
記住我





Cases of accidently ingested foreign bodies are frequently encountered in clinical practice, but most foreign bodies pass through the gut uneventfully within 1 week.1 However, less than 1% of individuals with a history of ingesting foreign bodies experience consequences like gastrointestinal perforation or penetration. The development of a hepatic abscess secondary to a foreign body penetrating through the gastrointestinal tract is even more unusual.2 We report a case of liver abscess caused by an ingested foreign body that penetrated the gastric antrum. The abscess was successfully treated by surgical removal of the foreign body and broad-spectrum antibiotic coverage.
CASE REPORTA 47-year-old hypertensive man presented with complaints of intermittent episodes of high-grade fever associated with chills and rigors along with progressive, dull, aching right upper quadrant abdominal pain for 20 days. No history of alcohol use, nonsteroidal anti-inflammatory drug use, or prior surgery was reported.
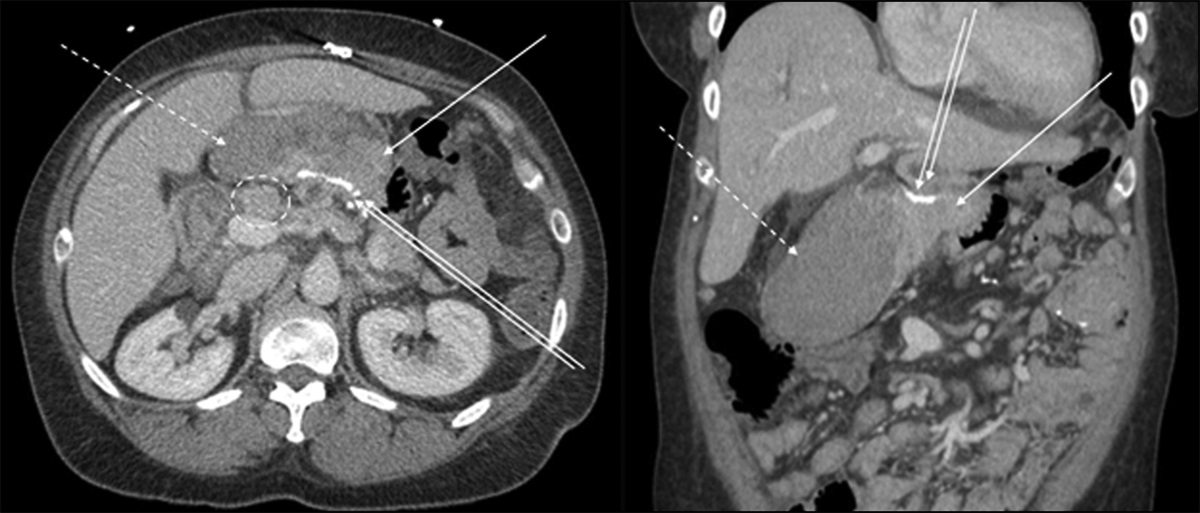
The patient denied any history of nausea, vomiting, loose stools, or jaundice. He was febrile (102°F) on examination, and tender hepatomegaly was present. Initial blood investigations revealed neutrophilic leukocytosis (44 × 10³/mm³), a mixed pattern of liver enzyme elevation, and mild urea and creatinine elevation. The blood culture was sterile (Table 1). Ultrasound of the abdomen was suggestive of a liver abscess measuring approximately 10 × 9 cm in the posterosuperior aspect of the right lobe of the liver. He was started on intravenous fluids and broad-spectrum antibiotics (injectable ceftriaxone 2 g intravenous once a day and injectable metronidazole 500 mg intravenous three times a day). The abscess was treated using ultrasound-guided pigtail drainage, and the pus sent for culture grew Staphylococcus capitis. According to the organism's sensitivity report, he was started on ertapenem. Persistent enzyme rise and fever spikes necessitated the search for a biliary etiology, for which contrast-enhanced imaging was used. An abdominal computed tomography was performed. It revealed a liver abscess measuring 7.4 × 12.0 × 9.4 cm involving segments 1, 4a, 4b, 5, 7, and 8 with pigtail drain in situ. Computed tomography (CT) also revealed a foreign body extruding from the pylorus of the stomach up to the caudate lobar capsule alongside the abscess and gallbladder calculus (Figures 1 and 2).
