In our study, we found that POAG filtering surgery, male sex and the COVID-19 pandemic period might be potential interrelated factors for BAE. Streptococcus species were the leading pathogenic organisms isolated in the current research.
IOP is one of the most important risk factors for glaucoma [13, 14], and glaucoma filtration surgery is an effective approach to decreasing it [2]. The presence of a filtering bleb after the surgery may result in bleb-associated endophthalmitis, which is rare and could be a devasting complication [8, 15, 16].
From the patient demographic investigation in our study, we found that the proportion of BAE was approximately 0.3%, which is close to other reported studies [9, 11, 17,18,19,20], varying from 0.2% to 3.8%. Also, we found most of them were male patients (71.4%, p = 0.023), which was consistent with the reports that male sex might be a potential correlative factor for BAE [21, 22].
Consistent with our previous study on BAE duration from 2003–2010 [8], POAG in the current study (39.3%, p ≤ 0.001) was the most common glaucoma related to BAE. Although a national cross-sectional study has shown that PACG accounts for the largest proportion in China [23], POAG has been considered a relative factor in bleb-related infections [6, 8]. The reasons can be considered from two perspectives. On the one hand, patients with POAG are younger and more prone to scarring than those with PACG, leading to longer use of the subconjunctival infiltration of antimetabolites to achieve a lower IOP, potentially predisposing to bleb-related infection [6, 22]. On the other hand, the surgical options for PACG have changed in recent years, and an increasing number of doctors are inclined to select cataract extraction combined with goniosynechialysis instead of traditional glaucoma filtration surgery [10].
Gathering statistics on antimetabolite usage was challenging in this study, as most patients had previously undergone glaucoma filtration surgery in other primary hospitals, except for nine patients who had previously undergone glaucoma surgery in our hospital and who received MMC adjunctive infiltration. Previous research has confirmed that antimetabolites are a risk factor for BAE and can induce thinner and more avascular filtering blebs. Thin-walled and avascular blebs were considered more inclined to become infected than thicker blebs [5, 20, 22, 24]. Patients with BAE visited our clinic with bleb infection and pus in the bleb, as well as thin and avascular blebs, suggesting that the bleb condition might be one of the related factors involved in the pathogenesis of BAE. In addition, bleb leaks detected in 9 patients (32.2%) in our current study and in other studies were also regarded as potential related factors for BAE. Bleb leaks might lead to hypotony and a vulnerable ocular surface, which is the barrier preventing invasion from bacteria and contributes to blebitis or endophthalmitis [9, 19].
All the cases in our study had late endophthalmitis, with an average time of approximately 9.8 years from glaucoma filtration surgery, longer than in some studies [9, 25]. In accordance with other studies, most of the patients visited the hospital with complaints of redness, reduction of vision, and ocular pain [8, 9, 24]. As most patients had endophthalmitis many years after the glaucoma filtration process, they should be advised by ophthalmologists about the significance of redness, blurred vision, and ocular pain as symptoms, and encouraged to promptly seek medical attention.
Visual acuity was one of the most important assessment criteria for ocular disease severity and treatment outcomes. In our study, only one patient had a VA better than 20/400 at the onset of BAE. Consistent with other reports, most patients diagnosed with BEA had poor initial visual acuity before treatment [8, 9, 24, 26], which might result from corneal edema and an inflammatory response in the vitreous humor. Fortunately, the visual acuity was significantly improved after treatment (p≤0.001), which reminded us of the importance of timely treatment in rescuing the vision of patients with BAE.
