
記住我




A 53-year-old man with a history of chronic HBV hepatitis was admitted to the rheumatology department in August 2020 for low-back pain, left hip pain, and bilateral knee arthritis. He carried a diagnosis of HLA-B27 negative axial spondyloarthropathy (AS), currently failing treatment with a third sequential tumor necrosis factor-α inhibitor (TNFi). He had previously received treatment with etanercept and adalimumab, and was currently treated with intravenous infliximab.
The diagnosis of HLA-B27 negative AS was made in 2017, on the basis of recurrent bilateral knee arthritis and long-standing low-back pain with inflammatory remodeling on the spine magnetic resonance imaging (MRI). In addition to the arthritis, the patient suffered from an unintentional weight loss of roughly 30 kgs in the last 6 months, a low-grade fever chronically hovering around 38 °C, cognitive disorders with personality changes, and he complained of decreased vision with floaters in both eyes during the past year. The patient did not complain of abdominal pain or diarrhea.
Given the unusual presentation for AS and the ineffectiveness of 3 different TNFi (etanercept, adalimumab, and infliximab), the diagnosis of AS was questioned and further investigations were performed.
Laboratory tests revealed an elevated C-reactive-protein (CRP) level at 60 mg/L, and a prolonged erythrocyte sedimentation rate (ESR) at 84 mm/h. Complete blood count found microcytic anemia, with normal white blood cell and platelet counts. Blood