
記住我




A retrospective chart review was performed on all patients who received STA at the University of Colorado Hospital for treatment of uveitic ME between January 1, 2013, and July 31, 2022, from two uveitis fellowship-trained ophthalmologists (AKR or AGP). The study received approval from the Colorado Multiple Institutional Review Board and all research conformed to the tenets of the Declaration of Helsinki. To reduce the chance that uveitic ME changes were due to systemic medication alterations, patients were excluded if there were changes in systemic IMT in the 8 weeks prior to or 4 weeks after STA, or change in systemic corticosteroids in the 4 weeks prior to STA. Exclusion criteria also included a diagnosis of infectious uveitis, lack of follow-up within 12 weeks following STA, or intraocular surgery within the 12 weeks following STA. Only the first STA that qualified was analyzed for eyes that received multiple STA injections in the study time period.
All injections were done as superior posterior sub-Tenon’s injections, using a modified Nozik technique described previously [8]. This method has been found to have similar efficacy as other periocular routes [15, 16]. Adult patients received 40 mg of triamcinolone acetonide, while pediatric patients received 20 mg.
Uveitic ME was defined by a CST greater than 320 μm [5] or the presence of intra-retinal cystoid spaces using a Heidelberg Spectralis OCT machine (Heidelberg Engineering, Heidelberg, Germany), or by the presence of petaloid macular leakage on wide-field FA in the setting of uveitis. FA was obtained at the discretion of the treating physician.
The following data were collected for each patient eye: age, race/ethnicity, sex, history of diabetes mellitus, history of retinal vein occlusion, laterality of uveitis and injection, dosage of STA, uveitis diagnosis, anatomic classification of uveitis, use of regional corticosteroid injections, use of corticosteroid eyedrops, use of systemic corticosteroids, use of systemic IMT, use of intraocular pressure (IOP)-lowering eyedrops, measures of visual acuity (VA) and IOP, grading of anterior chamber and vitreous cell, presence of intra-retinal and subretinal fluid on OCT, presence of epiretinal membrane on OCT, CST on OCT, and presence of petaloid macular leakage on FA. For eyes with CST greater than 320 μm initially, the CST 12 weeks post-STA injection was also obtained.
STA failure was defined as the need for additional corticosteroid therapy, intravitreal anti-vascular endothelial growth factor injections, or intravitreal methotrexate within 12 weeks of STA due to persistent or worsening uveitic ME, as determined by the treating physician. Corticosteroid therapy included additional corticosteroid eyedrops, local injections, and systemic corticosteroid medications.
Statistical analysisPatients could have one or two eyes included in the study analysis. Demographic and clinical characteristics were summarized for eyes that experience STA success versus failure with basic frequencies and percentages for categorical variables and means, medians, and standard deviations for continuous variables. CST was analyzed both as a continuous variable and categorized into tertiles. The rate of STA failure was calculated for all eyes and by select demographic and clinical variables. Univariate and multivariable logistic regression analysis with generalized estimating equations and an unstructured correlation were used to compare eyes that failed versus eyes that succeeded with STA. Missing data were presented in frequencies and percentages, but were not included in statistical comparisons. Multivariable predictors of STA failure included all variables with p-values < 0.10 in univariate analysis with the exception of petaloid macular leakage on FA due to the large number of missing values. Patients with missing CST were also not included in the multivariable model.
ResultsA total of 180 eyes from 131 patients were included in this study (Table 1). Forty-two eyes (23.3%) were considered treatment failures.
Table 1 Patient characteristics by STA success or failure by eyeIn the univariate analysis, there were no significant baseline differences between treatment successes and treatment failures with regards to age, sex, presence of diabetes mellitus, use of systemic steroids, use of systemic IMT, or presence of intra-retinal cystoid spaces or subretinal fluid on OCT. In contrast, in the univariate analysis, treatment failures were less likely to have an anatomic classification of intermediate uveitis and more likely to be using topical corticosteroids and have a baseline CST greater than 331 μm (Tables 1 and 2).
Table 2 Eye-level characteristics by STA success or failureWithin the multivariable analysis, the use of topical corticosteroids (odds ratio [OR], 2.91 [95% CI, 1.07 to 7.95], P = 0.037) and increased CST (OR 1.17 for each 30 μm increase in CST [95% CI, 1.03 to 1.32], P = 0.016) remained statistically significant for failing STA (Table 3).
