
記住我



A 72-year-old female patient was referred to our ophthalmology clinic for evaluation of retinitis and vasculitis in the right eye (OD).
The patient initially developed blurred vision OD one month prior to presenting to an outside ophthalmology clinic. She was diagnosed with anterior uveitis OD, and topical prednisolone acetate was subsequently initiated. However, her vision continued to deteriorate, and retinal whitening was noted three weeks later. Uveitis work-up, including Treponema pallidum IgG, antinuclear antibodies (ANA), and Toxoplasmosis serology, was all negative, and the patient was promptly referred to our ophthalmology clinic for further evaluation.
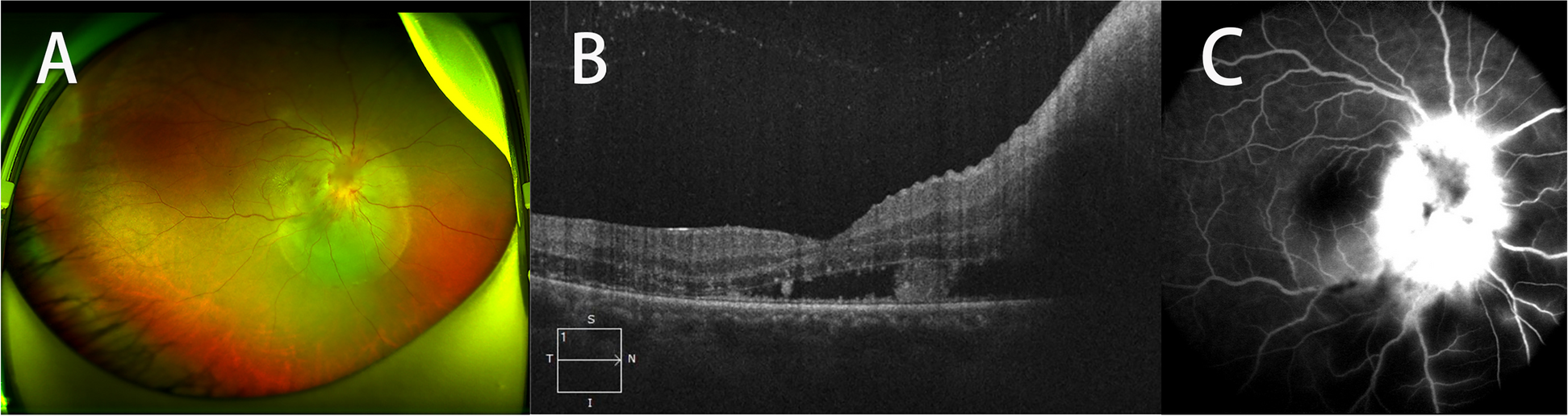
Detailed past medical history revealed hypertension, hyperlipidemia, hearing loss, chronic cystitis, and diffuse large B cell lymphoma (DLBCL) with cutaneous involvement. She had previously received chemotherapy from February to July 2021 for her DLBCL and had been in remission since. On examination, best-corrected visual acuities (BCVAs) were hand motions OD and 20/20 in the left eye (OS). Slit-lamp examination revealed diffuse fine keratic precipitates, 1 + anterior chamber cells, and 3 + vitreous cells OD. Fundus examination of the right eye was limited due to the vitreous opacities, but optic disc edema and diffuse retinal whitening superior to the superotemporal arcade were noted. Fluorescein angiography of the right eye revealed diffuse retinal vascular leakage and hyperfluorescent staining of the corresponding retinal whitening (Fig. 1A). Optical coherence tomography (OCT) demonstrated intraretinal fluid and subretinal fluid along with the optic disc edema OD (Fig. 1C). The B-scan through the retinal whitening area demonstrated significant retinal thickening with subretinal deposits (Fig. 1D). Fluorescein angiography of the left eye demonstrated mild hyperfluorescent staining in the periphery, and OCT of the left eye was normal (Fig. 1B, E). Given the high suspicion of infectious retinitis, the patient was treated with intravitreal foscarnet, valacyclovir, and oral prednisone and underwent a comprehensive uveitis workup. Magnetic resonance imaging of the brain and orbits demonstrated microvascular changes, and echocardiogram and carotid ultrasound were unremarkable. Furthermore, the patient underwent a lumbar puncture with cerebrospinal fluid analysis, which was suspicious for a B-cell lymphoproliferative disorder.