electrolytes, renal and liver function tests were normal. Blood cultures and immunologic assays (anti-cyclic citrullinated peptide antibodies, antinuclear antibodies, and rheumatoid factor) were negative, and multiple infectious diseases were serologically ruled out (Treponema pallidum, Rickettsia spp, Coxiella spp, Brucella spp, Bartonella spp, HIV, Cytomegalovirus, and Epstein-Barr virus). Thoraco-abdominal computed tomography (CT) scan revealed portal hypertension with splenomegaly, possibly in the context of chronic HBV hepatitis.
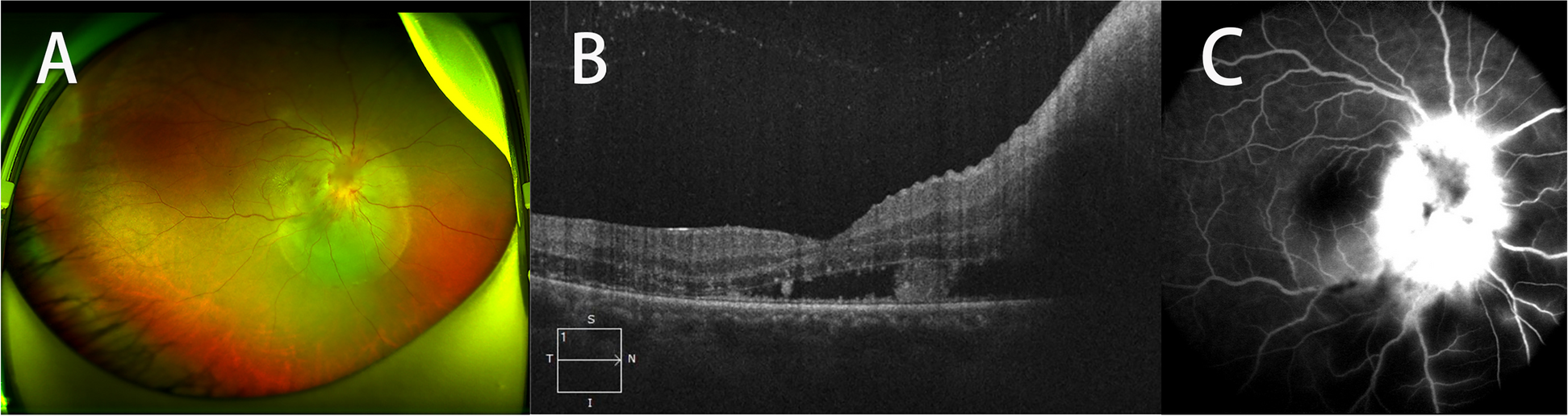
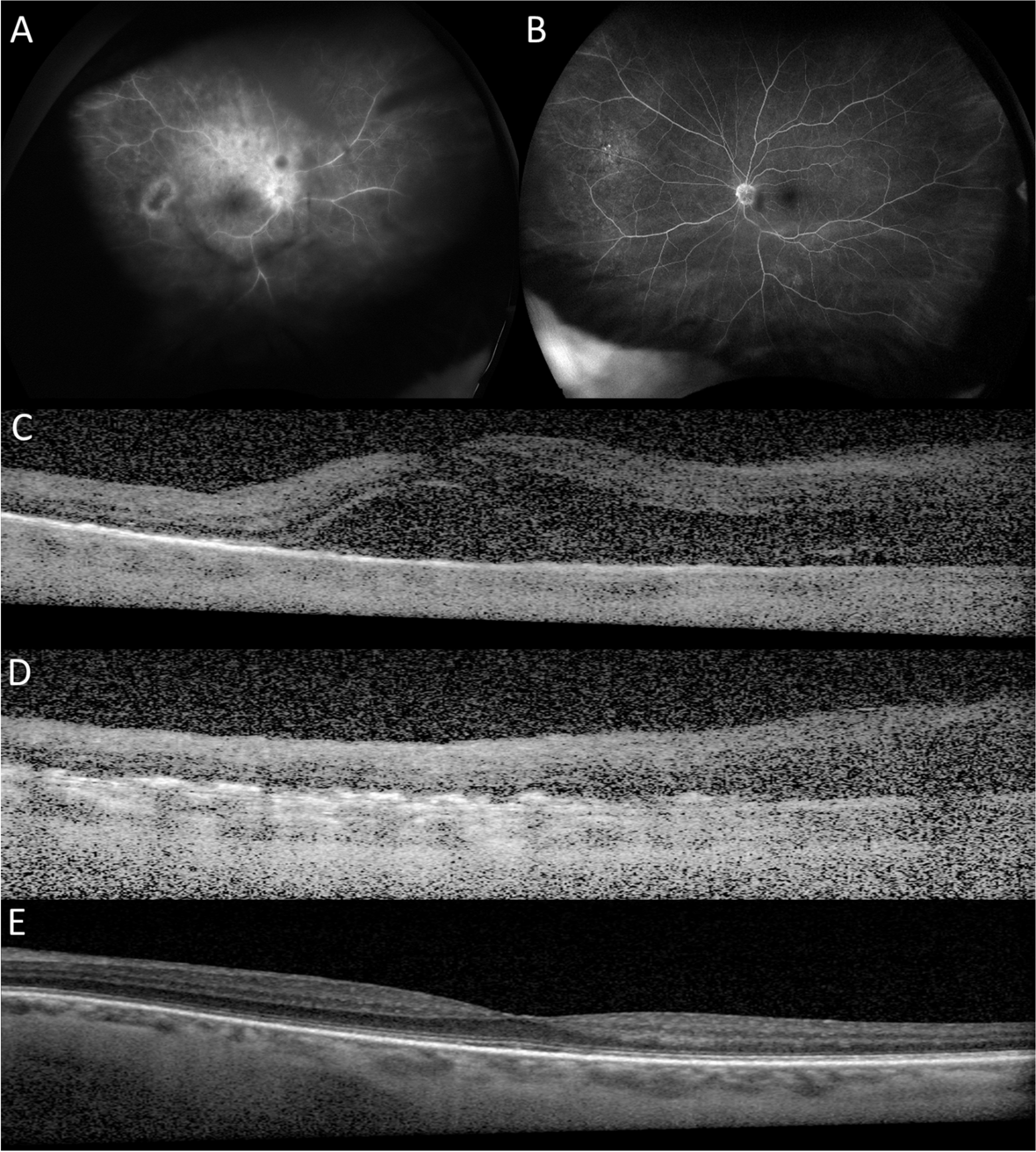
Ophthalmologic examination found a decreased best-corrected visual acuity (BCVA) of 20/30 in both eyes, normal intraocular pressures (IOP), normal slit-lamp examination (SLE) with no anterior chamber cells or flare, presence of 1 + vitritis in the right eye and 3 + vitritis in the left, as well as bilateral optic nerve head edema (Fig. 1A–B). Some snowballs could be also seen in both eyes. Fluorescein angiogram (FA) revealed leakage in both optic nerve heads and venous vasculitis in both eyes (Fig. 1C–D). Indocyanine green angiography (ICGA) was normal in both eyes. Macular and optic nerve head spectral-domain optical coherence tomography (SD-OCT) found bilateral diffuse macular thickening, faint intraretinal exudates, and severe optic nerve head edema (Fig. 1E–G). A diagnosis of bilateral posterior uveitis with mild neuroretinitis and intense vitreous reaction was made.
