
記住我



A 57-year-old man presented to the emergency department with unilateral right eye blurred vision for three days, which predominantly affected his inferior hemifield. This was preceded by one week of progressive right periorbital erythema and oedema. He had a history of hypermetropia and no other past ophthalmic history.
His medical history included multiple myeloma diagnosed 13 years prior and in remission at the time of presentation. As part of his treatment for multiple myeloma, he received allograft stem cell transplantation. He developed interstitial lung disease secondary to severe graft-versus-host disease which resulted in bilateral sequential lung transplantation three months prior to presentation.
On routine bronchoscopy two weeks post lung transplant, a bronchoalveolar lavage (BAL) specimen cultured 1+ Lomentospora prolificans. The patient commenced voriconazole 200mg twice daily, terbinafine 250mg twice daily and his tacrolimus dose was reduced. Two subsequent BAL specimens six- and eight-weeks post-transplant demonstrated no growth. However, he then developed mild neutropenia and acute on chronic renal failure, with a creatinine clearance of 52mL/minute. As a result of his poor renal function, prophylactic valganciclovir was dose-reduced and trimethoprim/sulfamethoxazole was ceased.
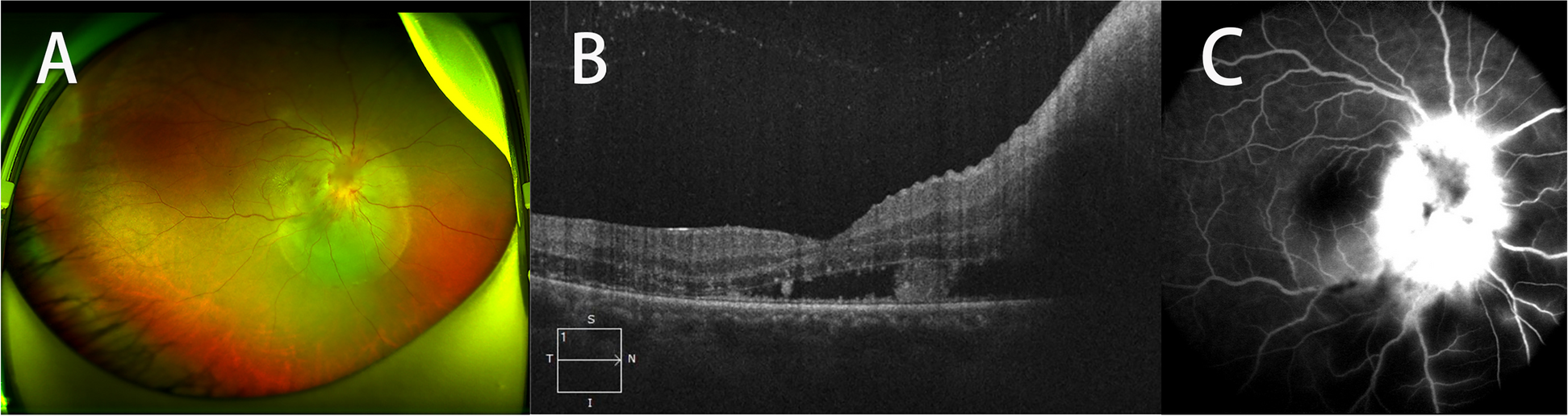
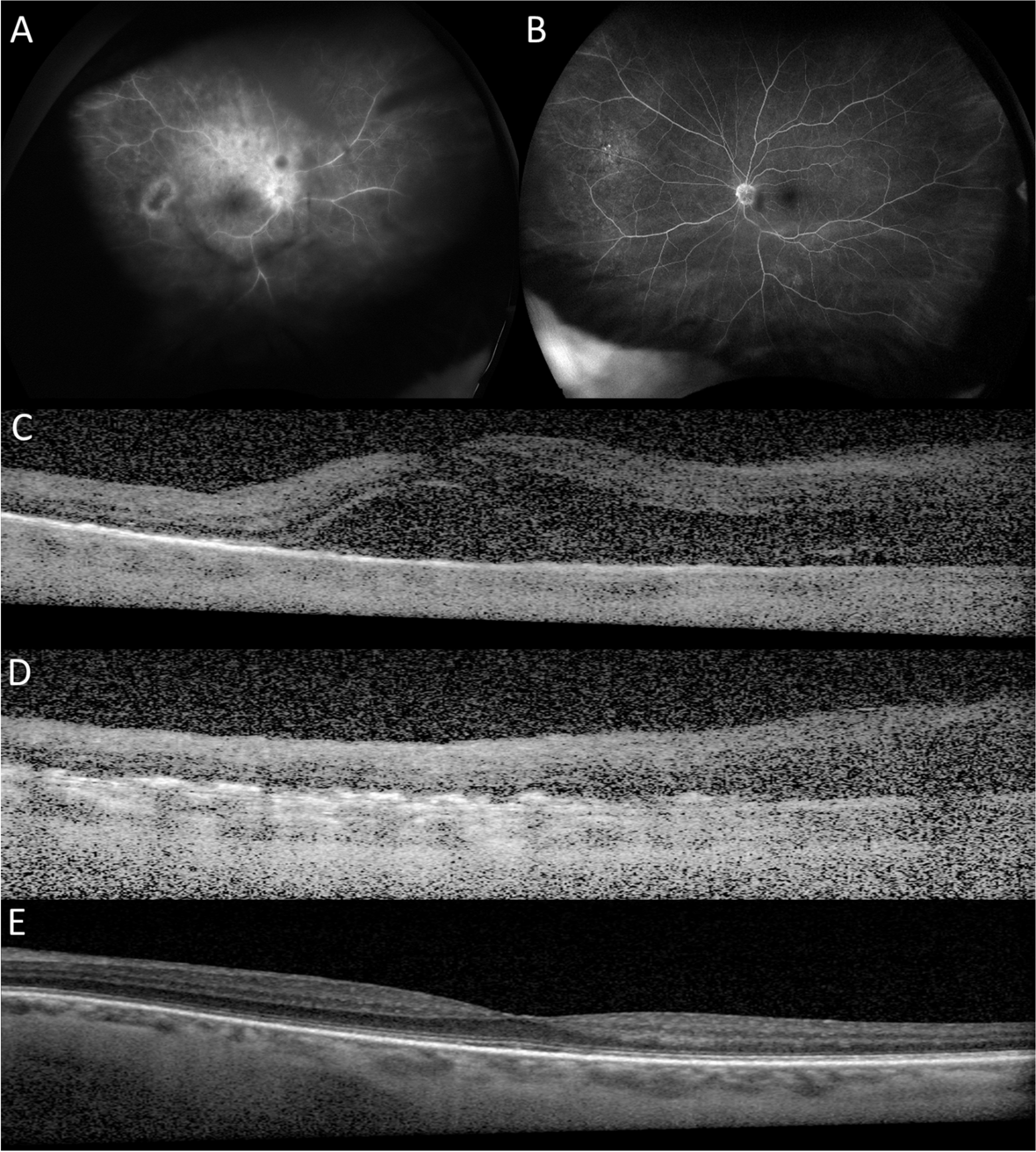
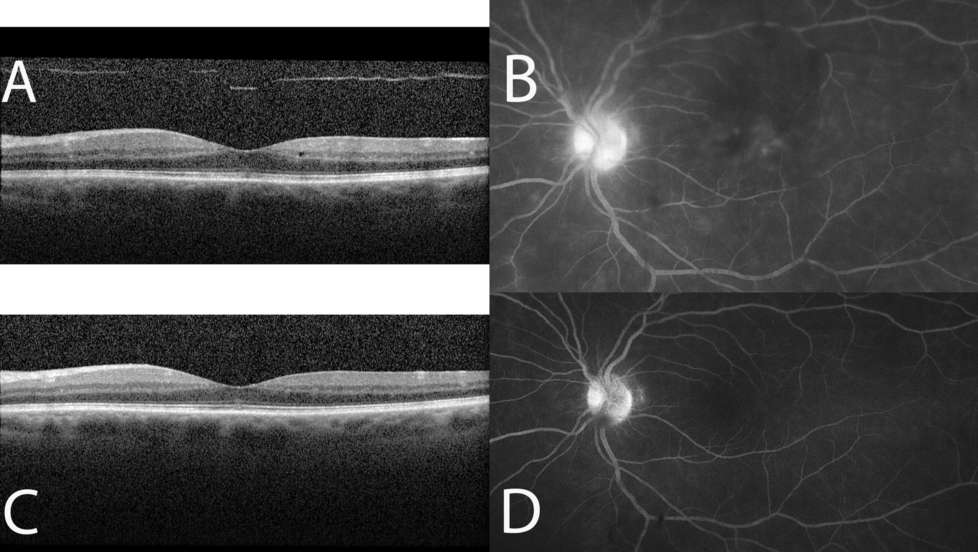
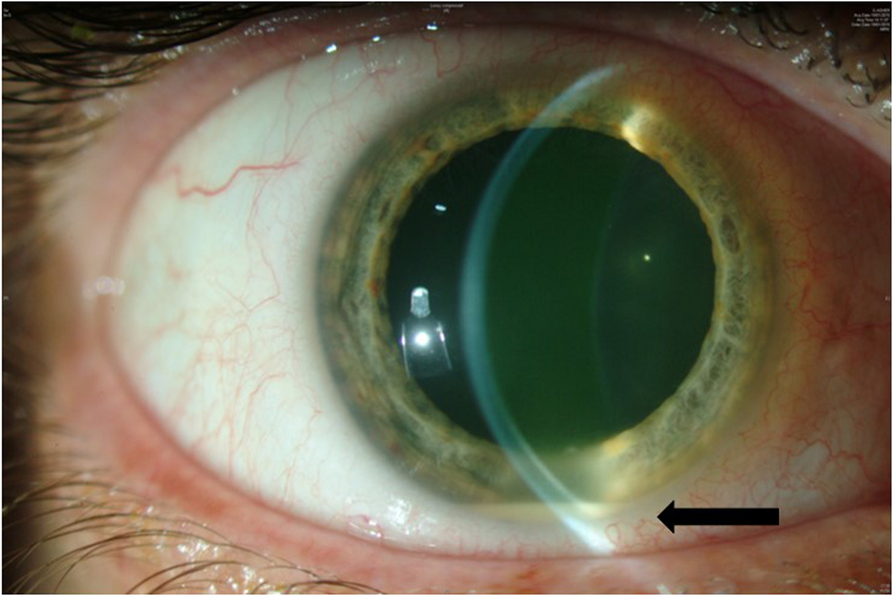
At presentation, right visual acuity was 6/24. However, this rapidly deteriorated to counting fingers within 24 hours. Left visual acuity was 6/6. Intraocular pressures were 8mmHg bilaterally. There was inferior chemosis and inferior conjunctival injection in the right eye with a clear cornea. There was 2+ anterior chamber cells in the right eye and 1+ anterior vitreous. Fundus examination revealed moderate vitreous haze with a large area of elevated retinitis encompassing the superior macula surrounded by patchy occlusive retinal vasculitis and retinal haemorrhages. The left eye was unremarkable.
An urgent anterior chamber and vitreous aspiration was performed for microscopy and culture. The vitreous was injected with ceftazidime, vancomycin, foscarnet and voriconazole prior to both vitreous and aqueous specimens culturing 1+ Lomentospora. Antifungal sensitivities were performed which demonstrated resistance to Amphotericin B, however sensitivities to 5-Flurocytosin, anidulafungun, posaconazole and voriconazole were not able to be interpreted due a lack of established clinical breakpoints in minimum inhibitory concentration. Other blood work up demonstrated a haemoglobin of 90g/L (reference range 128–175), lymphocyte count of 0.13x109/L (reference range 0.90–3.30) and neutrophil count of 1.06x109/L (reference range 1.90–8.00).