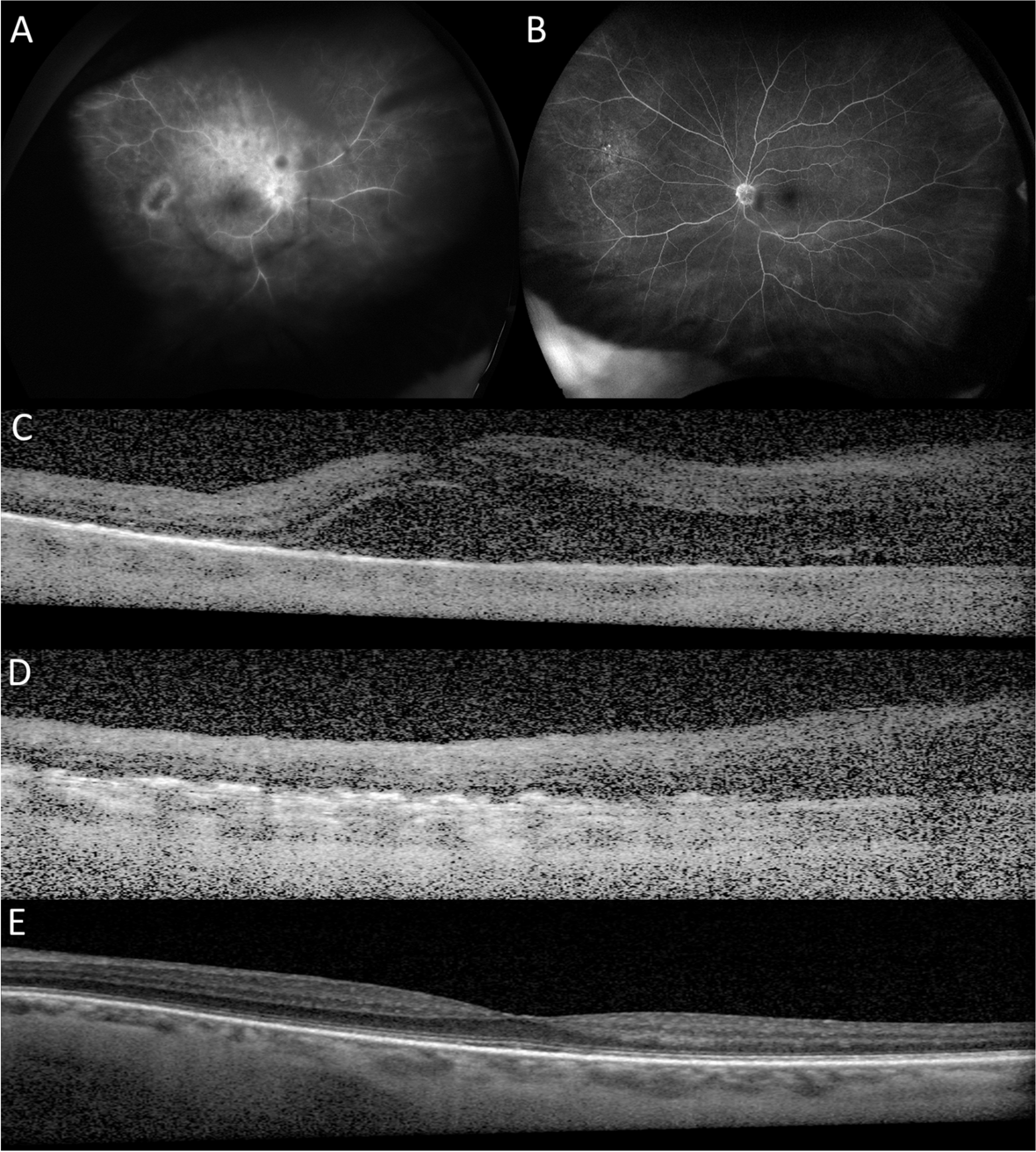
Fig. 1
Fluorescein angiography revealed diffuse retinal vascular leakage and hyperfluorescent staining of the corresponding retinal whitening OD (A). Optical coherence tomography demonstrated intraretinal fluid and subretinal fluid along with the optic disc edema OD (C). The B-scan through the retinal whitening area demonstrated significant retinal thickening with subretinal deposits OD (D). Fluorescein angiography of the left eye demonstrated mild hyperfluorescent staining in the periphery, and OCT of the left eye was normal (Fig. 1B, E)
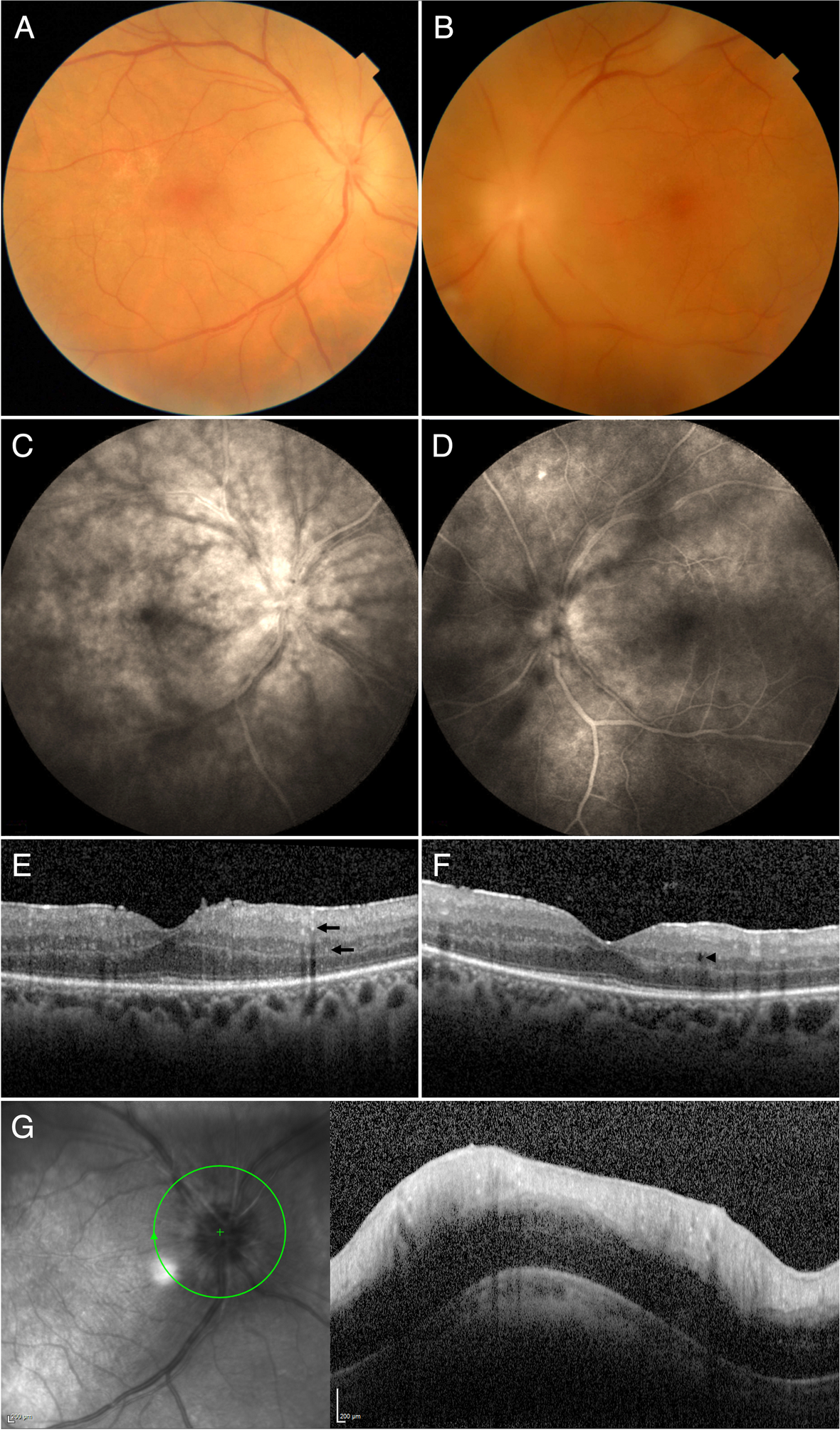
The patient returned for a follow-up one week later, and her vision remained unchanged. Uveitis work-up was unremarkable including antineutrophilic cytoplasmic antibody (ANCA), antinuclear antibody (ANA), anti-cyclic citrullinated peptide (anti-CCP), rheumatoid factor (RF), Quantiferon-TB, serum Toxoplasmosis IgG and IgM, Treponema pallidum antibody, Bartonella henselae antibody, angiotensin-converting enzyme (ACE), and Lysozyme. Anterior chamber paracentesis was negative for varicella zoster virus (VZV), cytomegalovirus (CMV), herpes simplex virus (HSV)-1 and HSV-2. On examination, BCVAs were hand motion OD and 20/20 OS. Slit-lamp examination revealed diffuse fine keratic precipitates, trace AC cells, and 2 + vitreous cells OD. Fundus examination of the right eye revealed optic disc edema, whitening around the peripapillary region, and diffuse whitening superior to the superotemporal arcade (Fig. 2A). Examination of the left eye demonstrated mild vitritis along with some infiltrates in the periphery (Fig. 2B). Given the negative PCR testing and history of B-cell lymphoma, vitreoretinal lymphoma was suspected, and the patient was scheduled to undergo vitrectomy with vitreous and retinal biopsy.