The abnormal intraocular pressure at the onset of BAE observed in the present study is noteworthy. Seven (25.0%) eyes showed a low tension of < 10 mmHg), and one patient presented with hypotony < 6 mmHg, which might be related to poor bleb conditions like bleb leak and impaired ocular surface. The fragile surface surroundings provided a path for the invasion of pathogenic microorganisms, resulting in blebitis or endophthalmitis [9, 19]. Meanwhile, we noticed that five patients (17.9%) exhibited abnormally high IOP > 30 mmHg, with the highest IOP value being 60 mmHg. Quite a few studies account for this phenomenon. Sacc`a et al. indicated that inflammation in the anterior segment might elevate aqueous outflow resistance, promote trabecular meshwork dysfunction, and increase IOP in POAG [27]. In our study, we hypothesized that the inflammatory response in the anterior chamber and vitreous cavity may result in filtration outflow channel obstruction or dysfunction and contribute to ocular hypertension at the onset of BAE.
In our study, all patients received PPV combined with the tap-and-inject procedure, most patients (85.7%, < 0.001) underwent single PPV. However, some underwent PPV or tap-and-inject more than once for inflammatory inhibition. Some studies have shown that PPV for BAE results in improved visual outcomes [26, 28,29,30]. However, Islam et al. confirmed that visual acuity and IOP control were similar after initial PPV compared with taps and injections when managing BAE [31]. Leng et al. found that patients with BAE had better visual acuity via tap and injection than patients with PPV [18].
During surgery, specimens were acquired from the aqueous and vitreous chambers to detect the causative infectious agents. Streptococcus spp. were the most common pathogenic organisms found in our study (46.4%, p ≤ 0.001). Similar findings have been reported in some research [9, 11, 25, 26, 29]. Our previous study and some researchers noted that Staphylococcus species were more commonly observed [8, 32]. Although microbiological cultivation was affected by technical means, the microbial spectrums for BAE have not changed much over the years, and gram-positive bacteria are still the most frequent organisms.
At the final follow-up, the visual acuity was significantly increased after treatment (p ≤ 0.001), and the cases presented with VA of 20/400 or better were raised from 3.6% to 28.6% after reasonable treatment. This indicates that timely treatment may improve visual acuity in some patients. However, patients with NLP raised from 3 to 5 cases at the final follow-up, and even ended up with enucleation