Systemically, the oral voriconazole dose was increased to 250mg twice a day and micafungin was commenced at 300mg loading followed by 150mg daily in addition to terbinafine 250mg twice daily.
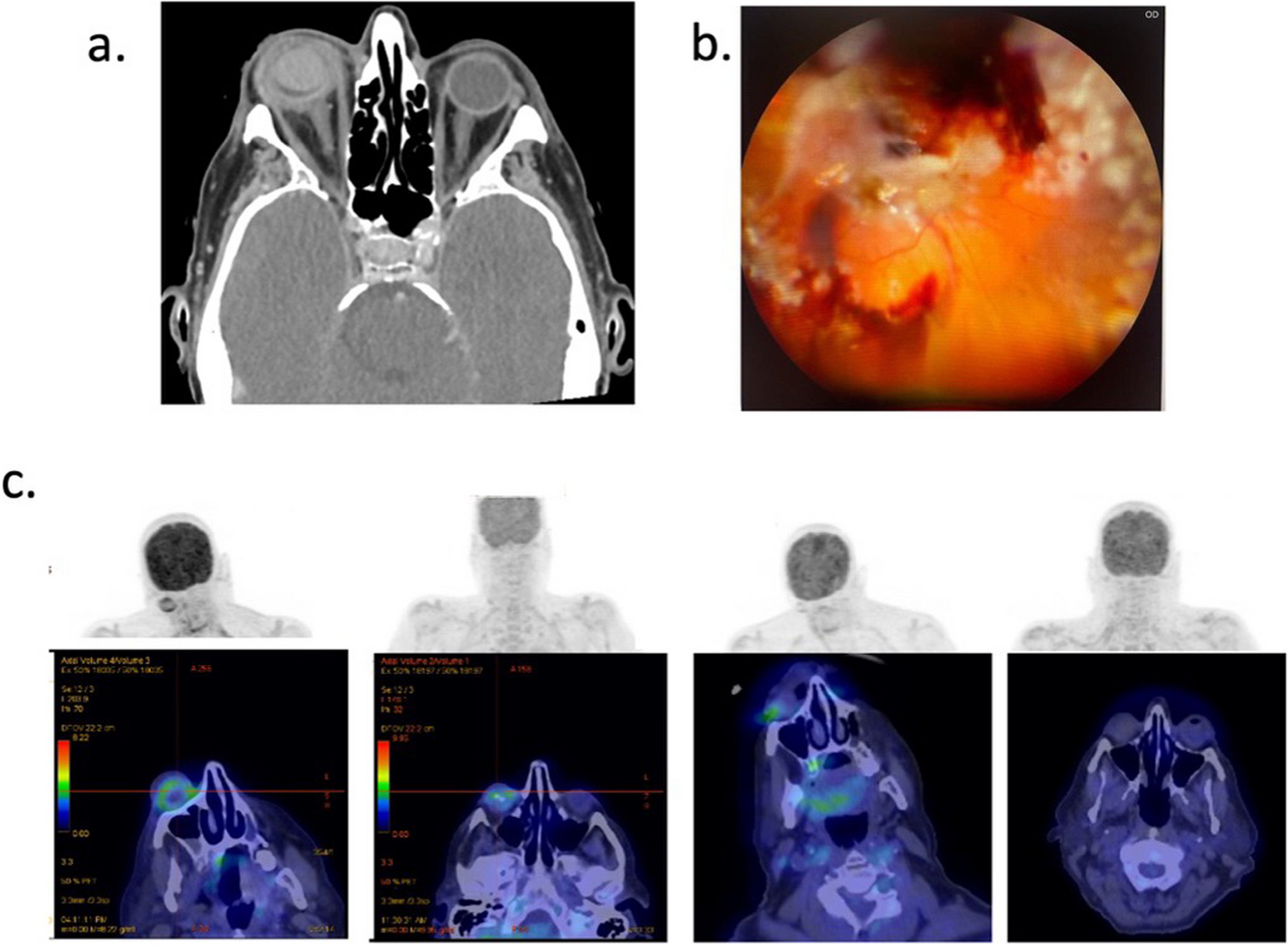
Right combined pars plana vitrectomy, lensectomy with insertion of silicone oil and intravitreous injection of voriconazole (100µg/0.1mL) and caspofungin (100 µg/0.1mL) was performed three days later. Intraoperative findings noted a large temporal retinal detachment and a superior subretinal abscess extending into the macula (Fig. 1b).
Fig. 1
a Coronal computerised tomography scan of the orbit demonstrating circumferential thickening and enhancement around the entire right globe, vitreous haemorrhage, proptosis and retro-orbital intraconal inflammatory stranding. Normal CT appearance of the left globe. B Intraoperative right fundus photo of the right eye demonstrating large temporal retinal detachment, vitreous haemorrhage, superior area of retinitis and subretinal abscess extending inside superior arcade into macula. C Serial Fludeoxyglucose (FDG) positron emission tomography (PET) scans demonstrating FDG uptake and inflammatory changes in the right globe and subsequent interval improvement in right globe avidity. Images were obtained at approximately 1 month intervals from initial presentation
The patient was commenced on a loading dose of Olorofim (150mg daily) and 90mg twice daily ongoing. All other systemic antifungal therapy (voriconazole, terbinafine, micafungin) was ceased due to concern for potential drug antagonism.
However, he subsequently developed painful right ophthalmoplegia, proptosis and haemorrhagic chemosis with severe raised intraocular pressure (IOP) of 50mmHg. A positron emission tomography (PET) scan revealed disseminated disease with uptake in the right eye and the aortic valve, suggestive of fungal endocarditis. Oral voriconazole and terbinafine was recommenced in conjunction to Olorofim. Granulocyte colony stimulating factor (G-CSF) was administered for ongoing neutropenia.
The patient’s symptoms and ocular signs significantly improved whilst on triple antifungal therapy with two further doses of intravitreal voriconazole (100µg/0.1mL) one week apart. He was discharged home after a total of six-weeks as an inpatient during which he received a total of six intravitreal voriconazole injections. Oral voriconazole and terbinafine were ceased five days after discharge however the patient remained on Olorofim 90mg twice daily.
