
記住我


Chronic pancreatitis (CP) is a progressive disease characterized by fibrosis and inflammation of the pancreas, which is caused by genetic and environmental factors (1). Morphological changes, including atrophy, fibrosis, duct distortion, and strictures, and calcification lead to irreversible damage to pancreatic endocrine and exocrine functions. Abdominal pain is the most dominant clinical feature of CP. Both the recurrent pain and the development of pancreatic insufficiency contribute to poor quality of life and increase mental and economic burdens for patients (2).
Female patients account for around 30% of all CP patients (3). The course of CP may cover the duration of childbearing age; therefore, there are concerns about the fertility and outcomes of pregnancies in female CP patients. There is a paucity of studies focused on the effect of CP on pregnancy outcomes, with inconsistent conclusions. One study by Mahapatra et al (4) enrolled 99 CP patients and found no increased risk of CP on adverse maternal and fetal outcomes. Another retrospective study of 46 patients by Rana et al (5) also found that CP was not associated with adverse pregnancy outcomes. Both of the above studies had relatively small sample sizes and were designed as retrospective studies. The most recent population-based study conducted by Niu et al (6) analyzed the clinical data of 3,094 CP patients obtained from the US National Inpatient Sample database and concluded that CP was associated with elevated rates of adverse pregnancy outcomes, such as gestational diabetes mellitus (GDM) (adjusted odds ratios [AOR], 1.63), gestational hypertensive complications (AOR, 2.48), preterm labor (AOR, 3.10), and small for gestational age (AOR, 2.40). To date, no study has focused on the risk factors for adverse pregnancy outcomes among CP patients.
Different from the etiology of male patients, which is predominated by alcoholic CP, the most common etiology of female patients is idiopathic CP (ICP) (7), which is characterized by high rates of CP-susceptibility gene mutations. Genetic factors are known to play important roles in the development, clinical manifestations, and progression of CP. SPINK1 (encoding pancreatic secretory trypsin inhibitor), PRSS1 (encoding cationic trypsinogen), CTRC (encoding chymotrypsin C), and CFTR (encoding cystic fibrosis transmembrane conductance regulator) are the 4 major germline susceptibility genes for CP (8). Our previous study (7) of 1,061 Chinese CP patients found that 50.42% of patients harbored at least one rare pathogenic variant in the above 4 genes; these variants were associated with earlier median ages at disease onset and diagnosis of pancreatic stones, diabetes mellitus, and steatorrhea. Muller et al (9) also found that SPINK1-related pancreatitis was associated with earlier onset and pancreatic insufficiencies, based on a European cohort of 209 CP patients with gene mutations. It is also known that germline genetic alterations significantly contribute to reproductive failure. Thus, whether variants in CP-susceptibility genes impact pregnancy outcomes in female CP patients is worthy of further exploration.
Given the current uncertainty regarding the pregnancy outcomes of CP patients with or without gene mutations, this study explored the effects of genetic factors on pregnancy outcomes using a well-phenotyped cohort of Chinese female CP patients. The aim was to provide valuable information to assist maternal healthcare providers in counseling female CP patients and identifying those at high risk of adverse pregnancy outcomes to inform clinical decision-making.
METHODS Study setting and patientsThis prospective observational study was performed at Changhai Hospital. Female CP patients from January 2010 to December 2014 were enrolled in the study after informed consent was obtained. Study participants provided a blood sample for genetic testing. The study was approved by the Institutional Review Board of Changhai Hospital (CHEC2020-008), and all procedures were performed according to the ethical standards in the Declaration of Helsinki. All diagnostic and therapeutic procedures were performed according to the approved guidelines.
Patients were under regular annual follow-up as described in our previous study (3). The patients' clinical features and pregnancy-related data were updated by telephone. Data for this study were obtained in May 2023. The exclusion criteria were (i) patients without documented pregnancy, (ii) patients who refused to provide pregnancy-related information or those with incomplete pregnancy data, and (iii) patients with other autoimmune comorbidities that might influence pregnancy outcomes, such as systemic lupus erythematosus and autoimmune thyroid diseases.