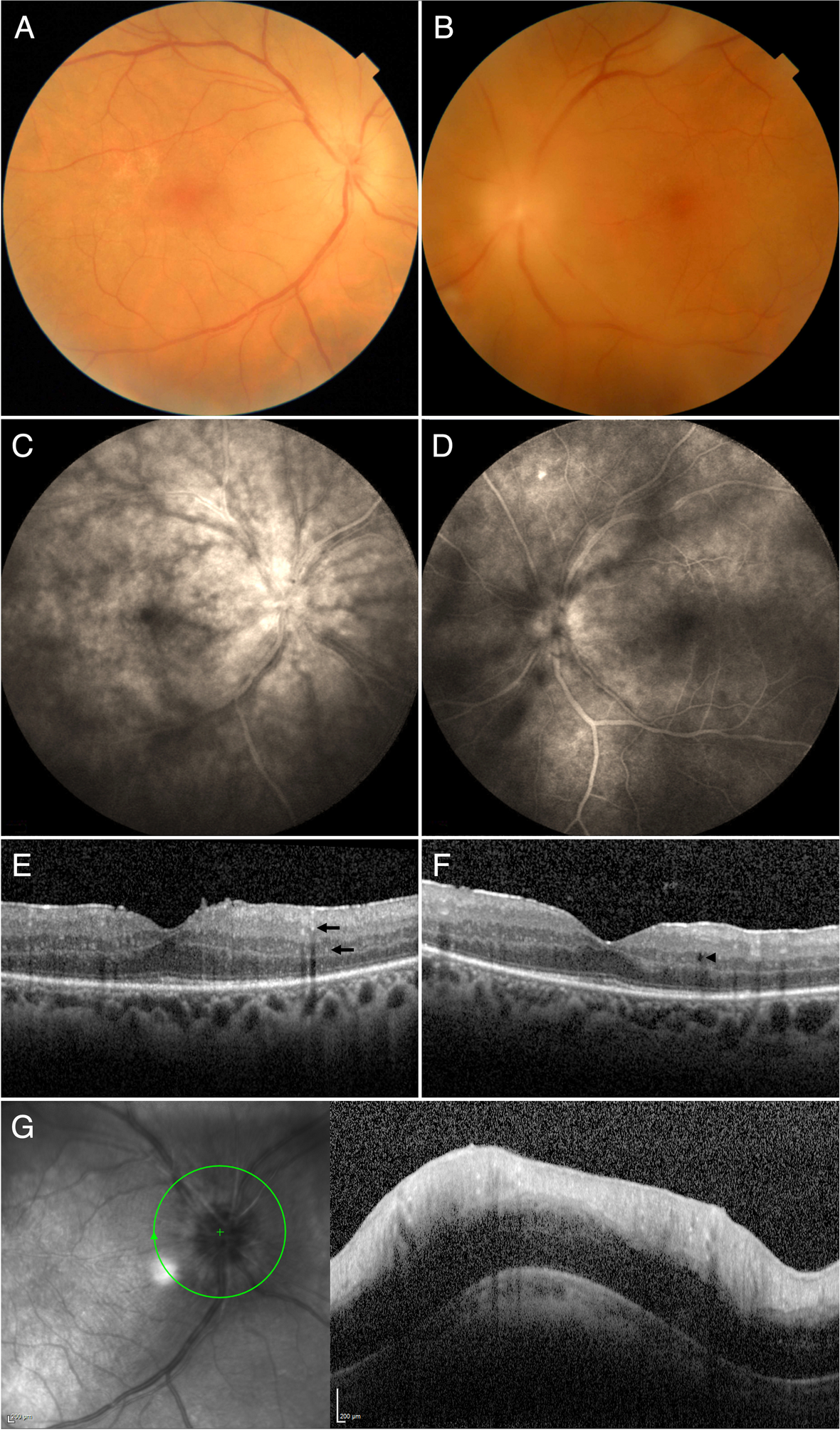
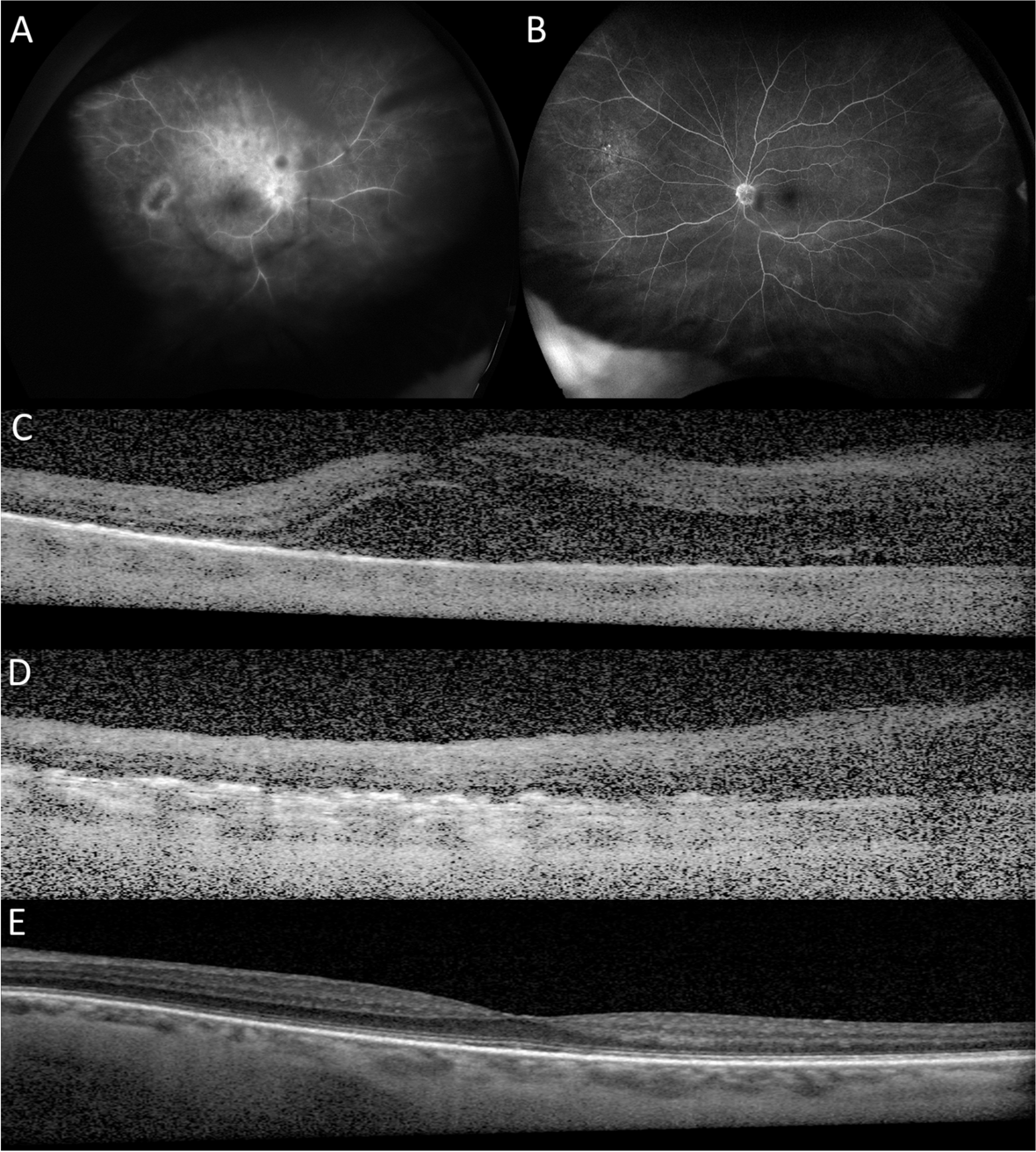
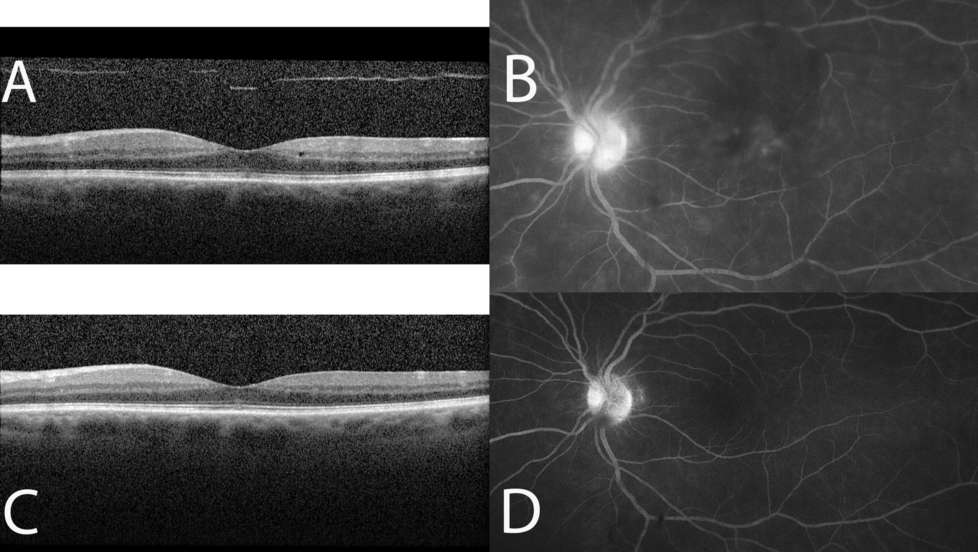
Table 3 Multivariable predictors of STA failureAdditionally, eyes included in this study that would have met criteria for enrollment in the POINT trial (initial CST greater than 320 μm) were statistically more likely to fail STA (22 of 60 eyes = 36.7%) than eyes that would not have met criteria for POINT trial enrollment (initial CST less than 320 μm; 20 failures out of 120 eyes = 16.7%) (P = 0.002). An example of an eye with uveitic ME that responded well to STA but would not have met entry criteria for the POINT trial is illustrated in Fig. 1. The initial OCT macula of the left eye shows intra-retinal cystoid spaces with a CST of 258 μm (Fig. 1a) and the initial FA shows petaloid macular leakage (Fig. 1b). Two months following STA, the intra-retinal cystoid spaces (Fig. 1c) and petaloid macular leakage (Fig. 1d) have resolved.