because of eyeball atrophy or absolute glaucoma. Busbee and Jacobs et al. confirmed that culture-positive cases were related to worse VA outcomes than culture-negative cases [26, 33]. In accordance with previous research, both eyes in our study that ended with enucleation were culture-positive, indicating that organisms affected visual outcomes. Most of the cases (78.6%) in our study acquired a stable IOP after surgery at the final follow-up. However, four patients accepted further glaucoma surgeries and had stable IOP at the final follow-up. Another BAE patient, who accepted cyclophotocoagulation in 2022, still had ocular hypertension at the final follow-up. The proportion of stable IOP control was higher than that of Mady et al., who found that 25% of patients with BAE could maintain stable IOP control after treatment [34].
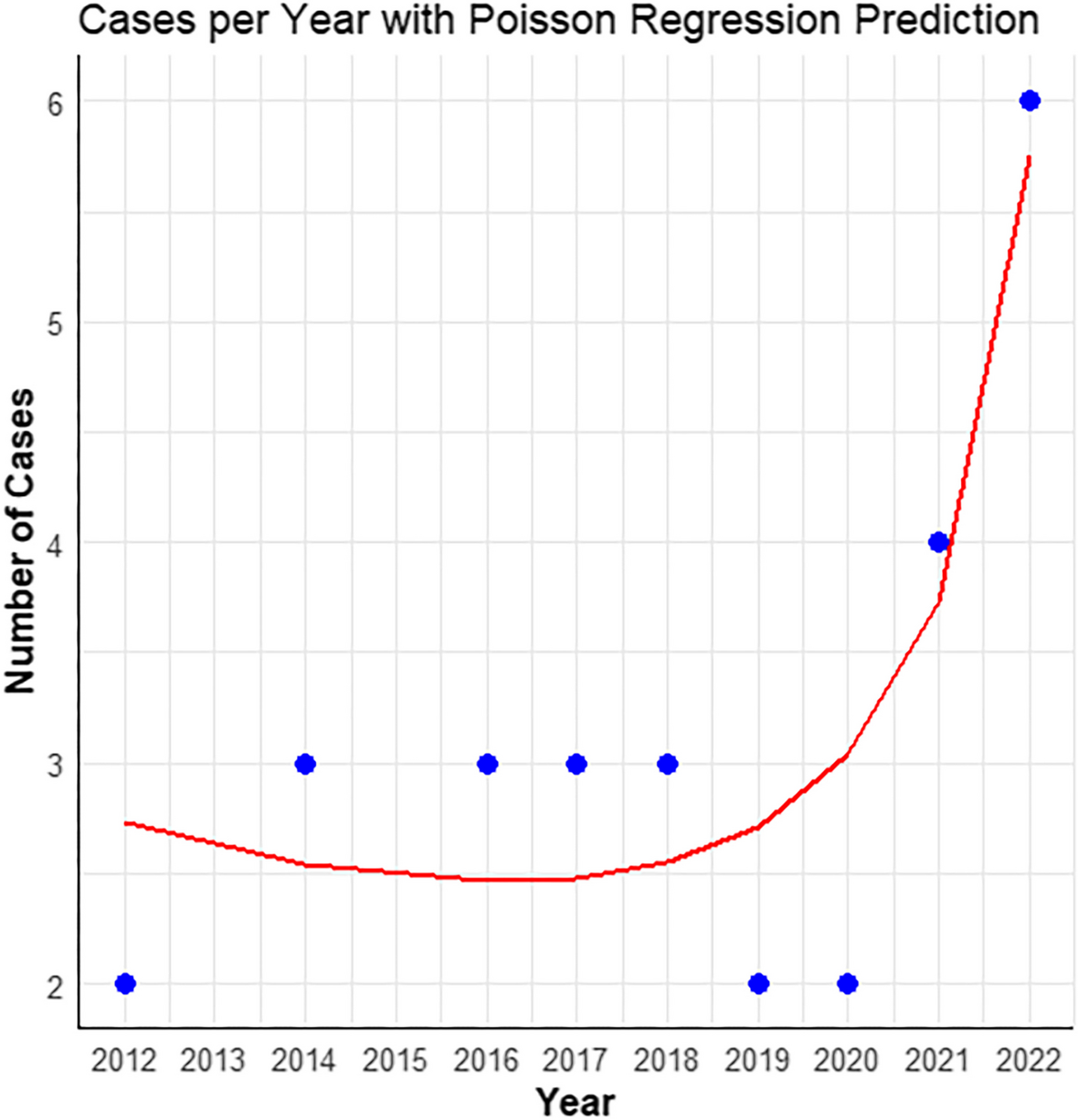
The COVID-19 pandemic has made it difficult for people to receive medical services throughout China. In this study, we compared the clinical processes between the COVID-19 pandemic and previous years. The cases of BAE occurring annually during the COVID-19 pandemic period (4 cases per year on average) were twice as many as in the previous years (2 cases per year on average). Poisson regression model analysis showed a significant upward trend during the COVID-19 pandemic period from 2020–2022, compared to previous years, which indicated the COVID-19 pandemic might be a potential related factor for increased incidence rate of BAE. We noticed that, with non-statistical meaning, the proportion of patients with VA 20/400 or better at the final follow-up was seemingly higher during the COVID-19 pandemic period. Several hypotheses can explain this phenomenon. On the one hand, researchers put forward the idea that a digital revolution was needed to face the COVID-19 pandemic [35], and ophthalmologists have been striving to provide medical care most effectively via telemedicine during the COVID-19 pandemic [36]. Consistent with other reports, doctors in our hospital struggled to provide reliable and timely advice via online outpatient services. However, patients might pay sufficient attention to their self-health status and eye discomfort during the COVID-19 pandemic and visit doctors promptly.
As this was a descriptive report with only 28 cases with BAE included from 2012–2022, our data analysis and hypothesis were restricted by the number of cases in the current study. Further research on BAE is required in our future studies, and the time range of the data search should be expanded to make our results more significant.





留言 (0)