Fig. 2
Ultrawide-field color fundus photo of the right eye revealed severe vitritis, optic disc edema with the blurring of margins, whitening around the peripapillary region, and diffuse whitening superior to the superotemporal arcade (A). Ultrawide-field color fundus photo of the left eye demonstrated mild vitritis along with some infiltrates in the periphery (B)
A 25-gauge pars plana vitrectomy was performed to obtain a vitreous specimen. The specimen was sent for cytopathologic analysis, flow cytometry, and culture. Following a complete vitrectomy, the retina was visualized, and a zone of retinal whitening was noted. Given the high suspicion for a neoplastic process, decision was made to proceed with a retinal biopsy at the border of abnormal and more normal-appearing retina. Internal cautery was used to demarcate the boundaries of the retinal biopsy. Subsequently, a Finesse loop (Alcon, Ft. Worth, Texas) and intraocular forceps were used to dissect the retina and the underlying pigment epithelium from the choroid. A broad chorioretinal adhesion at the site of the biopsy was noted. The specimen was removed from the eye via a pars plana sclerotomy and was sent for cytopathologic analysis. The donor site was surrounded by three rows of endolaser retinopexy. Fluid-air exchange and 12% perfluoropropane (C3F8) gas exchange were performed (Video, Supplemental Material).
The flow cytometric analysis identified a population of mature large B-cells (77% of isolated cells) with increased side light scatter expressing HLA-DR, CD19, CD38 and moderate-density kappa light chains. Cytology of vitreous fluid demonstrated atypical lymphoid cells with