
記住我





Endoscopic ultrasound–guided choledochoduodenostomy (EUS-CD) is a biliary drainage procedure that was first described in 2001.1,2 This procedure has become an acceptable alternative to percutaneous transhepatic biliary drainage for patients with malignant biliary obstruction in whom endoscopic retrograde cholangiopancreatography (ERCP) has failed or is not technically feasible.
A meta-analysis showed no significant increase in complication rate with EUS-CD in comparison with ERCP when used first in patients with malignant biliary obstruction.3 EUS-CD was found to be a technically and clinically highly successful procedure with less need for reintervention when compared with percutaneous biliary drainage.4 EUS-CD with lumen-apposing metal stent (LAMS) has gained more favor over straight metal biliary stents, despite being a technically challenging procedure with a relatively steep learning curve. One of the less studied technical challenges to EUS-CD is the presence of a duodenal stent. Very few case reports were published for EUS-CD with an LAMS through a previously placed duodenal stent.1,5–7 In this study, we present 2 EUS-CD with LAMS cases with a particular technical challenge in one case in which we demonstrate a salvage technique.
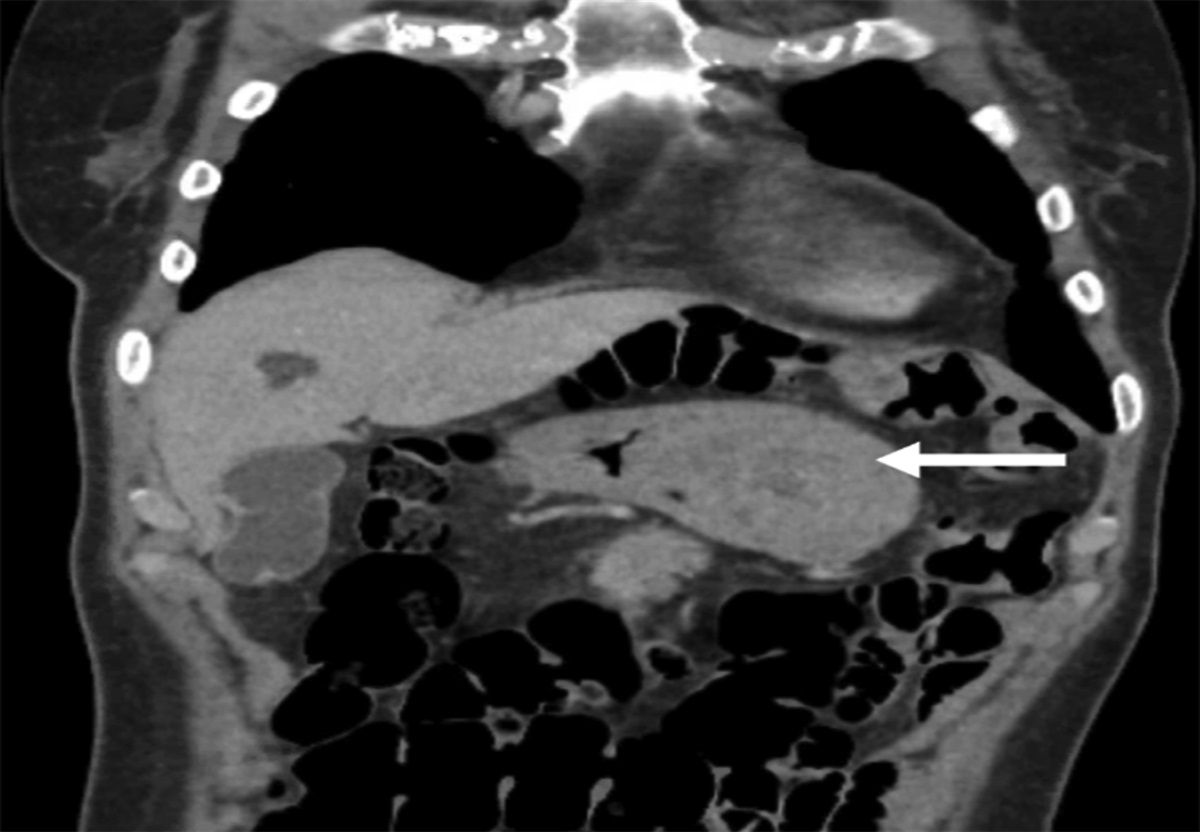
CASE REPORT Case 1A 78-year-old female patient with an 8-month history of unresectable pancreatic head cancer. She initially had ERCP, with a metal biliary stent placement for common bile duct (CBD) obstruction followed, 5 months later, by a duodenal stent placement to relieve a duodenal obstruction by the pancreatic neoplasia. One month after the duodenal stent placement, the patient presented with obstructive jaundice. Abdominal computed tomography (CT) showed obstruction of the distal end of the biliary stent with dilated CBD up to 2.1 cm and dilated intrahepatic bile ducts. Her liver panel showed total bilirubin (TB): 8.36 mg/dL, alkaline phosphatase (ALP): 448 IU/L, and alanine transaminase (ALT): 111 IU/L. The patient was started on piperacillin-tazobactam. ERCP was attempted but failed because of extensive tumor growth inside the duodenal stent. EUS-guided biliary drainage was then considered. The EUS examination showed the CBD dilated up to 23 mm and was 4–5 mm from the duodenal wall. The proximal end of the duodenal stent was located in the mid-duodenal bulb, so the possibility of puncturing through the duodenal stent was taken into consideration. Under EUS control, the dilated portion of the CBD was