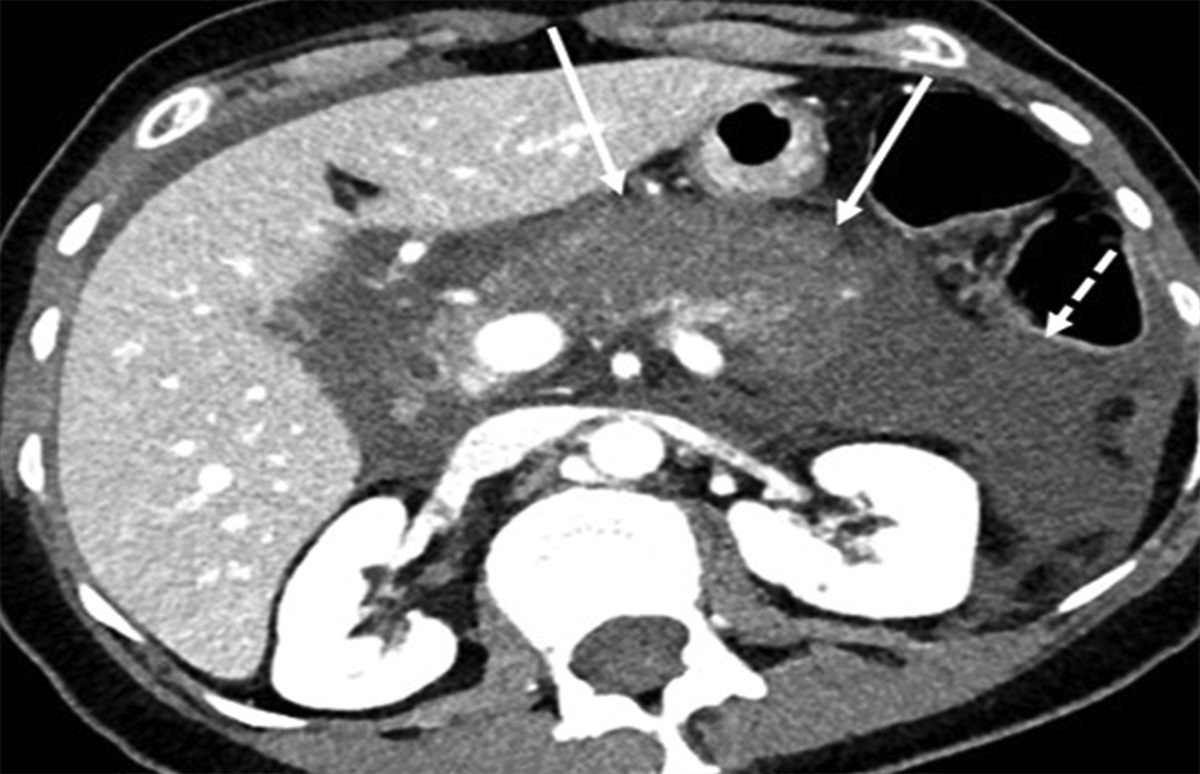
On presentation to our emergency department, she had an unremarkable physical examination other than jaundice. Bloodwork was significant for INR 2.0, ALT 1,636 U/L, and TB 7.2 mg/dL. Serological bloodwork showed reactive HBsAg, total HBcAb, and HBeAb, whereas HbcAb IgM, HBeAg, and HBsAb were negative. Other relevant causes of acute hepatitis were ruled out. Abdomen magnetic resonance imaging was significant for slightly nodular contour of the liver, suggestive of cirrhosis but without signs of portal hypertension. She was again diagnosed with acute severe hepatitis B flare-up in the setting of immunosuppression from upadacitinib but with underlying possible cirrhosis. Her Model for End-Stage Liver Disease score rapidly progressed to 37 with INR reaching 6.0 in 1 day. Emergent liver transplant evaluation was initiated because of concern for fulminant hepatic failure, and she was listed for a liver transplant within 48 hours of presentation.