a high nuclear/cytoplasmic ratio, irregular nuclear membranes and multiple nucleoli (Fig. 3A, B). The large lymphoid cells were positive for CD20 (Fig. 3C), while CD3-stained cells were small, reactive T-cells (Fig. 3D). In the retinal biopsy, there was near complete effacement of retinal architecture by large, atypical CD20 + lymphocytes (Fig. 4A, B). Cells of interest were kappa restricted by flow cytometry (Kappa + : 91.55%), and CD10-negative, 60% BCL6 + and > 80% MUM1 + by IHC indicative of a non-germinal center (activated B-cell) phenotype (Fig. 4E, F, G) [13]. Consistent with this diagnosis, Ki67 staining was markedly elevated at 60% positive cells, and the Ki67 proliferative index was 80% (Fig. 4H). The findings were consistent with diffuse large B-cell lymphoma. The patient was diagnosed with vitreoretinal lymphoma and treated with 6 intravenous infusions of high-dose methotrexate (3 g/m2) and 6 intravenous infusions of rituximab (375 mg/m2) every two weeks. At 5-month follow-up, BCVAs were hand motions OD and 20/30 OS, and slit-lamp examination revealed resolved keratic precipitates, and trace AC cells OD. Fundus examination demonstrated disc edema with blurry margins and resolved retinal whitening OD (Fig. 5A). OCT of the right eye revealed loss of outer retinal tissue and resolution of macular edema (Fig. 5C). Examination of the left eye remained unchanged (Fig. 5B, D). She responded well to the treatment with regression of vitreoretinal lymphoma on examination, and she was monitored closely for lymphoma recurrence. Unfortunately, she developed recurrence 5 months later, which subsequently prompted intravitreal methotrexate (400 mcg/0.1 mL) monthly for 3 months and oral maintenance chemotherapy with ibrutinib.