punctured with a Hot AXIOS device (6 × 8 mm; Boston Scientific) using pure cut current 100 W without guidewire. There was no resistance at the puncture point and after confirming the choledochobulbar apposition, the LAMS was successfully deployed through the duodenal stent, and it successfully opened inside the duodenal stent lumen followed by a gush of purulent bile (Video 1). No postprocedural complications occurred. The patient was started on an oral diet 4 hours after the procedure. The next day, the TB level went down to 3.57 mg/dL and was normalized a few days later. Twelve days later, the patient needed a second duodenal stent placement to relieve the symptomatic duodenal stent obstruction. At her 1-month follow-up, the serum bilirubin level was normal, and she did not have any duodenal obstruction symptoms.
Case 2An 83-year-old male patient with metastatic gastric antral adenocarcinoma, who had a gastroduodenal stent previously placed for gastric outlet obstruction, was referred for obstructive jaundice. Abdominal CT showed metastatic lymph nodes in the liver hilum with dilated intrahepatic bile ducts and dilated proximal CBD up to 20 mm. The liver panel showed TB: 12. 98 mg/dL, direct bilirubin: 10.94 mg/dL, ALP: 618 IU/L, and ALT: 123 IU/L. The patient was started on piperacillin-tazobactam. ERCP was not successful because of difficult duodenal intubation and inadequate positioning through the duodenal metallic stent. EUS-CD was then attempted. The tip of the echoendoscope could be inserted into the duodenal bulb through the gastroduodenal stent. There was significant mucosal granularity induced by the indwelling duodenal stent. The EUS examination estimated the duodenal bulb wall thickness to be around 2.5 mm. The proximal CBD was dilated up to 20 mm with a measured distance of 8 mm from the duodenal wall.
We decided to attempt EUS-CD through the duodenal stent, given the unsuccessful ERCP approach. With a stable echoendoscopic position in the duodenal bulb, the dilated CBD was directly punctured with a HOT AXIOS device (6 × 8 mm) using a pure cut current 100 W with no resistance at the duodenal wall. The distal stent flange was released under EUS guidance inside the CBD and was retracted until a cone shape was observed confirming the choledochal-bulbar apposition. The proximal stent flange was then deployed inside the echoendoscope and released. Dark-colored bile was immediately seen coming through the duodenal stent. Nevertheless, the proximal LAMS flange could not be observed.
