
記住我


Duodenal cancer is a rare but aggressive malignant neoplasm, accounting for 0.5% of all gastrointestinal tumors.1 As patients present with nonspecific symptoms, the diagnosis of duodenal cancer is often delayed. For patients who undergo surgical resection for duodenal cancer, the 5-year survival rate ranges from 18% to 71%.2–6 Most previous studies have reported lymph node involvement as a significant prognostic factor. Moreover, age, tumor size, and tumor, node, metastasis (TNM) staging have been inconsistently reported in various reports.4–6 Due to the rarity of duodenal cancer, the use of tumor markers for this disease has not yet been investigated.
In recent years, liquid biopsies have ushered in a new era of tumor detection, monitoring, and molecular targeting therapies by enabling the noninvasive investigation of blood and body fluids. In particular, analysis of cell-free deoxyribonucleic acid (cfDNA) has demonstrated promising predictive and prognostic value. Higher concentrations of cfDNA are detected in patients with cancer than the concentration in healthy individuals as a result of tumor cell apoptosis and necrosis.7 Additionally, cfDNA as a novel biomarker for the prediction of survival in patients with cancer has been applied in various aspects, including colorectal, pancreatic, breast, and lung cancer, etc.8–12 Nevertheless, the molecular potential of cfDNA has not been explored in duodenal cancer.
In the present study, plasma cfDNA levels were quantified in patients with duodenal cancer. This study aimed to determine the correlation between cfDNA levels and clinicopathological features. Furthermore, the prognostic efficiency of cfDNA levels in predicting the survival outcome of patients with duodenal cancer was also investigated.
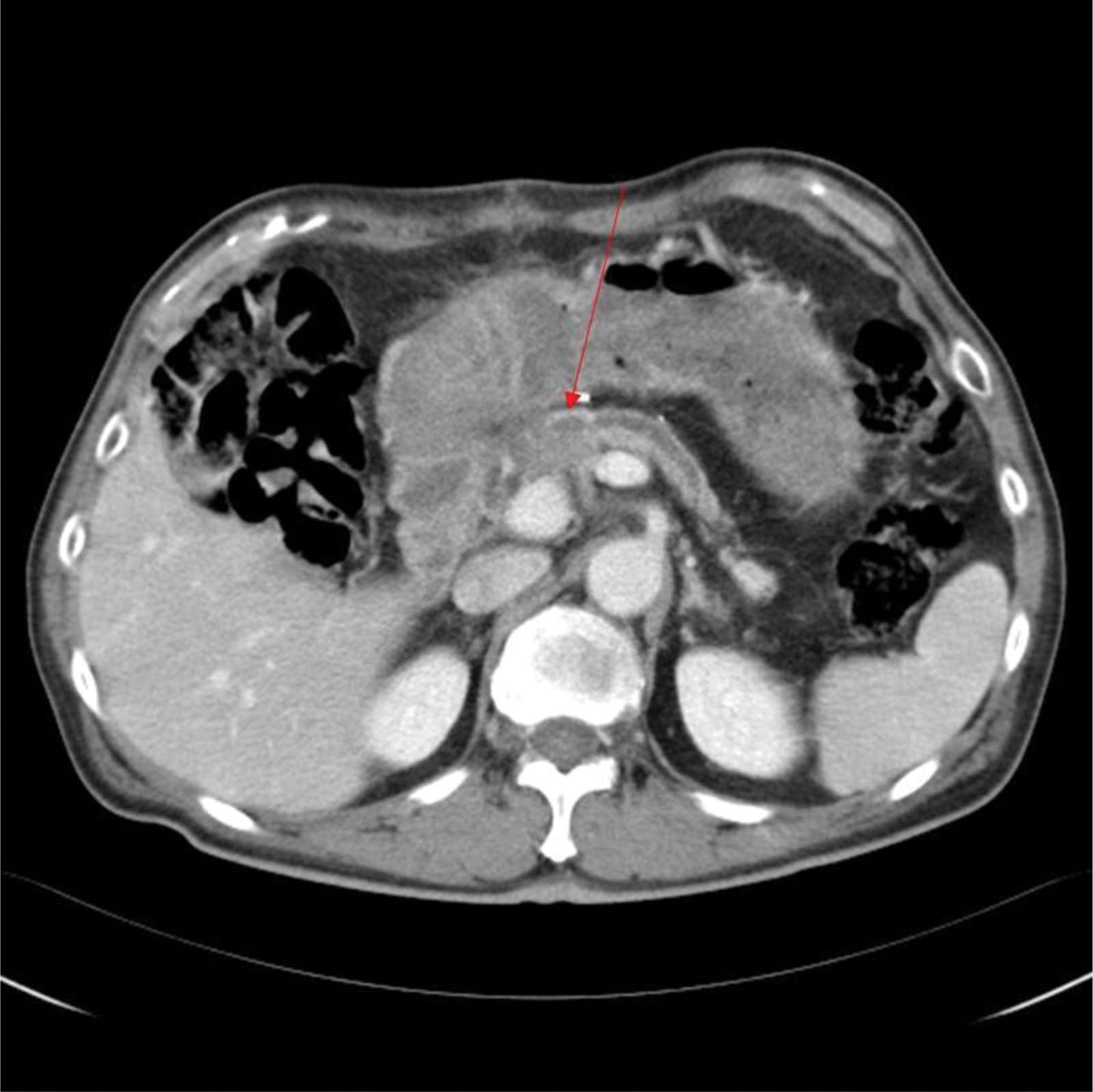
2. METHODSBetween June 2003 and July 2021, 41 patients were surgically treated for duodenal adenocarcinoma at the Department of Surgery, Taipei Veterans General Hospital. Pancreaticoduodenectomy was performed in most patients for radical resection and adequate lymphadenectomy. In a palliative setting, a gastrojejunal bypass was carried out. Data were prospectively collected into a computer database for subsequent retrospective analysis. All patients signed informed consent before entering the study and this study was approved by the Institutional Review Board (IRB) of the Taipei Veterans General Hospital (IRB-TPEVGH No. 2021-08-003CC). An assessment of cfDNA was carried out in combination with established prognostic clinicopathological