Genetic testingThis study examined 4 major CP-susceptibility genes, i.e., the SPINK1, PRSS1, CTRC, and CFTR genes. A detailed description of the procedures for DNA preparation and gene sequencing has been provided previously (7). Known rare pathogenic gene mutations (those with a minor allele frequency of <1% in the general population) were included in the final analysis.
OutcomesThe outcome was a composite variable of adverse pregnancy outcomes, including adverse maternal outcomes (CP-associated cesarean delivery, CP-associated preterm delivery, GDM, intrahepatic cholestasis of pregnancy, and hypertensive disorders of pregnancy [HDP]) and adverse fetal outcomes (low birth weight, CP-associated abortion, congenital anomaly, and stillbirth).
DefinitionsThe diagnosis of CP was established according to the Asia-Pacific consensus (10). Alcoholic CP was defined as alcohol intake of ≥60 g/d for at least 2 years. Hereditary CP was defined as more than 2 first-degree relatives or more than 3 second-degree relatives with CP or recurrent acute pancreatitis. Other etiologies of CP included abnormal anatomy of the pancreatic duct, trauma, and so forth. ICP was diagnosed when none of the known causes were identified (3). Diabetes was diagnosed according to the diagnostic criteria of the American Diabetes Association (11). Steatorrhea was diagnosed in accordance with our previous study (7). Pseudocysts, portal hypertension, and biliary stricture were diagnosed on imaging examination (12).
The pregnancy outcomes in this study were defined as follows. CP-associated cesarean delivery was defined as cesarean delivery because of acute attacks of CP or comorbidities associated with CP, such as GDM or HDP (6). Acute attacks of CP could be diagnosed if at least 2 of the following 3 criteria were fulfilled: (i) The current attack displayed typical abdominal pain, (ii) serum lipase or amylase level was at least 3 times the upper limit of normal, and (iii) ultrasonography showed morphological changes in the pancreas. CP-associated preterm delivery was defined as preterm delivery (i.e., delivery at less than 37 weeks' gestation (13)) because of acute attacks of CP or comorbidities associated with CP. GDM was defined as the onset or first recognition of abnormal glucose tolerance during pregnancy (14). The diagnosis of intrahepatic cholestasis of pregnancy was based on characteristic symptoms and elevated serum bile acids in the absence of other hepatobiliary diseases (15). HDP included preeclampsia/eclampsia, chronic hypertension with/without superimposed preeclampsia, and gestational hypertension (16). Low birth weight was defined as a weight <2,500 g at birth (17). CP-associated abortion was defined as abortion (i.e., pregnancy loss before 28 weeks' gestation (18)) because of acute attacks of CP or comorbidities associated with CP. Congenital anomaly was defined as inborn errors of development (19). Stillbirth was defined as a fetus ≥20 weeks' gestation with no signs of life (20).
Statistical analysisFor continuous variables, tests of data normality were performed using the Shapiro-Wilk test. Normally distributed variables were presented as mean ± SD and were compared using Student t tests; non-normally distributed variables were presented as median (interquartile range [IQR]) and were compared using Mann-Whitney U tests. Categorical variables were presented as frequencies and percentages. χ2 analysis or Fisher exact test was used for the comparison of categorical variables. Two-sided P values <0.05 were considered statistically significant. For multiple comparisons, Bonferroni adjustment was applied. Variables with a P value <0.05 in the univariate analysis were included in the multivariate logistic regression model. For multivariate analysis, the likelihood ratio statistic was calculated with an “enter” logistic regression model. AORs and 95% confidence intervals (CIs) were calculated. Data were analyzed using SPSS version 23 (SPSS, Chicago, IL).