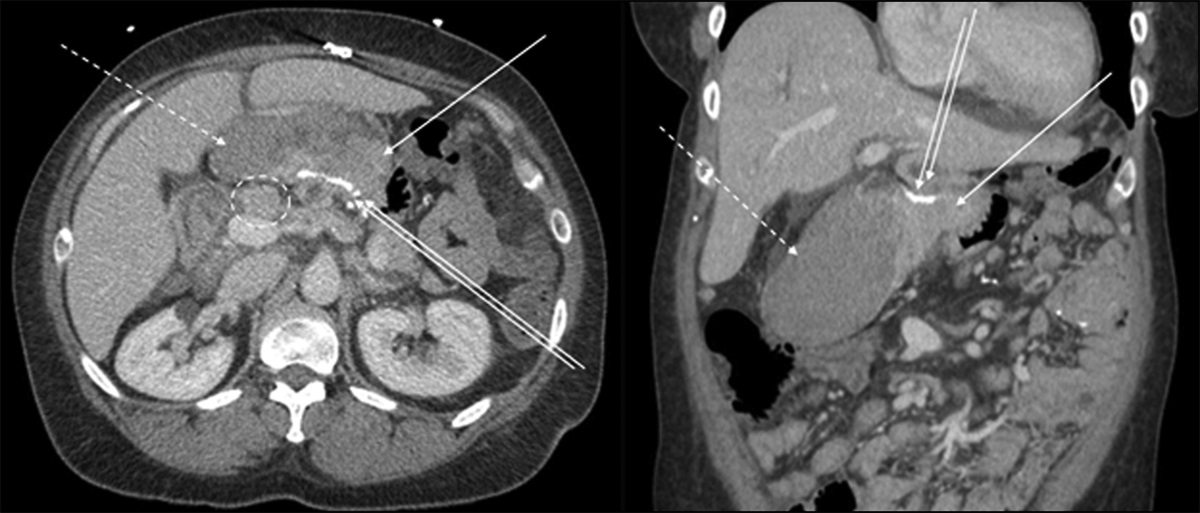
Under fluoroscopy, pneumobilia was observed inside the CBD with no signs of pneumoperitoneum or pneumoretroperitoneum. The duodenal end of the LAMS was seen deployed behind the duodenal stent (Figure 1A and B). A guidewire was immediately inserted through the AXIOS system to secure the stent track. Bile flow gradually stopped as the duodenal (proximal) LAMS flange was embedded in the duodenal bulb wall. At this point, the procedural success was totally uncertain. Contrast was injected through a balloon catheter that was placed over the guidewire through the LAMS (Figure 1C). There was no sign of leak outside the biliary tree.
 Figure 1.:
Figure 1.: (A and B) The duodenal end of the LAMS deployed behind the duodenal stent. (C) Injected contrast through a balloon catheter, placed over the guidewire through the LAMS without sign of leak outside the biliary tree. (D) The stent flange positioned within the duodenal stent lumen, via the LAMS, without pneumoperitoneum on x-ray.
An immediate solution was needed to salvage the embedded part of the LAMS and ensure adequate biliary drainage. A single flange head, partially covered metal stent (Hanarostent Biliary Flange NCN 10 × 80 mm; M.I.TECH, South Korea) was successfully placed and deployed over the guidewire under endoscopic and fluoroscopic control. The stent flange was well placed inside the duodenal stent lumen (Video 2). The uncovered part was placed inside the CBD, whereas the covered part was placed through the LAMS and the duodenal wall. Dark bile flow was again observed. There was no sign of pneumoperitoneum on the postprocedural x-ray (Figure 1D). In 48 hours, the liver panel significantly improved (TB: 4.91 mg/dL, direct bilirubin: 4.21 mg/dL, ALP: 310 IU/L, and ALT: 67 IU/L). The patient was started on an oral diet the next day after the procedure. There were no signs of complications on a follow-up abdominal CT scan. Despite the improvement of the liver function tests, the patient suffered from appetite loss and became progressively frail. He opted for hospice care.
