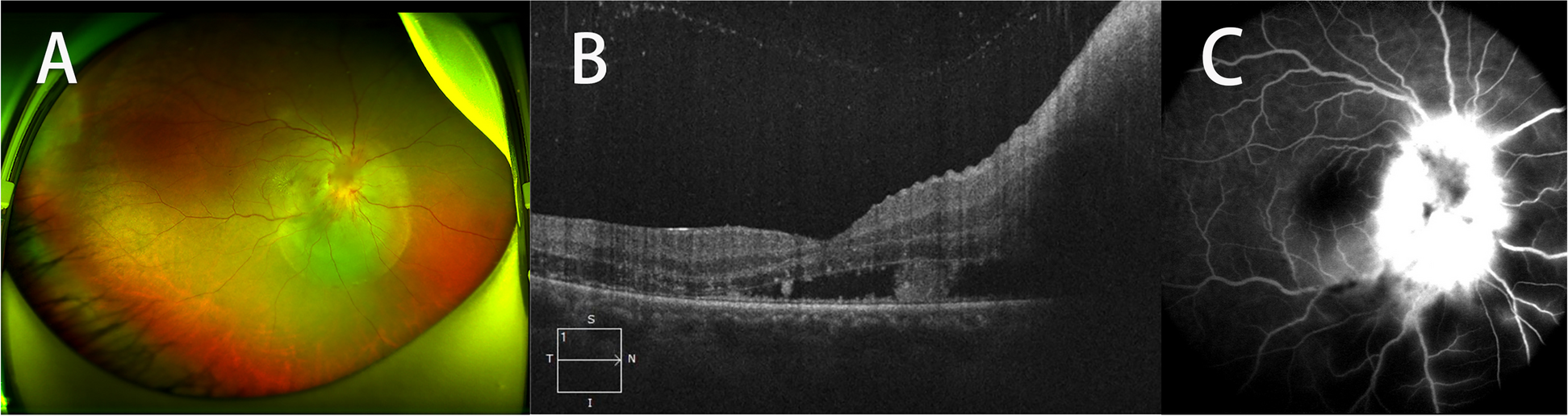
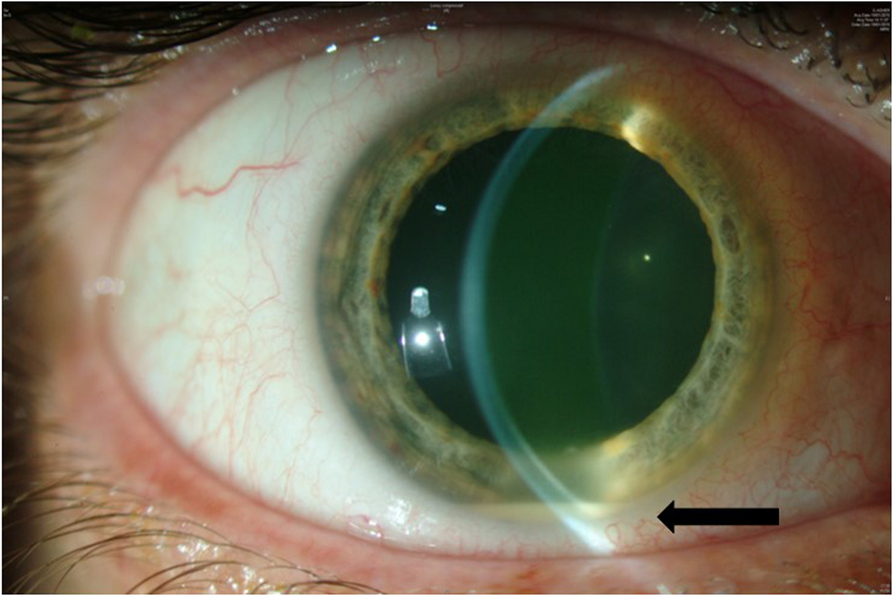
We herein report on the long-term follow-up of a healthy immunocompetent middle-aged patient who was diagnosed with EE secondary to Streptococcus anginosus. The patient presented with cold hypopyon and low-grade uveitis of two-month duration. It was an atypical presentation for a bacterial infection since bacterial endophthalmitis classically presents with an abrupt course and rapid deterioration. Fungal infections on the other hand present insidiously with slow progression [1]. Hypopyon, which is composed primarily of neutrophils, is seen in 35% [1] of EE of bacterial origin. It is termed as 'hot' in the presence of ciliary injection, and 'cold' in the absence of ciliary injection. Cold hypopyon is more commonly seen in patients with uveitis masquerade syndromes [4].