and biochemical characteristics, including age, gender, tumor size, lymph node involvement, tumor cell differentiation, lymphovascular invasion, perineural invasion, carbohydrate antigen 19-9 (CA 19-9), carcinoembryonic antigen (CEA), and tumor stage. Univariate and multivariate analyses were conducted to identify independent prognostic factors for overall survival with a Cox proportional hazards regression model.
In contrast, a control group consisting of 95 healthy volunteers was recruited and their cfDNA levels were measured. They had undergone regular health checkups for at least 2 years before this study and were followed up for at least 2 years. No previous or subsequent malignant diseases were recorded before or after the blood sampling.
Peripheral blood samples were collected from patients with duodenal cancer before surgery and stored in the Biobank of Taipei Veterans General Hospital. In our study, circulating DNA was derived from nuclear DNA (NcirDNA). Furthermore, plasma cfDNAs were extracted using QIAamp® DNATissue Kit and Minelute Virus Kit (Qiagen, Valencia, CA) according to the protocol of the manufacturer. Plasma DNA was purified and quantified using a NanoDrop 1000 spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). A TaqMan quantitative polymerase chain reaction (qPCR) assay (Thermo Fisher Scientific) was used to quantify the cfDNA copy number of the housekeeping gene cyclophilin, which is not known to be correlated with cancer. Quantitative PCR was performed using the TaKaRa Ex Master Mix (Takara Bio, Shiga, Japan). The serially diluted standard DNA was used to generate a standard curve. The results are expressed as the threshold cycle (Ct), representing the PCR product’s cycle when it reached the detection threshold. The final Ct value was normalized based on the standard curve.
Statistical analyses were performed using Statistical Product and Service Solutions (version 20.0; IBM Corp., Armonk, NY, USA). All continuous variables were reported as median (range) and mean (standard deviation). A descriptive comparison of cfDNA levels was performed using a two-sample t test. All categorical variables are summarized as numbers and percentages and compared using Fisher’s exact test. Overall survival was estimated using the Kaplan–Meier method, and differences were evaluated using the log-rank test. The Cox proportional hazard model was used to identify the independent prognostic factors for overall survival. All tests were two-sided, and a p value <0.05 was considered statistically significant.