Fig. 3
The cytospin preparation showed large, atypical lymphocytes (red arrows) with high nuclear/cytoplasmic ratio and irregular nuclear membranes. A few small benign lymphocytes are present (black arrow) in Diff Quick and Papanicolaou stains (A, B). Immunocytochemistry for CD20 and CD3 showed robust staining of atypical cells with CD20 (C) while small background lymphocytes were reactive with CD3 (D)
Fig. 4
Histologic examination of retinal biopsies demonstrated near complete effacement of retinal architecture by large, atypical lymphocytes (A, B). These atypical cells were CD20-positive (C) while CD3-stained cells were reactive with small, background T-lymphocytes (D). The atypical cells were CD10-negative (E), 60%-70% of cells stain for BCL6 (F) and greater than 80% of cells were reactive with MUM1 (3G). Ki67-stained cells were markedly elevated (H). (BCL-6: B-cell lymphoma 6; MUM1: multiple myeloma oncogene-1; Ki67: Antigen Kiel 67)
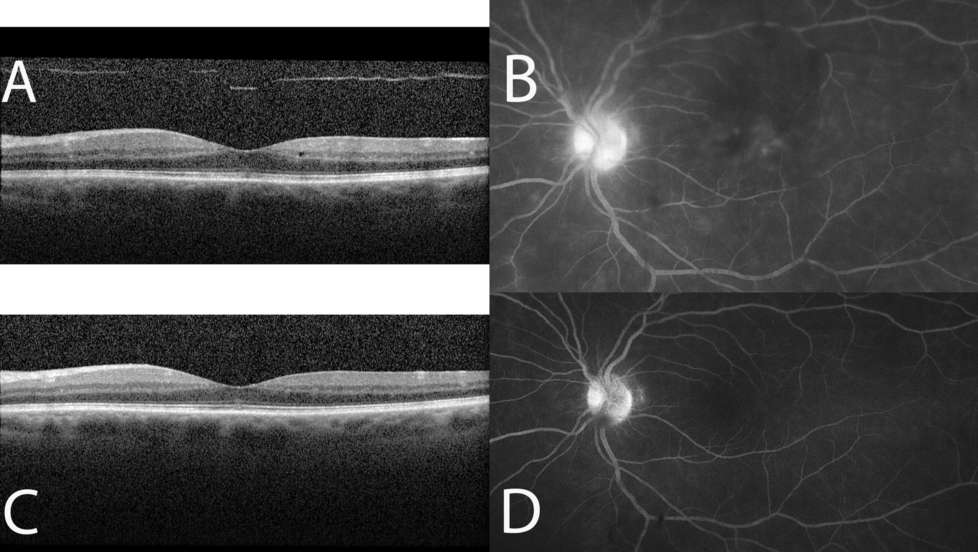
Fig. 5
Ultrawide-field color fundus photo of the right eye demonstrated disc edema with blurry margins and resolved retinal whitening, and arrowheads indicated the area of laser where retinal biopsy was taken (A). OCT of the right eye revealed loss of outer retinal tissue and resolution of macular edema (C). Examination of the left eye remained unchanged (B, D)
留言 (0)