Fig. 1
Example of an eye with uveitic macular edema that responded well to sub-Tenon’s triamcinolone acetonide (STA) but would not have met criteria for the POINT trial. The initial OCT macula of the left eye shows intra-retinal cystoid spaces with a central subfield thickness of 258 μm (a) and the initial fluorescein angiogram shows petaloid macular leakage (b). Two months following STA, the intra-retinal cystoid spaces (c) and petaloid macular leakage (d) have resolved
DiscussionME is a common cause of vision loss in uveitis [1]. The treatment of uveitic ME often requires the use of local corticosteroids, either intravitreal (IDI or ITA) or periocular (STA), even in the setting of systemic IMT use [4]. STA has some advantages over intravitreal corticosteroids, including decreased rates of ocular hypertension, increased duration of action, no risk of post-injection infectious endophthalmitis or implant migration, and substantially lower expense [5, 9,10,11,12,13,14]. However, the POINT trial found that intravitreal corticosteroids were superior to STA in reducing baseline CST 8 weeks following injection in patients with uveitic ME [5]. The POINT trial, though, only included eyes that had a CST greater than 320 μm on the Heidelberg Spectralis or 300 μm on the Zeiss Cirrus (Carl Zeiss AG, Oberkochen, Germany) or Topcon 3DOCT (Topcon, Tokyo, Japan) – two standard deviations higher than the population normative mean – without consideration for the presence of intra-retinal cystoid spaces on OCT or petaloid macular leakage on FA. While this strict cut-off increases the specificity for ME, it likely selects for eyes with more severe ME and excludes eyes that have ME by parameters other than CST.
Our study indicates that eyes with more severe ME, as defined by a higher CST, are more likely to fail STA for the treatment of uveitic ME. Specifically, each 30 μm increase in CST corresponded to a 17% increased likelihood of failing STA. Similarly, eyes that would have met criteria for the POINT trial were more likely to fail STA than eyes that would not have met criteria for the POINT trial (CST less than 320 μm). Correlating with this, when CST data is segmented into tertiles, eyes in the highest tertile (CST of 331–749 μm) were more likely to fail STA than eyes in the bottom two tertiles. However, it should be noted that over 60% of eyes in this highest tertile for CST still responded favorably to STA in our study.
The use of topical corticosteroids was also associated with an increased likelihood of failing STA in univariate and multivariable analysis. This could be an additional indicator of more severe ME, as the use of topical corticosteroids was at the discretion of the treating physician, and eyes with more severe inflammation and/or ME may have been more likely to be prescribed this additional anti-inflammatory therapy.
The limitations of this study include its retrospective nature, variability of baseline uveitic characteristics and prior treatments, absent data for some variables, and potential patient selection bias, as patients with milder uveitis overall may have been more likely in our practice to have received STA.
ConclusionsOverall, our data suggests that eyes with less retinal thickening secondary to uveitic ME may do well with STA and not require intravitreal therapy. While intravitreal corticosteroids are clearly very effective for uveitic ME, they do have some relative disadvantages compared to STA, of which one of the most important is the substantially higher cost. The preservative-free triamcinolone acetonide required for intravitreal use is approximately four times more and the IDI approximately 70 times more expensive than the triamcinolone acetonide used for periocular injections [17]. In the setting of rising costs of healthcare generally, and intravitreal injections specifically [18], it would be reasonable for clinicians to consider STA as an initial treatment for mild uveitic ME, and then advance to intravitreal therapies as needed.
留言 (0)