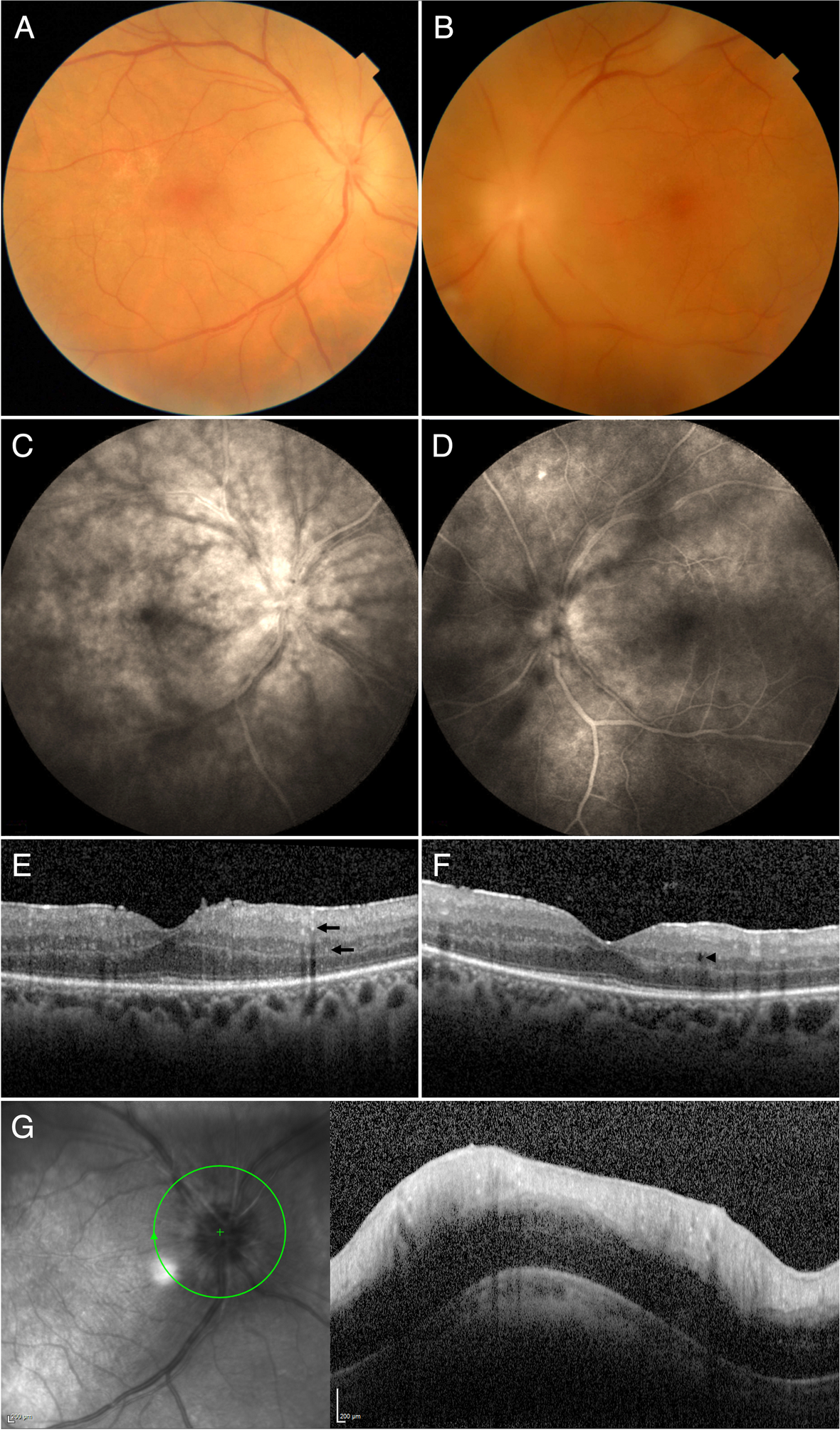
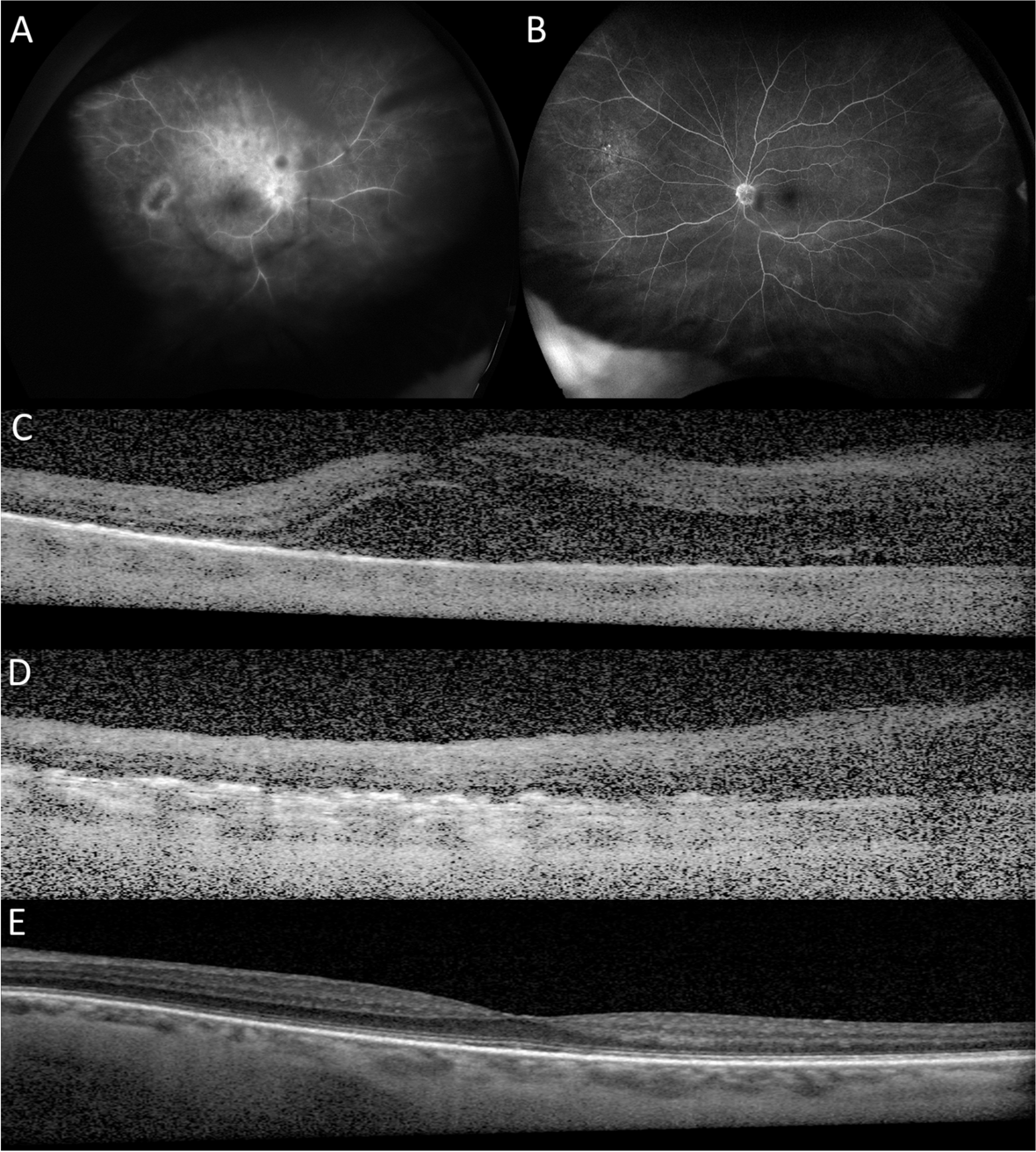
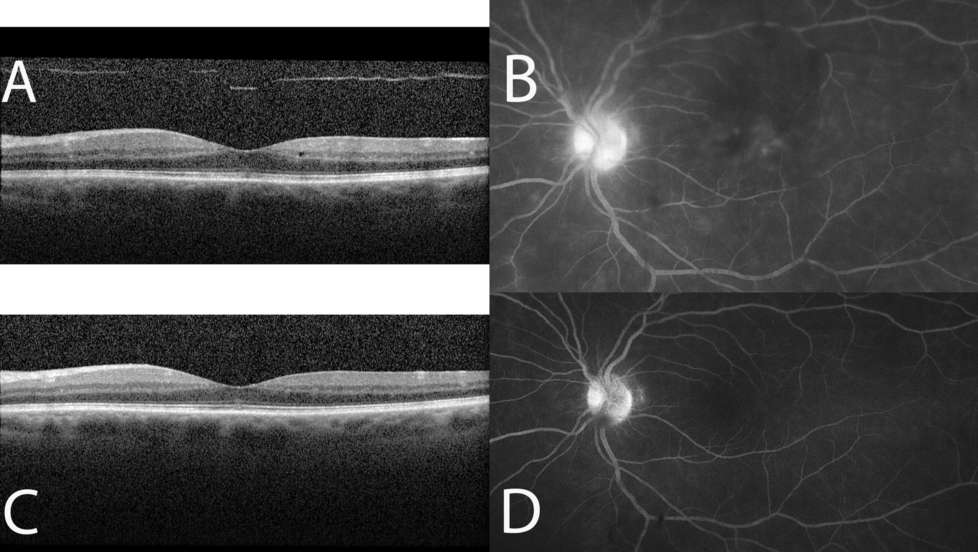
Despite the initial good response to ocular and systemic antibiotics and systemic steroids, persistent intraocular inflammation leading to CME and NVD necessitated aggressive immunosuppressive therapy with IV and intravitreal steroids in addition to azathioprine. When compared with the literature, visual prognosis in EE is usually poor. In a major review by Jackson et al. [1] on 342 cases of EBE, 41% of eyes achieved VA of ≥ 20/200, 35% had VA worse than < 20/200, and 19% required enucleation or evisceration in cases after 2001. Both intravitreal dexamethasone and vitrectomy were each associated with a significantly greater probability of retaining 20/200 vision or better and significantly fewer rates of evisceration or enucleation.
EE occurs when organisms reach the eye via the bloodstream, and then cross the blood ocular barrier. It is a rare but severe infection with poor visual prognosis and an appreciable mortality rate. EBE constitutes 2 