3. RESULTSForty-one patients with duodenal adenocarcinoma at our institute were included in the study. The mean age at diagnosis was 62.8 (±14.2) years (median 66 years, range 25-83 years). The cfDNA levels ranged from 5,332 to 26,852 copies/mL. The mean and median cfDNA levels in patients with duodenal cancer were 11,936 and 9288 copies/mL, respectively. We used 9288 copies/mL (median cfDNA level for all patients) as the cut-off cfDNA level. The 41 patients with duodenal cancer were divided into a low plasma cfDNA level group (≤9288 copies/mL) and a high plasma cfDNA level group (>9288 copies/mL). The control group consisted of 95 healthy individuals (66 male and 29 female) with a mean age of 54.2 ± 15.5 years. The cfDNA level of the control group ranged from 0 to 4157 copies/mL with a median of 168 copies/mL and a mean of 613 ± 888 copies/mL at our institute (Fig. 1). The predictive accuracy is demonstrated as a receiver operating characteristic (ROC) curve in Fig. 2. The area under the ROC curve (AUCs) for duodenal adenocarcinoma was 0.960 (95% CI, 0.913-0.984).
 Fig. 1:
Fig. 1: The scatterplot for healthy volunteers and duodenal adenocarcinoma. cfDNA = cell-free deoxyribonucleic acid.
 Fig. 2:
Fig. 2: ROC curve of cfDNA level for differentiating duodenal adenocarcinoma from healthy individuals. Plasma cfDNA level yielded an AUC of 0.960, with a 95% CI of 0.913-0.984. AUC = area under the curve; cfDNA = cell-free deoxyribonucleic acid; ROC = receiver operating characteristics.
The cfDNA levels were analyzed to determine their correlation with clinicopathological characteristics. No significant differences were observed in cfDNA levels according to age, sex, tumor size, lymph node involvement, tumor cell differentiation, lymphovascular invasion, perineural invasion, serum CA 19-9 or CEA levels, or pathological stage (Table 1).
Table 1 - Circulating cell-free DNA level in duodenal cancer patients according to various clinicopathological factors Correlation factor Circulating cell-free DNA level (copies/mL) p Mean (SD) Median Range Total, n = 41 11,936 (5835) 9288 5332-26,852 Age, y 0.48 ≤65, n = 17 11,156.94 (6,190) 8109 5676-26,852 >65, n = 24 12,488.71 (5638) 9694.5 5332-26,461 Sex 0.42 Male, n = 22 11,237.86 (5623) 8978 5332-26,852 Female, n = 19 12,745.47 (6122) 9568 5676-26,461 Tumor size, cm 0.48 ≤4, n = 23 12,517.52 (5782) 9568 6148-26,852 >4, n = 18 11,194.11 (5985) 8752 5332-26,461 Lymph node involvement 0.11 Negative, n = 19 10,246.89 (5437) 8625 5676-26,461 Positive, n = 21 13,198.24 (5961) 12,149 5332-26,852 Tumor cell differentiation 0.47 Well, n = 3 10,382.67 (6493) 8109 5332-17,707 Moderate, n = 27 11,344 (5692) 8625 5676-26,461 Poor, n = 8 14,148 (6967) 12,938 6703-26,852 Lymphovascular invasion 0.81 Negative, n = 15 11,773.87 (6389) 8871 5676-26,461 Positive, n = 22 12,268.64 (5835) 9729 5332-26,852 Perineural invasion 0.50 Negative, n = 16 12,845.94 (6328) 8871 5676-26,461 Positive, n = 21 11,475.38 (5782) 9718 5332-26,852 CA 19-9, U/mL 0.55 Normal ≤37, n = 23 12,834.78 (5945) 9568 5676-26,461 Abnormal >37, n = 14 11,587.86 (6156) 9299.5 5332-26,852 CEA, ng/mL 0.90 Normal ≤5, n = 29 12,138.93 (6167) 9085 5332-26,852 Abnormal >5, n = 10 12,418.10 (5123) 9984 6683-19,525 Stage 0.10 I and II, n = 19 10,246.89 (5437) 8625 5676-26,461 III and IV, n = 20 13,403.90 (6040) 16,565 5332-26,852CA 19-9 = carbohydrate antigen 19-9; CEA = carcinoembryonic antigen.