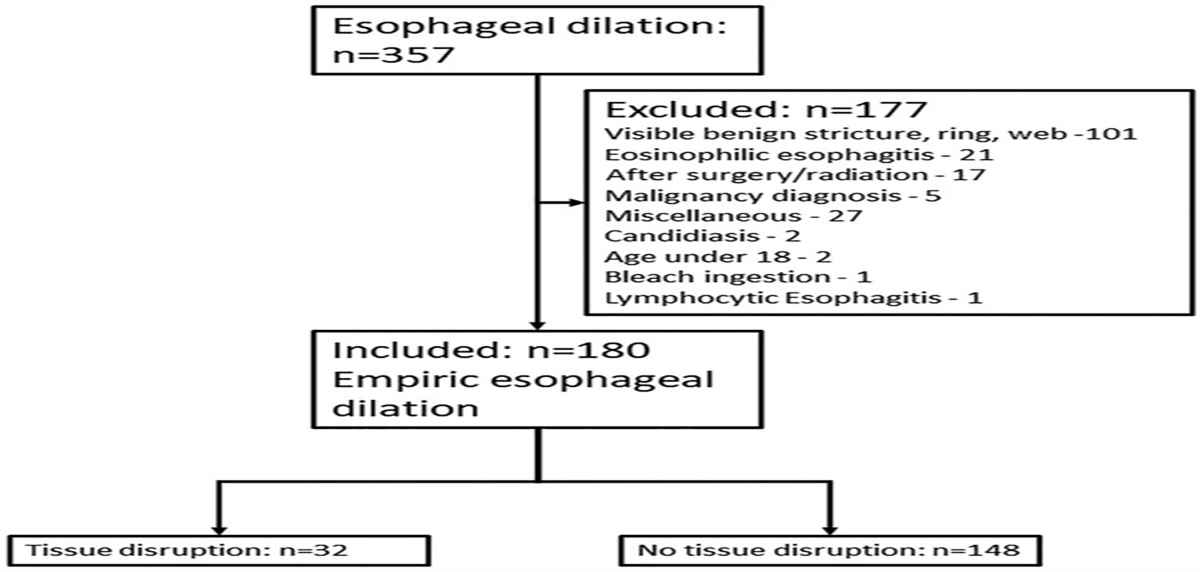
RESULTS General characteristics of the enrolled patientsThe enrollment flow diagram is shown in Figure 1. A total of 292 females from our previously reported prospective Chinese CP cohort (3) were enrolled. After the application of the exclusion criteria, 42 patients without documented pregnancy, 47 patients who refused to provide pregnancy-related information, 38 patients without complete pregnancy-related information, and 5 patients with other autoimmune comorbidities that might influence pregnancy outcomes were excluded from this study. Finally, data from 160 patients who had known genetic backgrounds and a pregnancy history were analyzed.
 Figure 1.:
Figure 1.: Flowchart of study participants. CP, chronic pancreatitis.
The characteristics of the cohort are presented in Table 1. At least one rare pathogenic mutation in the 4 genes mentioned above was identified in 95 patients (59.4%). Among these, SPINK1 mutations were the most common, observed in 67 patients (41.9%). Compared with patients without gene mutations, more patients with gene mutations were classified as ICP (P < 0.001), and the prevalence of pseudocysts was lower (7.4% vs 18.5%, P = 0.033).