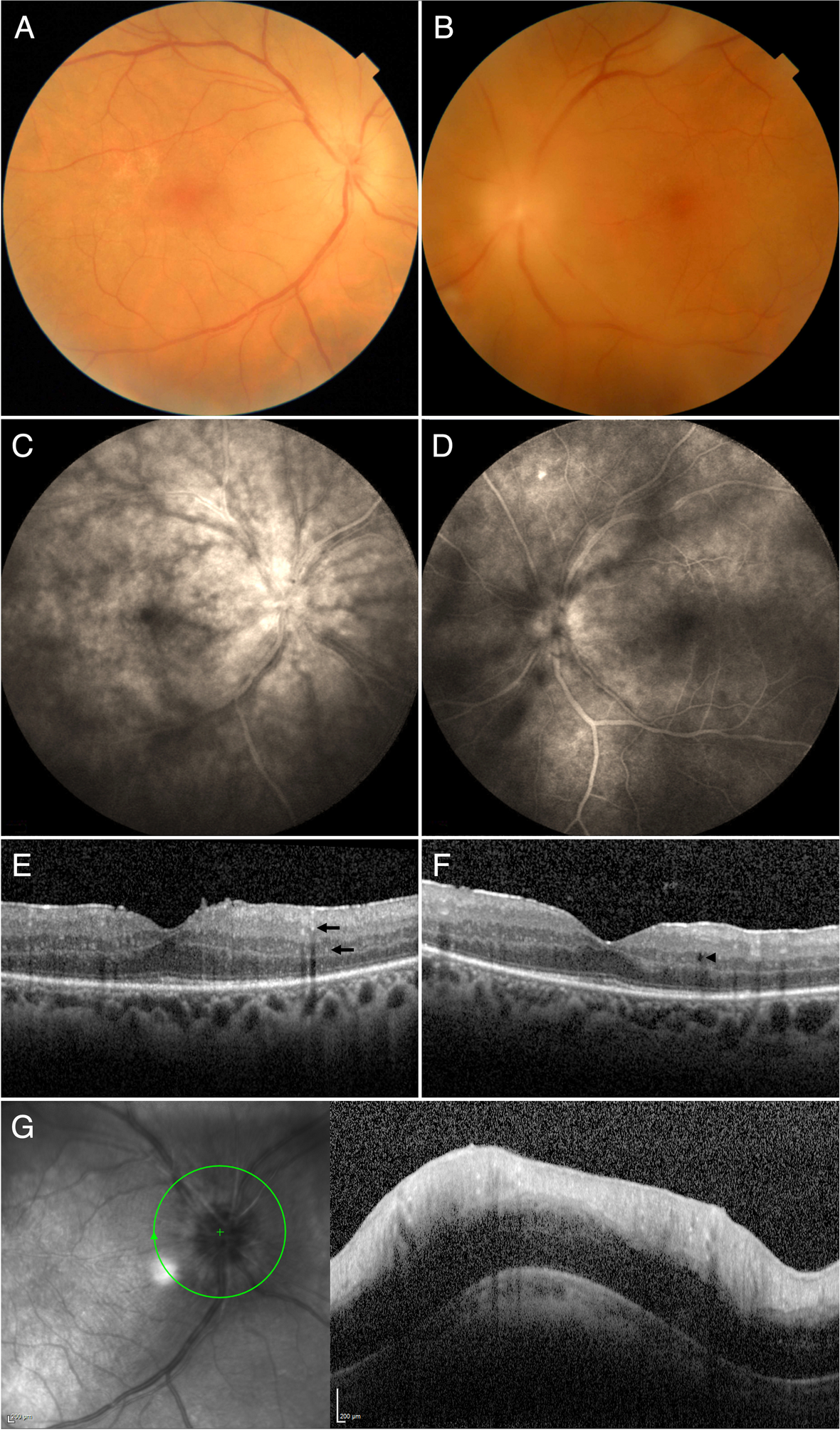
Two months post discharge, the patient was readmitted with whole body myalgias, blurred left vision, photophobia, and new left eye floaters. Left visual acuity was 6/12 which rapidly deteriorated to hand movements within 48 hours. IOP was 9mmHg. There was 2-3+ anterior chamber cells and nearly 360-degree posterior synechiae with a hazy view to the posterior segment. Both left vitreous aspiration and blood cultures grew Lomentospora prolificans. Intravitreal voriconazole was administered in conjunction with systemic voriconazole, terbinafine and Olorofim. The patient underwent urgent left eye pars plana vitrectomy which revealed two areas of retinitis inferiorly with a pale optic disc.
Despite intravitreal voriconazole (100µg/0.1mL), caspofungin (100µg/0.1mL) and amphotericin B (10μg/0.1mL) and systemic triple therapy, the patient died fourteen days later from severe aortic valve and femoral artery involvement of disseminated Lomentospora.
留言 (0)