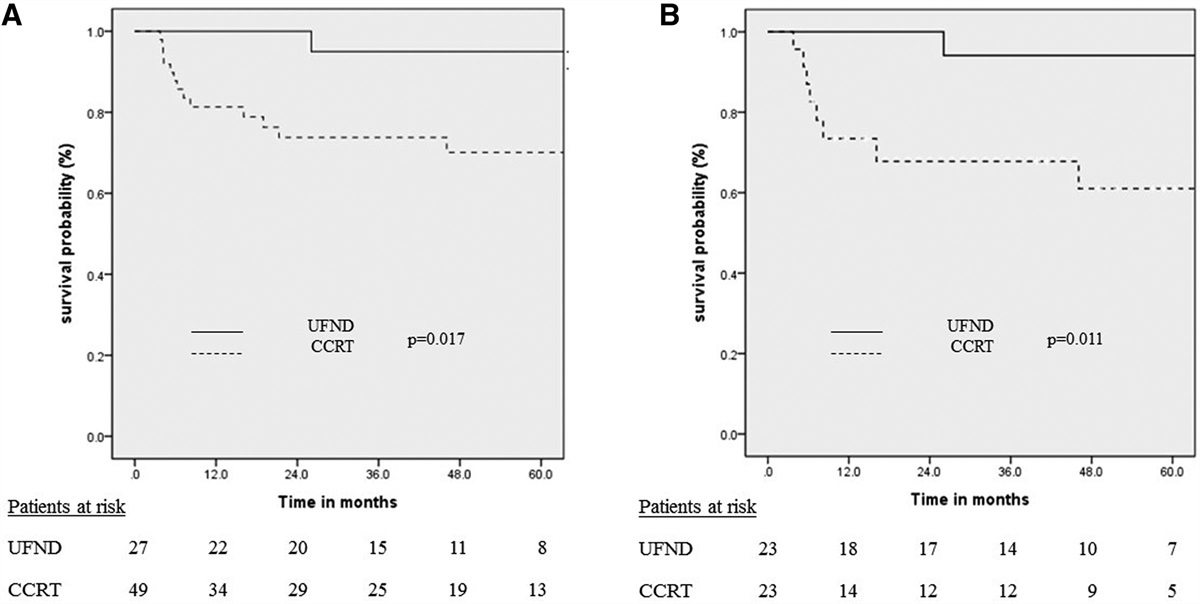
Of the 41 patients with duodenal adenocarcinoma, the overall survival rates were 77.8% at 1 year and 47.9% at 5 years, with a median survival time of 37.3 months. Univariate analysis demonstrated that high cfDNA level >9288 copies/mL, positive lymph node involvement, lymphovascular invasion, and advanced tumor stage were associated with decreased survival (p < 0.05; Table 2). Fig. 3 displays the components of the Kaplan–Meier curves for cfDNA levels. For patients with a low cfDNA level of ≤9288 copies/mL, the 1- and 5-year survival rates were 95.2% and 64.6%, respectively. As the cfDNA level increased, the survival rate progressively decreased, with 1- and 5-year survival rates of 58.7% and 17.6%, respectively, for patients with a high cfDNA level of >9288 copies/mL, p = 0.002). Multivariate analysis demonstrated that a high cfDNA level (odds ratio: 5.151; 95% CI, 1.424-18.637; p = 0.01) was the only independent prognostic factor for overall survival (Table 3).