Table 1. - Characteristics of the enrolled patients Total (n = 160) Patients with gene mutations (n = 95) Patients without gene mutations (n = 65) P Age at diagnosis of CP, yr (IQR) 38.5 (27.0–48.0) 33.0 (24.0–41.0) 46.0 (35.5–54.0) <0.001 Age at onset of CP, yr (IQR) 32.5 (22.0–44.0) 29.0 (19.0–39.0) 42.0 (29.5–50.5) <0.001 Age at the end of follow-up, yr (IQR) 49.5 (38.9–58.0) 44.0 (37.0–53.0) 56.0 (46.5–64.0) <0.001 Smoking history, n (%) 4 (2.5) 1 (1.1) 3 (4.6) 0.367 Alcohol use, n (%) 4 (2.5) 1 (1.1) 3 (4.6) 0.367 Age at marriage, yr (IQR) 24.0 (22.0–26.0) 24.0 (22.5–26.0) 23.0 (21.0–26.0) 0.055 Age at first pregnancy, yr (IQR) 25.0 (22.0–28.0) 25.0 (23.0–28.0) 24.0 (22.0–27.8) 0.278 Age at first delivery, yr (IQR) 25.0 (23.0–28.0) 25.0 (23.0–28.0) 24.0 (22.0–27.8) 0.237 Onset symptoms, n (%) 0.565 Pain 50 (31.3) 33 (34.7) 17 (26.2) AP 78 (48.8) 41 (43.2) 37 (56.9) Diabetes 14 (8.8) 9 (9.5) 5 (7.7) Steatorrhea 10 (6.3) 7 (7.4) 3 (4.6) Asymptomatic 8 (5.0) 5 (5.3) 3 (4.6) Etiology of CP, n (%) <0.001 Idiopathic 131 (81.9) 84 (88.4) 47 (72.3) Alcoholic 4 (2.5) 1 (1.1) 3 (4.6) Hereditary 6 (3.8) 6 (6.3) 0 (0.0) Othersa 19 (11.9) 4 (4.2) 15 (23.1) Complications of CP, n (%) Diabetes 48 (30.0) 28 (29.5) 20 (30.8) 0.861 Steatorrhea 36 (22.5) 24 (25.3) 12 (18.5) 0.312 Pseudocyst 19 (11.9) 7 (7.4) 12 (18.5) 0.033 Portal hypertension 6 (3.8) 3 (3.2) 3 (4.6) 0.958 Biliary stricture 4 (2.5) 3 (3.2) 1 (1.5) 0.897 Pancreatic cancer 0 (0.0) 0 (0.0) 0 (0.0) — Gene mutations, n (%) 95 (59.4) — — — SPINK1 mutations 67 (41.9) 67 (70.5) — — PRSS1 mutations 24 (15.0) 24 (25.3) — — CTRC mutations 6 (3.8) 6 (6.3) — — CFTR mutations 16 (10.0) 16 (16.8) — — Acute pain attack during pregnancy, n (%) 13 (8.1) 10 (10.5) 3 (4.6) 0.179 ERCP and/or ESWL, n (%) 156 (97.5) 95 (100.0) 61 (93.8) 0.053 Surgery, n (%) 10 (6.3) 5 (5.3) 5 (7.7) 0.771AP, acute pancreatitis; CP, chronic pancreatitis; ERCP, endoscopic retrograde cholangiopancreatography; ESWL, extracorporeal shock wave lithotripsy; IQR, interquartile range.
aOther etiology of CP includes abnormal anatomy of pancreatic duct and trauma.
The pregnancy outcomes of the patients are shown in Table 2 and Supplementary Digital Content (see Supplementary Figure 1, https://links.lww.com/CTG/B93). There was a total of 364 pregnancies and 227 deliveries among the enrolled patients. CP-associated adverse pregnancy outcomes occurred in 38 patients (23.8%).
Table 2. - Pregnancy outcomes of female CP patients with and without gene mutations Total (n = 160) Patients with gene mutations (n = 95) Patients without gene mutations (n = 65) P No. of pregnancies per woman, median (IQR) 2 (1–3) 2 (1–3) 2 (1–3) 0.604 No. of deliveries per woman, median (IQR) 1 (1–2) 1 (1–2) 1 (1–2) 0.069 Delivery, n (%) 157 (98.1) 93 (97.9) 64 (98.5) 1.000 CP-associated adverse pregnancy outcomes, n (%) 38 (23.8) 29 (30.5) 9 (13.8) 0.015 CP-associated adverse maternal outcomes, n (%) 25 (15.6) 19 (20.0) 6 (9.2) 0.065 CP-associated cesarean delivery 19 (11.9) 15 (15.8) 4 (6.2) 0.064 CP-associated preterm delivery 14 (8.8) 12 (12.6) 2 (3.1) 0.036 Gestational diabetes mellitus 4 (2.5) 3 (3.2) 1 (1.5) 0.897 Intrahepatic cholestasis of pregnancy 1 (0.6) 1 (1.1) 0 (0.0) 1.000 Hypertensive disorders of pregnancy 5 (3.1) 4 (4.2) 1 (1.5) 0.623 Gestational hypertension 4 (2.5) 3 (3.2) 1 (1.5) 0.897 Eclampsia 1 (0.6) 1 (1.1) 0 (0.0) 1.000 CP-associated adverse fetal outcomes, n (%) 27 (16.9) 21 (22.1) 6 (9.2) 0.033 Low birth weight 10 (6.3) 7 (7.4) 3 (4.6) 0.708 CP-associated abortion 20 (12.5) 17 (17.9) 3 (4.6) 0.013 Congenital anomaly 2 (1.3) 2 (2.1) 0 (0.0) 0.515 Stillbirth 2 (1.3) 1 (1.1) 1 (1.5) 1.000CP, chronic pancreatitis; IQR, interquartile range.