Fig. 1
Multimodal imaging of Whipple’s disease uveitis at presentation. A Fundus photograph of the right eye revealing minimal vitreous haze associated with severe optic nerve head edema, and mild whitish retinal changes in the temporal macula. B Fundus photograph of the left eye at presentation revealing moderate vitreous haze associated with optic nerve head edema with very hazy details. C Fluorescein angiography (FA) of the right eye showing profuse optic disc leakage, extensive capillary leakage over the entire posterior pole, and an associated area of venous vasculitis at the level of the superotemporal arcade. D FA of the left eye showing moderate optic disc leakage, capillary leakage, and superotemporal venous vasculitis. A small punctiform hyperfluorescent focus can be seen above the disc. E Macular spectral-domain optical coherence tomography (SD-OCT) of the right eye demonstrating a mild epiretinal membrane (ERM), diffuse macular thickening without cystic changes, and some discrete intraretinal hyperreflective dots (arrows). F Macular SD-OCT of the left eye demonstrating a mild ERM, diffuse macular thickening with one intraretinal cystic cavity (arrowhead), and some discrete intraretinal hyperreflective dots. G Optic nerve head SD-OCT of the right eye showing severe disc edema, mainly secondary to retinal nerve fiber layer (RNFL) edema
Considering these elements, the possibility of WD was raised. PCR tests for TW were ordered, and these were positive from multiple sites (blood, urine, saliva, stool, synovial fluid, CSF, and aqueous humor). PCR of duodenal biopsy specimens were also positive for TW. However, periodic acid-Schiff (PAS)-positive foamy macrophages were not seen. These findings led to revise the diagnosis of HLA-B27 negative AS to a diagnosis of classical WD with bilateral posterior uveitis and vitritis.
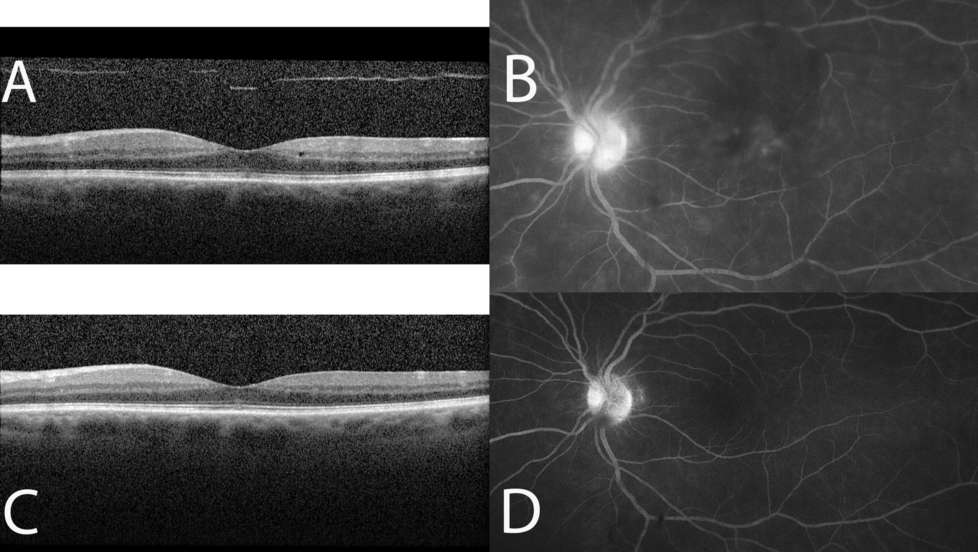
The patient received treatment with intravenous ceftriaxone 4 g/day for one month, followed by a combination therapy of doxycycline 100 mg twice a day and hydroxychloroquine 200 mg three times a day. Betamethasone subconjunctival injections were also performed to control the uveitis. This resulted in a progressive improvement of fever, joint pain, inflammatory syndrome, and weight gain. The ocular inflammation also improved in both eyes with fewer floaters, reduction of vitritis, and reduction of macular and optic nerve head thicknesses (Fig. 2A–C).