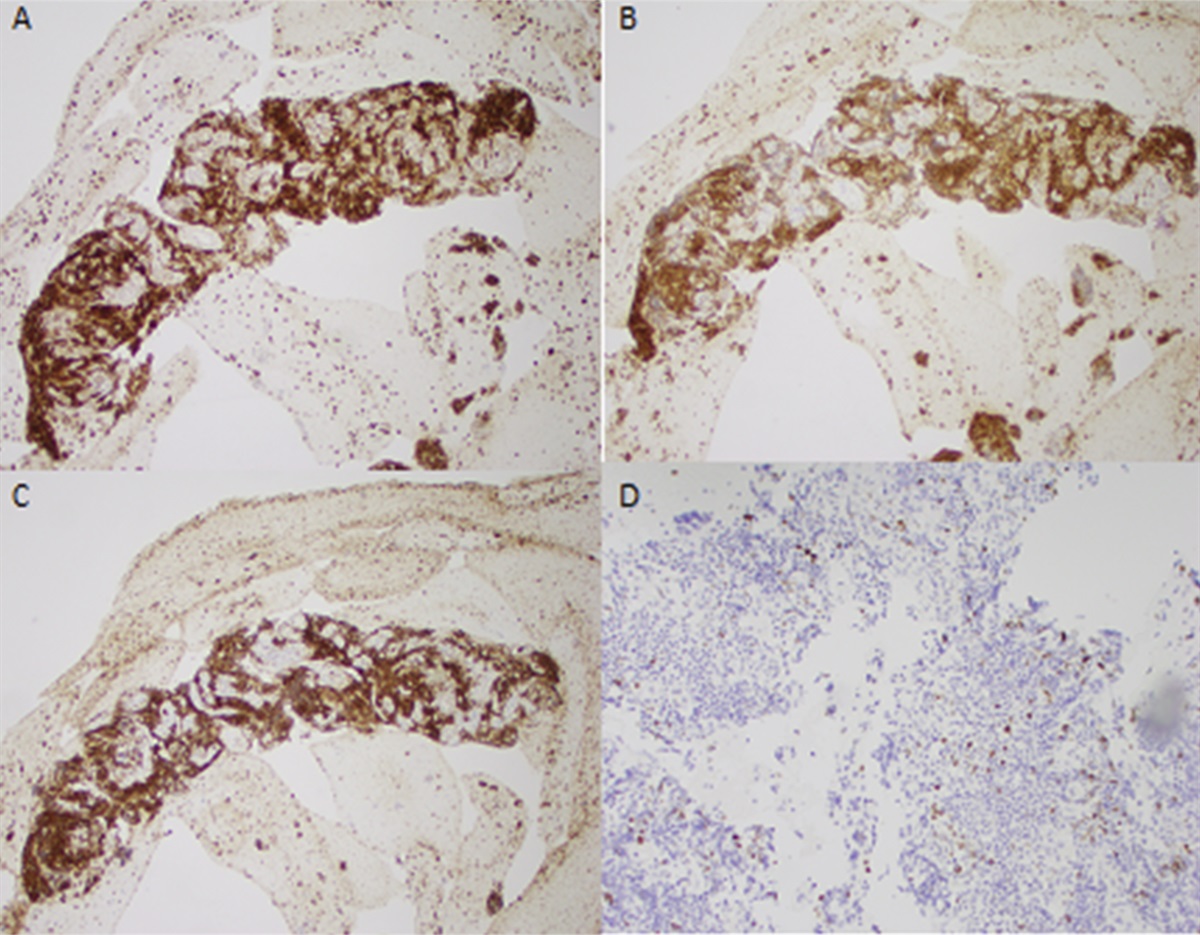
Figure 1 depicts patient's aminotransferases and bilirubin levels during this period. On day 5 of presentation, she underwent orthotopic liver transplantation. Her explant pathology confirmed HBVr-related fulminant hepatitis with 80%–90% parenchymal collapse with no evidence of cirrhosis (Figure 2). Her post-transplant course was unremarkable, and she was treated with tenofovir alafenamide. Tenofovir alafenamide was chosen over tenofovir disoproxil fumarate because of a better bone and renal safety profile. She also received HBV immunoglobulin for 6 months to maintain adequate HBsAb titer per center protocol.
 Figure 1.:
Figure 1.: Patient's aminotransferases and bilirubin levels.