to 6% of all cases of endophthalmitis [1]. Diagnostic challenge is encountered in the early stages of the disease, with 16% to 63% of the cases being initially misdiagnosed [1]. EE is frequently associated with many underlying systemic risk factors [1]. The most common risk factors include recent hospitalization, diabetes mellitus, urinary tract infection, immunosuppression, neutropenia, HIV, intravenous drug abuse and indwelling catheters [1].
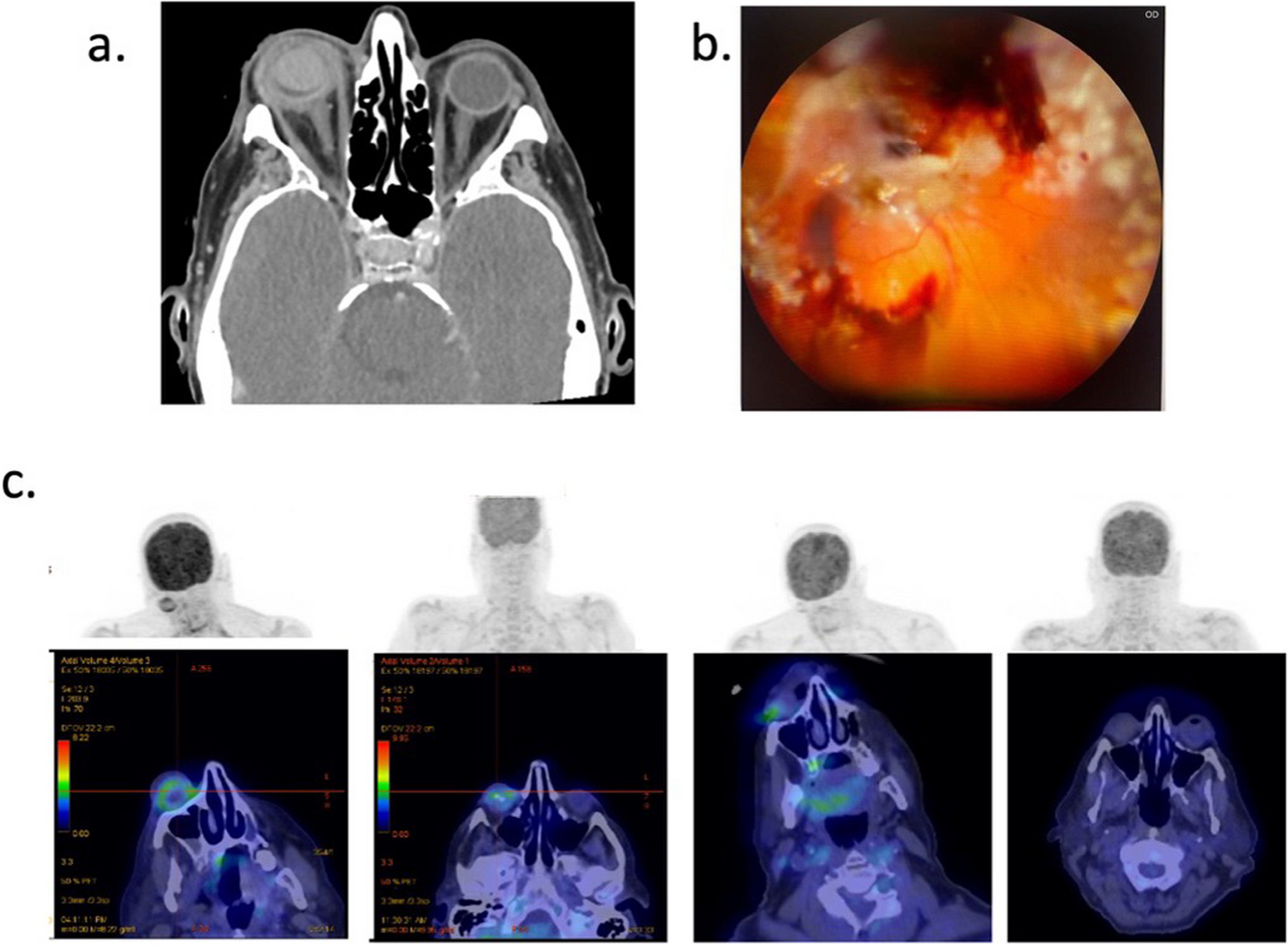
Streptococcus anginosus group, also known as the S. milleri group (SMG), is a subgroup of S. viridans that consists of three distinct streptococcal species: S. anginosus, S. intermedius, and S. constellatus [5, 6]. SMG is found in the oral cavity, nasopharynx, throat, and sinuses. It was reported in association with infective endocarditis, sinusitis, orbital cellulitis, intraorbital abscess formation, and cavernous sinus thrombosis [5,6,7]. EBE resulting from SMG was rarely reported previously [2, 8,9,10,11].