Fig. 2
Macular and optic nerve head optical coherence tomography showing initial improvement in anatomical features. A Macular spectral-domain optical coherence tomography (SD-OCT) of the right eye demonstrating mild reduction in diffuse macular thickening, and disappearance of the intraretinal hyperreflective dots. B Macular SD-OCT of the left eye also showing mild reduction in diffuse macular thickening, and disappearance of the intraretinal cystic cavity. C Optic nerve head SD-OCT of the right eye showing notable improvement in disc edema
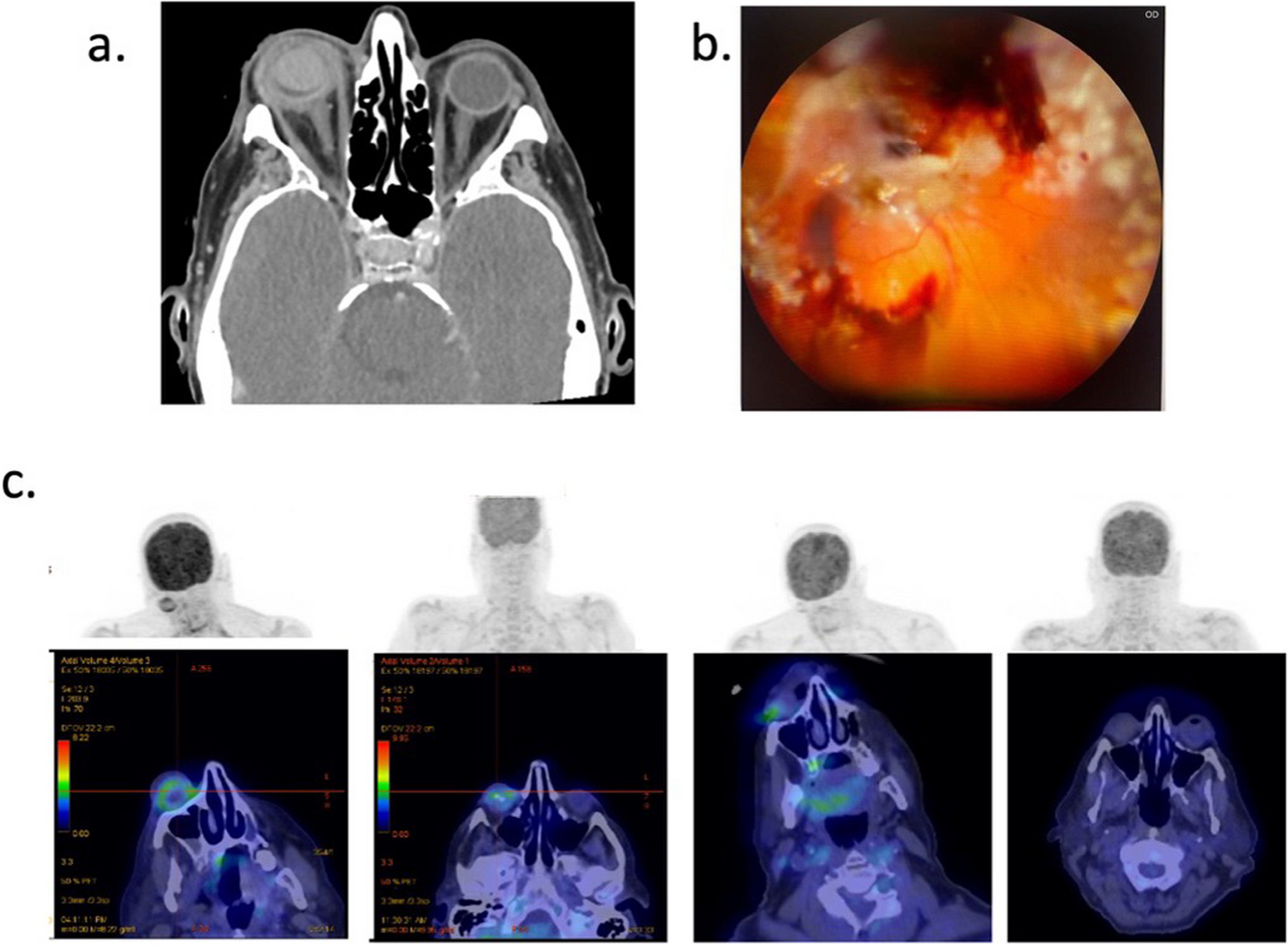
Three months after initiating antibiotic treatment for WD, the patient complained of a recurrence of floaters and vision loss. BCVA was 20/30 in the right eye, and 20/32 in the left, IOP and SLE were unremarkable. Fundus examination showed vitreous precipitates (Fig. 3A). FA showed optic disc edema associated with areas of occlusive vasculitis in both eyes (Fig. 3B–D). Macular SD-OCT found recurrence of macular edema in the right eye. Repeat PCR testing for TW in blood, saliva, stool, CSF, and aqueous humor samples were negative.
Fig. 3
Immune recovery uveitis in Whipple’s disease-associated immune reconstitution inflammatory syndrome. A Fundus photograph of the left eye showing mild vitreous haze, vitreous precipitates and mild optic nerve edema. B Fluorescein angiography (FA) of the left eye revealing vitreous precipitates and mild capillary leakage. C