Table 1. - Presenting and follow-up liver function test Parameters Presenting liver function test Post-surgery follow-up liver function test (2 wk after surgery) Follow-up liver function test after 2 yr Total bilirubin (mg/dL) 0.9 0.8 0.5 Direct bilirubin (mg/dL) 0.5 0.4 0.2 Total protein (mg/dL) 7.6 7.4 7.6 Serum Albumin (mg/dL) 3.1 3.8 4.4 Alanine aminotransferase (U/L) 234 60 25 Alkaline phosphatase (U/L) 375 170 102 Figure 1.:
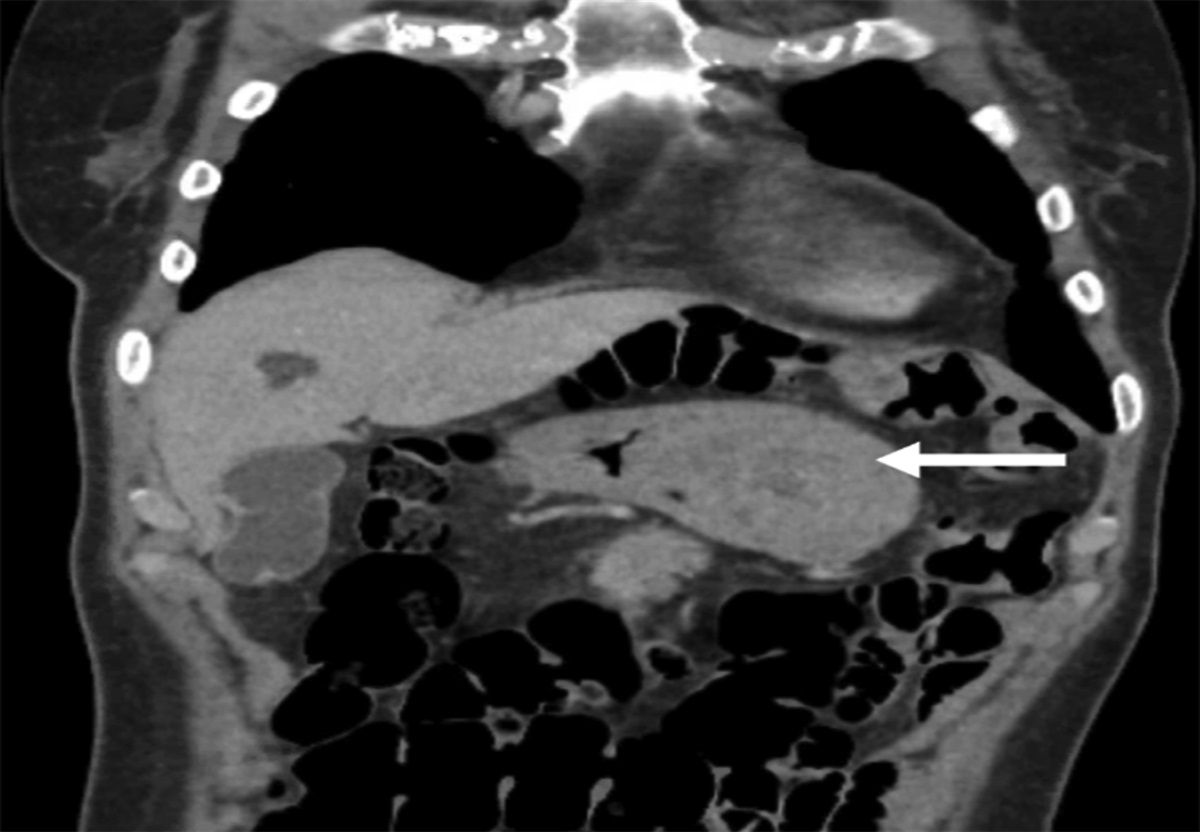
Figure 1.: Liver abscess demonstrated in contrast-enhanced computed tomography.
 Figure 2.:
Figure 2.: Hyperdense foreign body extruding from the pylorus of the stomach up to the caudate lobar capsule alongside the abscess.
The diagnosis of a liver abscess complicated by a foreign body was made. Although he could not recall any foreign body ingestion, esophagogastroduodenoscopy showed normal gastric mucosa devoid of a foreign body or fistula. There was no evidence of penetrating injury both on CT scan and in esophagogastroduodenoscopy.