Patients with gene mutations had a significantly higher incidence of CP-associated adverse pregnancy outcomes than those without (30.5% vs 13.8%, P = 0.015). In terms of maternal outcomes, the overall incidence of adverse outcomes was higher in patients with gene mutations, and this difference was borderline significant (20.0% vs 9.2%, P = 0.065). Notably, the proportion of CP-associated preterm deliveries was remarkably higher in patients with gene mutations (12.6% vs 3.1%, P = 0.036). For fetal outcomes, the overall incidence of adverse outcomes was significantly higher in patients with gene mutations (22.1% vs 9.2%, P = 0.033). Moreover, there was a significant difference between the 2 groups in the proportion of CP-associated abortion (17.9% vs 4.6%, P = 0.013) (Table 2).
Gene mutation distribution in patients with and without adverse pregnancy outcomesThe distribution of gene mutations in patients with and without adverse pregnancy outcomes is shown in Table 3. The prevalence of SPINK1 mutations (57.9% vs 36.9%, P = 0.022), as well as the most common variant c.194 + 2T>C (57.9% vs 33.6%, P = 0.007), was significantly higher in those with adverse pregnancy outcomes compared with those without. The distributions of gene mutations in patients with CP-associated preterm delivery and abortion, the 2 most serious adverse events, are shown in Supplementary Digital Content (see Supplementary Table 1, https://links.lww.com/CTG/B93).
Table 3. - Distribution of CP-susceptibility gene mutations in patients with and without adverse pregnancy outcomes Patients with adverse pregnancy outcomes (n = 38) Patients without adverse pregnancy outcomes (n = 122) P Gene mutations, n (%) 29 (76.3) 66 (54.1) 0.015 SPINK1 mutations 22 (57.9) 45 (36.9) 0.022 c.194 + 2T>C 22 (57.9) 41 (33.6) 0.007 c.101A>G 1 (2.6) 3 (2.5) 1.000 c.202C>T 0 (0.0) 1 (0.8) 1.000 c.206C>T 1 (2.6) 0 (0.0) 0.238 c.75C>G 1 (2.6) 0 (0.0) 0.238 PRSS1 mutations 7 (18.4) 17 (13.9) 0.499 c.86A>T 2 (5.3) 2 (1.6) 0.239 c.346C>T 0 (0.0) 2 (1.6) 1.000 c.364C>T 0 (0.0) 1 (0.8) 1.000 c.365G>A 3 (7.9) 3 (2.5) 0.293 c.623G>C 2 (5.3) 9 (7.4) 0.934 CTRC mutations 1 (2.6) 5 (4.1) 1.000 c.180C>T 0 (0.0) 4 (3.3) 0.573 c.181G>A 0 (0.0) 1 (0.8) 1.000 c.649G>A 1 (2.6) 0 (0.0) 0.238 c.703G>A 1 (2.6) 0 (0.0) 0.238 CFTR mutations 2 (5.3) 14 (11.5) 0.421 c.1865G>A 0 (0.0) 1 (0.8) 1.000 c.2909G>A 0 (0.0) 2 (1.6) 1.000 c.2936A>C 1 (2.6) 1 (0.8) 0.420 c.3205G>A 0 (0.0) 2 (1.6) 1.000 c.3635delT 0 (0.0) 1 (0.8) 1.000 c.4056G>C 1 (2.6) 7 (5.7) 0.733CP, chronic pancreatitis.