Table 2 - Univariate analysis for prognostic factors of duodenal cancer undergoing surgical treatment Prognostic factors Survival time, mo 1-y survival 5-y survival p Mean (SD) Median Range Total, n = 41 60.4 (9.0) 37.3 0.1-136.3 77.8% 47.9% cfDNA level, copies/mL 0.002* Low (≤9288), n = 21 77.6 (10.8) 106.3 0.1-136.3 95.2% 64.6% High (>9288), n = 20 25.1 (6.7) 25.4 2.1-65.6 58.7% 17.6% Tumor size 0.24 ≤4 cm, n = 23 48.5 (10.7) 34.5 2.1-111.5 77.6% 37.7% >4 cm, n = 18 76.7 (14.4) 106.3 0.1-136.3 77.8% 57.6% Lymph node involvement 0.04* Negative, n = 19 76.3 (12.0) 106.3 5.2-136.3 84.2% 66.8% Positive, n = 21 30.2 (5.4) 25.4 0.1-62.5 70.8% 24.5% Tumor cell differentiation 0.73 Well, n = 3 43.4 (11.2) 17.7 16.0-57.1 100% 66.7% Moderate, n = 28 56.7 (9.6) 37.2 1.0-111.5 74.4% 48.1% Poor, n = 8 73.5 (28.0) 19.1 2.1-136.3 75.0% 50.0% Lymphovascular invasion 0.045* Negative, n = 15 85.2 (13.3) 107.9 7.0-111.5 86.7% 86.7% Positive, n = 22 50.1 (12.1) 33.4 0.1-136.3 72.4% 31.4% Perineural invasion 0.98 Negative, n = 16 67.0 (13.6) 72.0 2.5-111.5 80.8% 62.3% Positive, n = 21 73.3 (14.0) 37.2 0.1-136.3 76.2% 47.0% CA 19-9, U/mL 0.24 Normal ≤37, n = 23 54.9 (11.6) 37.3 0.1-107.9 68.8% 42.4% Abnormal >37, n = 14 77.0 (14.8) 106.3 2.1-136.3 85.7% 57.1% CEA, ng/mL 0.56 Normal ≤5, n = 29 58.6 (10.7) 37.2 0.1-136.3 72.4% 40.8% Abnormal >5, n = 10 67.0 (20.8) 107.9 2.5-107.9 90.0% 54.0% Stage 0.05* I and II, n = 19 76.3 (12.0) 106.3 5.2-136.3 84.2% 66.8% III and IV, n = 20 30.0 (5.8) 25.4 0.1-62.5 69.3% 27.2%*indicates statistical significance with p<0.05.
CA 19-9 = carbohydrate antigen 19-9; CEA = carcinoembryonic antigen; cfDNA = cell-free deoxyribonucleic acid.
*indicates statistical significance with p<0.05.
cfDNA = cell-free deoxyribonucleic acid.
 Fig. 3:
Fig. 3: Survival outcomes for patients with duodenal adenocarcinoma deteriorated with high cfDNA levels. For patients with a low cfDNA level ≤9288 copies/mL, the 1- and 5-y survival rates were 95.2% and 64.6%, respectively. The survival rate progressively decreased for the high cfDNA group, with the 1- and 5-y survival rates of 58.7% and 17.6%. p = 0.002. cfDNA = cell-free deoxyribonucleic acid.
4. DISCUSSIONDue to the low incidence of duodenal cancer, the prognostic significance of various clinicopathological factors has been debated in previous literature. Lymph node metastasis has been commonly reported to have a negative impact on the survival of patients with duodenal cancer.1,3,4,13 However, other authors have reported that lymph node involvement does not influence prognosis.5,14,15 Discrepancies have been identified in prognostic factors such as age, tumor size, resection margin, and TNM staging.4–6 In the current study, age, sex, tumor size, lymph node involvement, tumor cell differentiation, lymphovascular invasion, perineural invasion, serum CA 19-9 and CEA levels, and tumor stage were not associated with survival outcomes. An impediment to achieving satisfactory agreement on the importance of these traditional factors has prompted our exploration of new biomarkers.