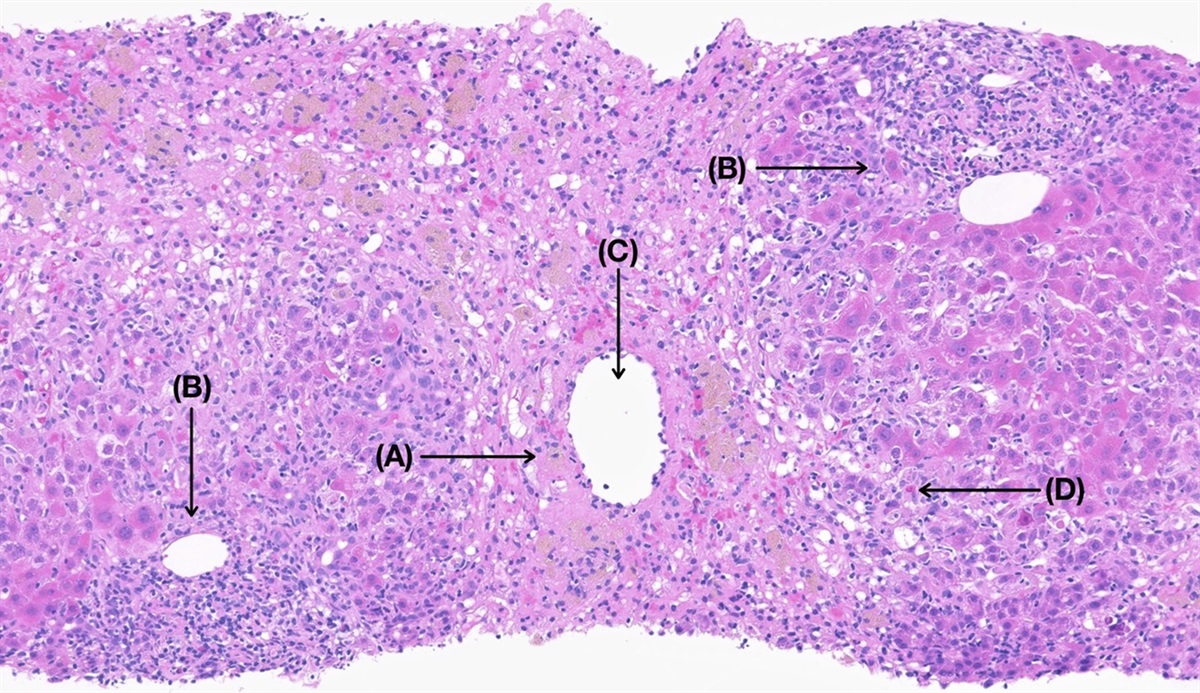
 Figure 2.:
Figure 2.: Histopathology of explanted liver tissue. (A) 200× Low-power view of fulminant active hepatitis with altered liver architecture with prominent hepatocyte collapse (80%–90% of parenchyma) admixed with abundant lymphoplasmacytic inflammation. (B) 400× High-power view of hepatocytes with reactive change and lymphoplasmacytic inflammatory infiltrate. (C) 400× Hepatitis B surface highlights cytoplasmic staining of affected hepatocytes. (D) 400× Hepatitis B core highlights nuclear expression of affected hepatocytes.
DISCUSSIONHBVr initiates with viral replication after exposure to immunosuppressive therapy. As per American Association for the Study of Liver Disease 2018 Hepatitis B guidance report, the criteria for HBVr include rise in HBV DNA from baseline and HBsAg seroreversion, that is, from HBsAg-negative to HBsAg-positive status.6 Anti-HBV therapy or cessation of immunosuppressive therapy can lead to improvement. However, some patients may develop injury and subsequent liver failure. The mortality rate associated with liver failure is high, and patients can end up requiring evaluation for liver transplantation.
Upadacitinib is a selective JAK 1 inhibitor, affecting the interleukin 6 and interferon (IFN) γ-related signaling, and is used in the treatment of several autoimmune disorders. IFN-α/β and IFN-γ are involved in antiviral responses, which are mediated by JAK1-tyrosine kinase 2 and JAK1-JAK-2 complexes, respectively.8,9 JAK inhibitors can thus impair the effect of IFN on viral replication. They also blunt T cell–based cell-mediated immunity by suppressing production of proinflammatory cytokines.10 Furthermore, JAK inhibitors negatively impact function and migration of dendritic cells contributing to HBVr.9,10
A meta-analysis involving patients with RA receiving disease-modifying antirheumatic drugs who were HBsAg-negative and HBcAb-positive was found to have a 1.0% pooled reactivation rate with JAK inhibitors.11 A retrospective cohort study of patients receiving tofacitinib was able to show that 2 of the 6 HBsAg-positive patients developed HBVr.12 HBVr with ruxolitinib use has also been documented.13–15 US Food and Drug Administration Adverse Event Reporting System shows a total of 41 cases of HBVr from JAK inhibitors, with 2 patients receiving upadacitinib.16 No case report of upadacitinib-induced HBVr has been published to date, however, to the best of our knowledge.