FA of the right eye showing severe optic disc leakage, multifocal segmental arterial (arrowhead) and venous (arrow) vasculitis, severe capillaropathy and grainy hyperfluorescent changes in the macula. D FA of the right eye showing severe ischemic changes in the inferior temporal periphery with multifocal areas of occlusive venous vasculitis
Presence of an inflammatory recurrence after initial improvement under antibiotic treatment and discontinuation of TNFi, and the absence of another identifiable cause for the inflammatory relapse, led to a diagnosis of WD-IRIS in the form of an IRU. We started treatment with intravenous methylprednisolone (1 mg/kg/day for three consecutive days), followed by an oral prednisone tapering regimen (starting at 1 mg/kg/day) during one year. Combination therapy with doxycycline and hydroxychloroquine was continued in parallel to the corticosteroids, and was given for a total of one year. This allowed improvement of the ocular inflammation, with some relapses however.
Indeed, almost 3 years of follow-up were marked by several ocular inflammatory relapses characterized by intermediate uveitis with snowballs predominantly in the left eye without systemic inflammation or symptoms. Inflammatory relapses were treated with subconjunctival triamcinolone acetonide and intravitreal Ozurdex injections, and were complicated by high intraocular pressure (up to 29 mmHg) in the left eye and cataracts in both eyes.