Compared to patients without malignancy, Bronkhorst et al proved that patients with cancer had an increased concentration of circulating DNA.16 Rich literature has demonstrated the potential value of cfDNA as a prognostic factor in patients with colorectal, pancreatic, breast, and lung cancer.8–12 Moreover, cfDNAs derive from apoptotic and necrotic cells. Rapid and uncontrolled cell division leads to increased cell turnover, resulting in an increased proportion of cfDNA in patients with malignancies. In our cohort, the cfDNA levels in patients with duodenal adenocarcinoma were remarkably higher than those in normal controls. This result is consistent with those of the previous studies. Several studies have demonstrated that cfDNA level is a potential biomarker for the diagnosis and prognosis of tumors. The ability to discriminate cfDNA levels between patients with duodenal adenocarcinoma and healthy controls was excellent in our cohort, supporting the need for further studies on cfDNA screening. However, the presence of noncancerous comorbidities can introduce complexity and influence the interpretation of cfDNA data. Therefore, conducting thorough investigations into the impact of these comorbidities on cfDNA levels and patterns is essential.
Regarding the correlation between cfDNA levels and clinicopathological factors, a lack of association was observed between cfDNA levels and age, sex, tumor size, lymph node involvement, tumor cell differentiation, lymphovascular invasion, perineural invasion, serum levels of CA 19-9 or CEA, or pathological staging. This is likely due to the rarity of this malignancy and the small number of patients. Recent studies have demonstrated that the lymph node ratio, which is the ratio of positive lymph nodes to the number of lymph nodes excised, maybe a superior prognostic predictor.17 Nevertheless, large multicenter studies are needed to investigate the mechanistic associations.
In our study, according to the cut-off point of cfDNA level, the 41 patients with duodenal adenocarcinoma were divided into high plasma cfDNA and low plasma cfDNA level groups. The 1- and 5-year survival rates of patients with high plasma cfDNA levels were 58.7% and 17.6%, respectively, which were much lower than those of patients with low cfDNA levels. Multivariate analysis confirmed that only high cfDNA level was an independent prognostic factor. These data suggest that cfDNA levels are negatively associated with the long-term survival of patients with duodenal cancer and may supplement traditional factors.
This study had some limitations. First, the study had a small sample size owing to the rare occurrence of duodenal adenocarcinoma. Therefore, performing sufficient analyses was difficult, and a large cohort was required to confirm the results. Second, we only included patients who underwent surgical treatment, and data on adjuvant chemotherapy and radiation therapy were unavailable. This may have resulted in selection and treatment bias. Third, the methods of sample collection and handling affect the quantity and characteristics of the cfDNA. Delays in the collection, separation, and extraction of cfDNA may have resulted in chemical damage or contamination. Furthermore, DNA hydrolysis, deamination, and oxidative damage can affect the accuracy of cfDNA analysis.18 The use of archived blood samples from biobanks was unavoidable as duodenal cancer is a rare entity that requires a long period for patient inclusion. Although sample collection and cfDNA assays in the control and duodenal cancer groups were performed carefully according to the same protocols, blood samples from patients with cancer and healthy individuals were collected and processed at different periods, which may have caused technical errors.
In conclusion, determination of cfDNA levels is a simple, noninvasive method for predicting survival outcomes in patients with duodenal adenocarcinoma. Our data demonstrated that cfDNA level is a strong independent prognostic factor for overall survival. This parameter should be integrated into clinical care to provide an accurate prognosis for patients with duodenal adenocarcinomas.
ACKNOWLEDGMENTSThis work was financially supported by grants from the Taipei Veterans General Hospital (V113C-188 and V113B-001), the Ministry of Science and Technology (NSTC 112-2314-B-075-016), and the Ministry of Health and Welfare (MOHW111-TDU-B-221-014015).
The authors would like to acknowledge the support of the Biobank of Taipei Veterans General Hospital, Common Well Foundation and statistical team of Taipei Veterans General Hospital.