Biologic agents are being widely used in various autoimmune conditions and malignancies.17 Careful assessment of the risk of HBVr is crucial in patients receiving these agents with underlying chronic HBV infection. In patients at high risk of HBVr, institution of timely antiviral prophylaxis can significantly reduce the risk of HBVr and prevent associated morbidity or mortality. Patients not on prophylaxis for HBV infection may need to be monitored for HBVr based on their risk profile.
DISCLOSURESAuthor contributions: SA Khan: literature review, data collection, manuscript drafting, review, and editing. R. Zahid: literature review, manuscript drafting. M. Amir: data collection, manuscript drafting, review, and editing. SA Khan is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Manzano-Alonso ML, Castellano-Tortajada G. Reactivation of hepatitis B virus infection after cytotoxic chemotherapy or immunosuppressive therapy. World J Gastroenterol. 2011;17(12):1531–7. 2. Wang Y, Han SHB. Hepatitis B reactivation: A review of clinical guidelines. J Clin Gastroenterol. 2021;55(5):393–9. 3. Lok AS, Zoulim F, Dusheiko G, Ghany MG. Hepatitis B cure: From discovery to regulatory approval. Hepatology. 2017;66(4):1296–313. 4. Seetharam A, Perrillo R, Gish R. Immunosuppression in patients with chronic hepatitis B. Curr Hepatol Rep. 2014;13(3):235–44. 5. Papatheodoridis GV, Lekakis V, Voulgaris T, et al. Hepatitis B virus reactivation associated with new classes of immunosuppressants and immunomodulators: A systematic review, meta-analysis, and expert opinion. J Hepatol. 2022;77(6):1670–89. 6. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Clin Liver Dis (Hoboken). 2018;12(1):33–4. 7. Koutsianas C, Thomas K, Vassilopoulos D. Reactivation of hepatitis B virus infection in rheumatic diseases: Risk and management considerations. Ther Adv Musculoskelet Dis. 2020;12:1759720X20912646. 8. Loomba R, Liang TJ. Hepatitis B reactivation associated with immune suppressive and biological modifier therapies: Current concepts, management strategies, and future directions. Gastroenterology. 2017;152(6):1297–309. 9. Akiyama S, Cotter TG, Sakuraba A. Risk of hepatitis B virus reactivation in patients with autoimmune diseases undergoing non-tumor necrosis factor-targeted biologics. World J Gastroenterol. 2021;27(19):2312–24. 10. Reinwald M, Silva JT, Mueller NJ, et al. ESCMID study group for infections in compromised hosts (ESGICH) consensus document on the safety of targeted and biological therapies: An infectious diseases perspective (intracellular signaling pathways: Tyrosine kinase and mTOR inhibitors). Clin Microbiol Infect. 2018;24(Suppl 2):S53–70. 11. Hong X, Xiao Y, Xu L, Liu L, Mo H, Mo H. Risk of hepatitis B reactivation in HBsAg-/HBcAb+ patients after biologic or JAK inhibitor therapy for rheumatoid arthritis: A meta-analysis. Immun Inflamm Dis. 2023;11(2):e780. 12. Chen YM, Huang WN, Wu YD, et al. Reactivation of hepatitis B virus infection in patients with rheumatoid arthritis receiving tofacitinib: A real-world study. Ann Rheum Dis. 2018;77(5):780–2. 13. Kirito K, Sakamoto M, Enomoto N. Elevation of the hepatitis B virus DNA during the treatment of polycythemia vera with the JAK kinase inhibitor ruxolitinib. Intern Med. 2016;55(10):1341–4. 14. Lussana F, Cattaneo M, Rambaldi A, Squizzato A. Ruxolitinib-associated infections: A systematic review and meta-analysis. Am J Hematol. 2018;93(3):339–47. 15. Ogawa E, Wei MT, Nguyen MH. Hepatitis B virus reactivation potentiated by biologics. Infect Dis Clin North Am. 2020;34(2):341–58. 16. Pan C, Cao M, Yan C, et al. Hepatitis B virus reactivation associated with Janus kinase (JAK) inhibitors: A retrospective study of pharmacovigilance databases and review of the literature. Expert Opin Drug Saf. 2023;22(6):469–76. 17. Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology. 2015;148(1):221–44.e3.
留言 (0)