The impact of genetic factors and clinical features on adverse pregnancy outcomes was further explored in univariate and multivariate analyses. In univariate analyses, harboring gene mutations (P = 0.017) and acute pain attack during pregnancy (P = 0.003) were associated with adverse pregnancy outcomes. These variables were then included in a subsequent multivariate analysis. In the final multivariate logistic regression model, harboring gene mutations (OR, 2.52; 95%CI, 1.08–5.90; P = 0.033) and acute pain attack during pregnancy (OR, 5.63; 95%CI, 1.68–18.87; P = 0.005) were identified as independent risk factors for adverse pregnancy outcomes (Table 4).
Table 4. - The impact of genetic factors and clinical features on adverse pregnancy outcomes in CP (n = 160) Comparison of characteristics Univariate analyses Multivariate analyses Patients with adverse pregnancy outcomes (n = 38) Patients without adverse pregnancy outcomes (n = 122) OR (95% CI) P OR (95% CI) P Smoking history, n (%) 1 (2.6) 3 (2.5) 1.07 (0.11–10.62) 0.953 Alcohol use, n (%) 1 (2.6) 1 (0.8) 3.27 (0.20–53.57) 0.406 Age at first pregnancy, yr (IQR) 25.0 (23.0–28.0) 24.0 (22.0–27.0) 1.09 (0.98–1.20) 0.113 Age at first delivery, yr (IQR) 26.0 (24.0–28.8) 25.0 (22.0–27.0) 1.11 (1.00–1.23) 0.063 Onset symptoms, n (%) Pain 12 (31.6) 38 (31.1) Reference AP 20 (52.6) 58 (47.5) 1.09 (0.48–2.49) 0.834 Diabetes 4 (10.5) 10 (8.2) 1.27 (0.34–4.78) 0.727 Steatorrhea 1 (2.6) 9 (7.4) 0.35 (0.04–3.07) 0.344 Asymptomatic 1 (2.6) 7 (5.7) 0.45 (0.05–4.06) 0.478 Etiology of CP, n (%) Idiopathic 31 (81.6) 100 (82.0) Reference Alcoholic 2 (5.3) 2 (1.6) 3.23 (0.44–23.86) 0.251 Hereditary 1 (2.6) 5 (4.1) 0.65 (0.07–5.73) 0.694 Othersa 4 (10.5) 15 (12.3) 0.86 (0.27–2.78) 0.802 Gene mutations, n (%) 29 (76.3) 66 (54.1) 2.73 (1.19–6.26) 0.017 2.52 (1.08–5.90) 0.033 Acute pain attack during pregnancy, n (%) 8 (21.1) 5 (4.1) 6.24 (1.90–20.45) 0.003 5.63 (1.68–18.87) 0.005AP, acute pancreatitis; CI, confidence interval; CP, chronic pancreatitis; IQR, interquartile range; OR, odds ratio.
aOther etiology of CP includes abnormal anatomy of pancreatic duct and trauma.
Next, the impact of SPINK1 mutations on pregnancy outcomes was explored. The characteristics and pregnancy outcomes of patients with and without SPINK1 mutations are shown in Supplementary Digital Content (see Supplementary Table 2 and Supplementary Table 3, https://links.lww.com/CTG/B93). Patients with SPINK1 mutations had a significantly higher incidence of CP-associated adverse pregnancy outcomes than those without gene mutations (32.8% vs 13.8%, P = 0.010). The impact of SPINK1 mutations on adverse pregnancy outcomes was then explored. In the final multivariate logistic regression model, harboring SPINK1 mutations (OR, 2.60; 95%CI, 1.06–6.37; P = 0.037) and acute pain attack during pregnancy (OR, 5.50; 95%CI, 1.60–18.92; P = 0.007) were identified as independent risk factors for adverse pregnancy outcomes (Tab
留言 (0)