The patient underwent surgical removal of the foreign body with drainage of the liver abscess (a 16 F Ryles Tube was placed in subhepatic space as a drain and fixed to the skin) (Figure 3). Interestingly, the foreign body was a fish bone (Figure 4). There was no perforation noted during surgery. After surgery, the recovery was uneventful, and the patient was discharged on a course of antibiotics. Complete resolution of the liver abscess was noted on follow-up ultrasound after 6 months.
 Figure 3.:
Figure 3.: Laparoscopic removal of the foreign body.
 Figure 4.:
Figure 4.: Surgical specimen of the foreign body retrieved (fish bone).
DISCUSSIONThe first case of hepatic abscess secondary to gastrointestinal tract perforation caused by a foreign body was reported by Lambert in 1898.3 In a review of literature conducted by Chong et al, of 88 patients identified through a PubMed search, 73% were male, 27% were female, and the mean age of the patients was 50.4 ± 18.6 years.4 Abdominal pain (77.3%) and fever (58%) were the most frequent symptoms, followed by vomiting (19.3%) and nausea (13.6%). Only 5% of the patients provided a positive history of ingesting a foreign body. Even in this case, the patient did not reveal a history of ingesting foreign bodies.
Fish bone (33%), toothpick (27.3%), chicken bone (12.5%), and needle (9.1%) were the reported cases of foreign body ingestion. There have also been reports of a clothespin, toothbrush, rosemary twig, pacemaker, rabbit bone, pen, lobster shell, metal wire, and dental plate.4
In the cases reviewed, the stomach was the most common site of perforation (40.9%), followed by the duodenum (20.5%) and colon (11.4%).4 Regarding the hepatic abscess location, it usually affects the left lobe of the liver (65.9%), then the right lobe (29.5%), and bilobar involvement was seen in 4.5% of cases. The liver abscesses ranged in size from 2 to 16 cm, with a mean of 6.82 ± 3.09 cm. Contrary to cryptogenic hepatic abscesses, which frequently affect the right liver lobe, liver abscesses caused by foreign body penetration primarily involve the left lobe of the liver.
In addition, when a lesion is encountered with no discernible underlying condition and treatment fails, liver abscess secondary to foreign body penetration of the gastrointestinal tract should be ruled out.4
In most of the patients, CT was used to establish the diagnosis. In the remainder of the cases, ultrasound, radiographs, and laparotomy were used. CT is more helpful than other modalities because it can identify the site of penetration of the foreign body along with the complications. In about 14% of the cases reported, the diagnosis was established only by laparotomy. In the early stages, when the foreign body has not completely migrated, endoscopy might be helpful.4
In the present patient, CT was diagnostic because it helped to localize the gastric antrum as the site of penetration and also identified complications in the form of liver abscess. The endoscopy although did not reveal any mucosal lesion as the mucosa might have healed.
A single bacterial strain can be identified in about half of the cases; 2 bacterial flora and multiflora can be identified in 18% and 12% of the cases, respectively. Negative culture results can be noted in about 14.5% of the cases. Streptococcus species (72.3%), followed by Escherichia coli (17%) and Klebsiella pneumoniae (10.6%) were the organisms identified in the reported cases.4
The recommended treatment of liver abscess caused by penetrating a foreign body comprises removal of the foreign body and drainage of the hepatic abscess. In the cases reported, surgical removal by laparotomy or laparoscopy was the most commonly performed procedure. Other procedures included endoscopic or percutaneous interventional radiological approaches.4 In this case, laparoscopic removal of the foreign body and drainage of the liver abscess were curative.
DISCLOSURESAuthor contributions: All authors contributed equally to this manuscript. P. Bhayani is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. McCanse DE, Kurchin A, Hinshaw JR. Gastrointestinal foreign bodies. Am J Surg. 1981;142(3):335–7. 2. Santos SA, Alberto SC, Cruz E, et al. Hepatic abscess induced by foreign body: Case report and literature review. World J Gastroenterol. 2007;13(9):1466–70. 3. Bekki T, Fujikuni N, Tanabe K, Amano H, Noriyuki T, Nakahara M. Liver abscess caused by fish bone perforation of stomach wall treated by laparoscopic surgery: A case report. Surg Case Rep. 2019;5(1):79. 4. Chong LW, Sun CK, Wu CC, Sun CK. Successful treatment of liver abscess secondary to foreign body penetration of the alimentary tract: A case report and literature review. World J Gastroenterol. 2014;20(13):3703–11.
留言 (0)