Table 1summarizes 6 cases (5 males) who were diagnosed with SA-associated EE. The median age at diagnosis was 52 years. In three patients, EE was secondary to infective endocarditis (one also had liver abscess). In one patient it was secondary to liver abscess. Blood cultures were positive in all former 4 cases. The youngest reported patient, a 25-year-old woman was healthy with no underlying focus of infection and negative blood culture similar to the index case [9]. She presented with thrombocytosis and elevated CRP and indicated prior facial cellulitis that was treated with oral antibiotics. The index case however was that of a healthy man with no past or present history of any systemic illness or any prior surgical intervention. We speculate that EE in the index case resulted from a remote incidence of transient bacteremia in which bacteria disseminated in the bloodstream and colonized the retina with subsequent infection of the vitreous. Transient bacteremia classically lasts for minutes to a few hours before being cleared from the body, and it is typically harmless in healthy people [12]. This can occur after manipulation of organs normally colonized by bacteria, such as the oral mucosa during tooth brushing, flossing, or dental procedures, or instrumentation of the bladder or colon [12, 13].
Table 1 Demograhic characteristics, co-morbidities, primary focus of infection, presenting and final visual acuity, medical and surgical treatment, vitreous and blood cultures, follow-up period and systemic and ocular complicationsThe index case is unique given the lack of clinical or laboratory evidence of any systemic predisposition to infection and the excellent visual outcome after the longest follow-up of such a case in the literature.
In conclusion, SMG has predisposition to create pyogenic infections complicated by multiple abscesses. SA and the SMG group, known to be virulent organisms, should be contemplated in the differential diagnosis of a slowly progressive endophthalmitis even in immunocompetent patients. Improved outcome is associated with prompt surgical and medical intervention including local and systemic antimicrobial treatment in combination with anti-inflammatory therapy.




留言 (0)