REFERENCES 1. Bakaeen FG, Murr MM, Sarr MG, Thompson GB, Farnell MB, Nagorney DM, et al. What prognostic factors are important in duodenal adenocarcinoma? Arch Surg. 2000;135:635–41. 2. Buchbjerg T, Fristrup C, Mortensen MB. The incidence and prognosis of true duodenal carcinomas. Surg Oncol. 2015;24:110–6. 3. Poultsides GA, Huang LC, Cameron JL, Tuli R, Lan L, Hruban RH, et al. Duodenal adenocarcinoma: clinicopathologic analysis and implications for treatment. Ann Surg Oncol. 2012;19:1928–35. 4. Struck A, Howard T, Chiorean EG, Clarke JM, Riffenburgh R, Cardenes HR. Non-ampullary duodenal adenocarcinoma: factors important for relapse and survival. J Surg Oncol. 2009;100:144–8. 5. Ryder NM, Ko CY, Hines OJ, Gloor B, Reber HA. Primary duodenal adenocarcinoma: a 40-year experience. Arch Surg. 2000;135:1070–4. 6. Zenali M, Overman MJ, Rashid A, Broaddus RB, Wang H, Katz MH, et al. Clinicopathologic features and prognosis of duodenal adenocarcinoma and comparison with ampullary and pancreatic ductal adenocarcinoma. Hum Pathol. 2013;44:2792–8. 7. Sorenson GD, Pribish DM, Valone FH, Memoli VA, Bzik DJ, Yao SL. Soluble normal and mutated DNA sequences from single-copy genes in human blood. Cancer Epidemiol Biomarkers Prev. 1994;3:67–71. 8. Cheng J C, Holland-Letz T, Wallwiener M, Surowy H, Cuk K, Schott S, et al. Circulating free DNA integrity and concentration as independent prognostic markers in metastatic breast cancer. Breast Cancer Res Treat. 2018;169:69–82. 9. Yanagita M, Redig AJ, Paweletz CP, Dahlberg SE, O’Connell A, Feeney N, et al. A prospective evaluation of circulating tumor cells and cell-free DNA in EGFR-mutant non-small cell lung cancer patients treated with Erlotinib on a phase II trial. Clin Cancer Res. 2016;22:6010–20. 10. Ren N, Ye QH, Qin LX, Zhang BH, Liu YK, Tang ZY. Circulating DNA level is negatively associated with the long-term survival of hepatocellular carcinoma patients. World J Gastroenterol. 2006;12:3911–4. 11. Lapin M, Oltedal S, Tjensvoll K, Buhl T, Smaaland R, Garresori H, et al. Fragment size and level of cell-free DNA provide prognostic information in patients with advanced pancreatic cancer. J Transl Med. 2018;16:300. 12. Hamfjord J, Guren TK, Dajani O, Johansen JS, Glimelius B, Sorbye H, et al. Total circulating cell-free DNA as a prognostic biomarker in metastatic colorectal cancer before first-line oxaliplatin-based chemotherapy. Ann Oncol. 2019;30:1088–95. 13. Jiang QL, Huang XH, Chen YT, Zhang JW, Wang CF. Prognostic factors and clinical characteristics of patients with primary duodenal adenocarcinoma: a single-center experience from China. Biomed Res Int. 2016;2016:6491049. 14. Sohn TA, Lillemoe KD, Cameron JL, Pitt HA, Kaufman HS, Hruban RH, et al. Adenocarcinoma of the duodenum: factors influencing long-term survival. J Gastrointest Surg. 1998;2:79–87. 15. Rotman N, Pezet D, Fagniez PL, Cherqui D, Celicout B, Lointier P. Adenocarcinoma of the duodenum: factors influencing survival. French Association for Surgical Research. Br J Surg. 1994;81:83–5. 16. Bronkhorst AJ, Ungerer V, Holdenrieder S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol Detect Quantif. 2019;17:100087. 17. Tran TB, Qadan M, Dua MM, Norton JA, Poultsides GA, Visser BC. Prognostic relevance of lymph node ratio and total lymph node count for small bowel adenocarcinoma. Surgery. 2015;158:486–93. 18. Song P, Wu LR, Yan YH, Zhang JX, Chu T, Kwong LN, et al. Limitations and opportunities of technologies for the analysis of cell-free DNA in cancer diagnostics. Nat Biomed Eng. 2022;6:232–45.
留言 (0)