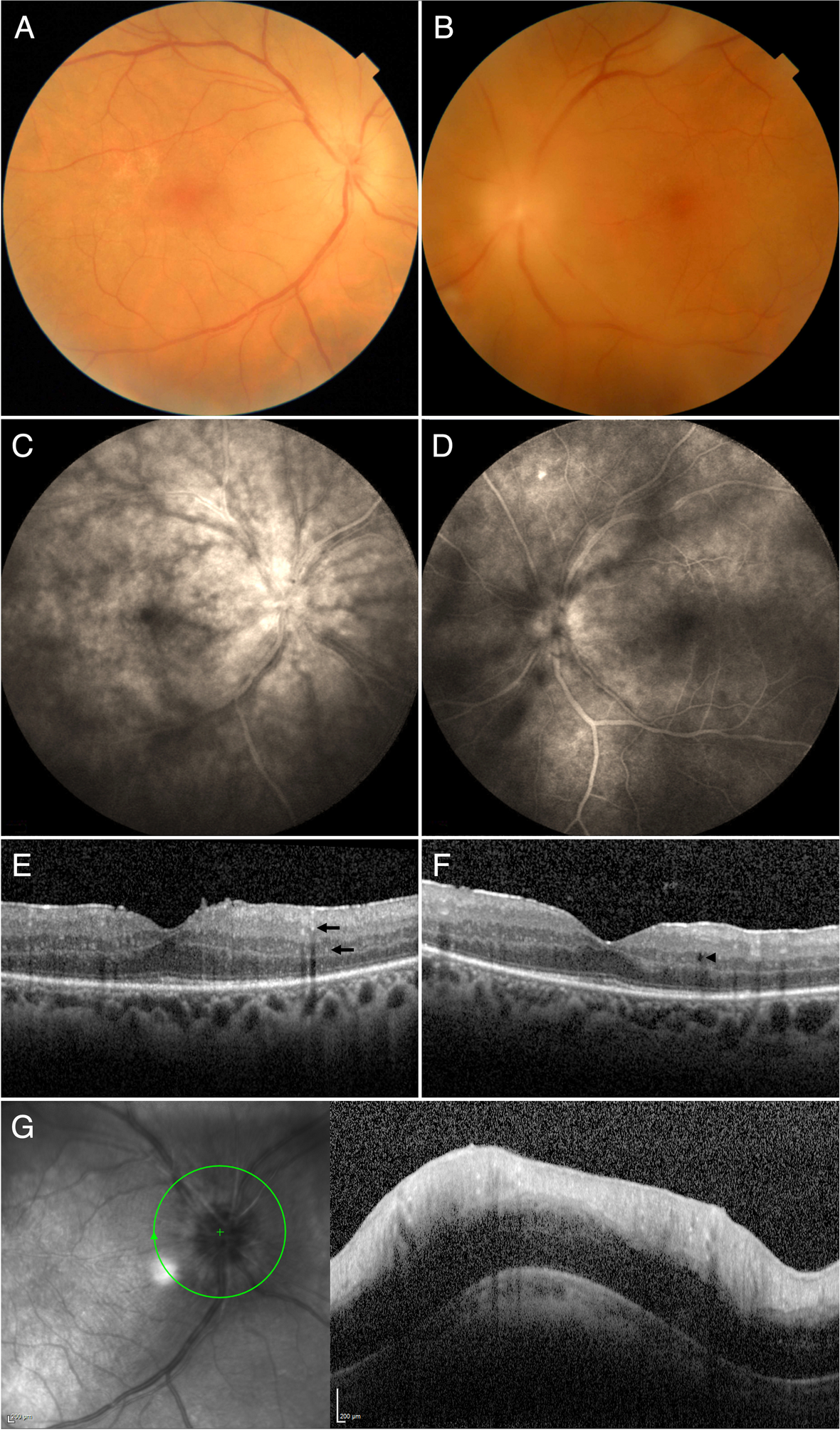
At the last follow-up visit in April 2023, the patient had a BCVA of 20/50 in the right eye, and 20/100 in the left due to uveitic and steroid-induced cataracts. There were some chronic inactive snowballs in the left eye (Fig. 4A–B). Fluorescein angiogram revealed absence of optic nerve head edema, and absence of active retinal vasculitis (Fig. 4C–D). Macular SD-OCT showed normal macular thickness in both eyes.
Fig. 4
Posterior segment findings after 2-year follow-up of Whipple’s disease uveitis and subsequent immune recovery uveitis. A Ultra-wide field (UWF) fundus photograph of the right eye showing discrete temporal venous sheathing (arrows) and a small intraretinal hemorrhage in the inferior temporal periphery (arrowhead). B UWF fundus photograph of the left eye showing hazy details because of subcapsular posterior cataract. Vitreous precipitates can be seen in front of the posterior pole and across the inferior periphery. Note areas of proximal venous vascular sheathing. C UWF fluorescein angiography (FA) of the right eye showing mild capillaropathy, and ischemic areas in the temporal periphery. D UWF FA of the left eye showing multifocal vitreous precipitates, and mild telangiectatic vascular changes in the temporal periphery. No vascular leakage can be seen
留言 (0)