DISCUSSIONEUS-CD is a well-described alternative in cases of failed ERCP. When a duodenal metal stent was initially placed, EUS-CD has been traditionally performed using straight metal biliary stents with certain caveats such as migration and bile leak because of inadequate coaptation between the CBD and the duodenal wall. There is one previous report of successful LAMS EUS-CD through a previously placed duodenal stent. In terms of determining stent size, the smaller size of LAMS of 6-mm diameter and 8-mm saddle length has generally been better adapted to the CBD size, especially with dilatation less than 15 mm. We opted this typical stent size to allow for easier passage through the duodenal stent.
In this report, our first case was a successful demonstration of the feasibility of EUS-CD with LAMS through a previously placed duodenal stent. In our second case, the LAMS proximal flange was inadequately deployed behind the duodenal stent and was embedded in the duodenal wall. The placement of the proximal end of the duodenal stent through the pylorus in the gastric lumen may have played a role in preventing adequate contact between the echoendoscope tip and the duodenal bulb wall. In this particular case, the duodenal stent-induced bulbar mucosal granularity and inflammation may have also played a role in the inadequate deployment. The 2 aforementioned factors may have together contributed to the faulty deployment of the proximal flange behind the duodenal stent and its embedment in the duodenal wall. In retrospect, a larger size LAMS 10-mm lumen diameter × 10-mm saddle length may have been a better option to accommodate the space occupied by the duodenal stent in addition to the duodenal wall. The single flange partially covered straight biliary metal stent proved to be a successful option to salvage the embedded LAMS, with no complication 2 weeks after the procedure and progressive improvement in the liver function tests.
EUS-CD with LAMS placement through duodenal stents needs further evaluation and comparison with EUS-CD with straight single flange metal stents to assess the technical caveats and success rates in different clinical scenarios and duodenal stent positions, to determine the most adapted stent type for this particular indication.
DISCLOSURESAuthor contributions: M. Elmassry, B. Hache, and J. Thongpiya wrote the original draft, preparing figures and videos. Y. Shiratori and G. Rateb reviewed and edited the manuscript. G. Rateb is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
,,]},,]}REFERENCES 1. Mangiavillano B, Kunda R, Robles-Medranda C, et al. Lumen-apposing metal stent through the meshes of duodenal metal stents for palliation of malignant jaundice. Endosc Int Open. 2021;9(3):E324–E330. 2. Iwashita T, Doi S, Yasuda I. Endoscopic ultrasound-guided biliary drainage: A review. Clin J Gastroenterol. 2014;7(2):94–102. 3. Han SY, Kim SO, So H, Shin E, Kim DU, Park DH. EUS-guided biliary drainage versus ERCP for first-line palliation of malignant distal biliary obstruction: A systematic review and meta-analysis. Sci Rep. 2019;9(1):16551. 4. Sawas T, Bailey NJ, Yeung KYKA, et al. Comparison of EUS-guided choledochoduodenostomy and percutaneous drainage for distal biliary obstruction: A multicenter cohort study. Endosc Ultrasound. 2022;11(3):223–30. 5. De Davide L, Bureau MA, Manière T, Toliopoulos P, Désilets É. EUS biliary drainage with a lumen-apposing metal stent through a pre-existing duodenal metal stent. VideoGIE. 2019;4(3):131–2. 6. Sportes A, Airinei G, Kamel R, Raynaud JJ, Benamouzig R. Endoscopic ultrasound-guided choledochoduodenostomy with a lumen-apposing metal stent through an uncovered metal duodenal stent. Endosc Int Open. 2018;6(12):E1395–7. 7. Mohapatra S, Fukami N. EUS–guided choledochoduodenostomy using a lumen-apposing metal stent in a patient with preexisting duodenal stent and ascites. VideoGIE. 2022;7(11):398–400.
留言 (0)