
記住我
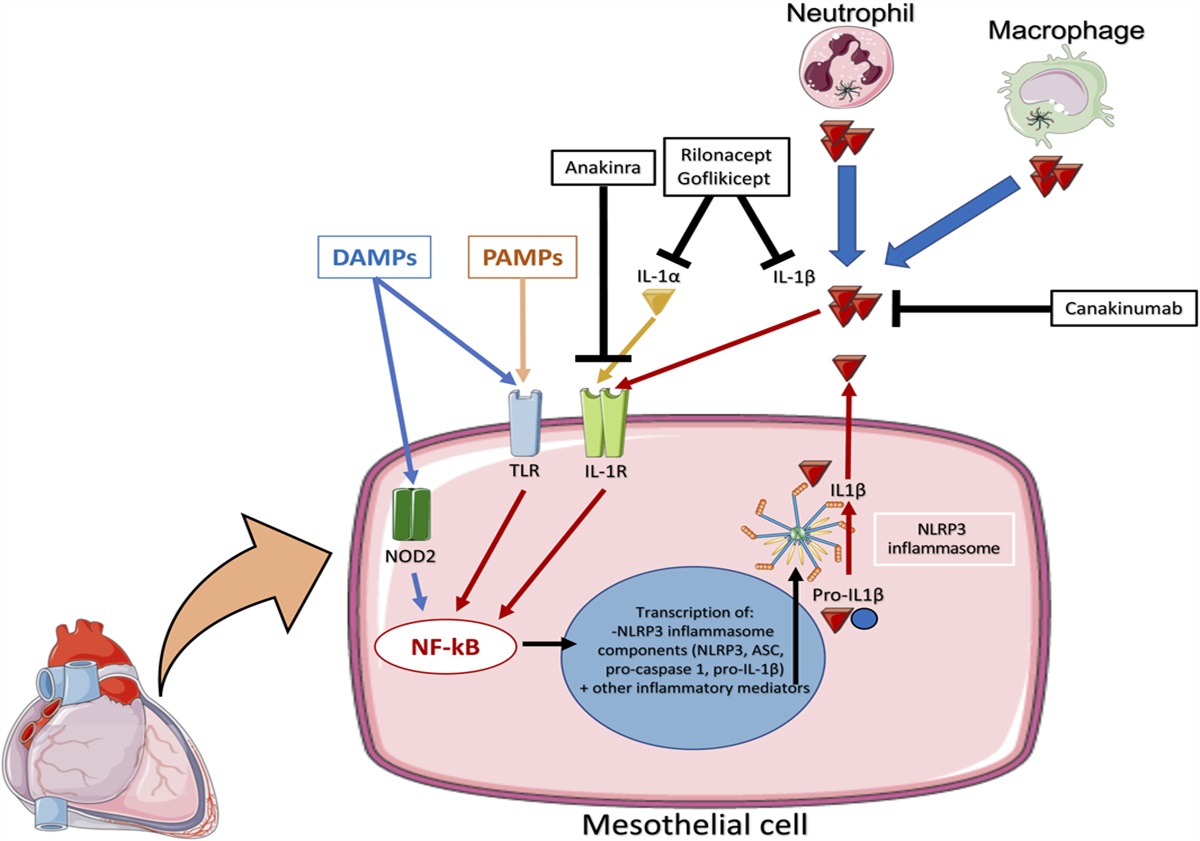



Inflammation plays a central role in coronary artery disease (CAD) pathophysiology. Atherosclerosis and its progression are driven by proinflammatory cytokines such as interleukin-1β (IL-1β), IL-18, and IL-6.1 Cholesterol crystals trigger the formation and activation of the NACHT, LRR, and PYD domains-containing protein 3 (NLRP3) inflammasome, an intracellular sensing and catalytic multiprotein aggregate responsible for the maturation and secretion of IL-1β and IL-18.2,3 Mononuclear leukocytes produce IL-6 in response to IL-1β, leading to neutrophil activation and recruitment in response to tissue damage and to the hepatic synthesis of acute-phase reactants, like C-reactive protein (CRP).4
In patients with established atherosclerotic disease, who are receiving optimal cardiovascular medical therapy, inflammatory biomarkers, like CRP, are predictors of adverse cardiovascular events, at least as strong as cholesterol levels.5 A cohesive concept has been developed that positions high-sensitivity CRP (hsCRP) as an established and reliable prognostic biomarker downstream of the primary inflammatory mediator, interleukin-1 beta (IL-1β).6
In the CANTOS trial (The Canakinumab Anti-inflammatory Thrombosis Outcomes Study), clinically stable individuals with previous myocardial infarction (MI) and “residual inflammatory risk,” defined as persistent elevations in hsCRP ≥2 mg/L despite low levels in low-density lipoprotein cholesterol levels (<70 mg/dL) receiving statins were treated with canakinumab, an IL-1β antibody, or placebo. Canakinumab significantly reduced the rate of myocardial infarction (MI) recurrence, stroke, or cardiovascular death.7
Along these lines, Colchicine,6 an anti-inflammatory drug that inhibits microtubule function and inflammasome formation, has been shown to reduce cardiovascular events in patients with recent MI or stable CAD.8–10 Ziltivekimab, an IL-6 antibody, has also been shown to reduce CRP levels in patients with stable CAD11 and is now being investigated in phase III clinical trials.
In this issue, Dr Yu and colleagues present data on the effects of colchicine and other anti-inflammatory drugs in patients undergoing percutaneous coronary intervention (PCI). Elevated CRP levels pre-PCI and post-PCI are predictors of adverse outcomes, including MI and mortality.12 The investigators sought to measure changes in hsCRP levels. One month after PCI, they compared the effect of colchicine 0.5 mg once daily, tranilast 0.1 g thrice a day, oridonin 0.5 g thrice a day, or standard of care alone for a period of 4 weeks.
Colchicine significantly lowered hsCRP levels, as well as proteins associated with neutrophil activation (azurocidin, myeloperoxidase, myeloblastin), platelet aggregation (glycoprotein VI), and endothelial damage (galectin-3). The effects of colchicine on GP6 (glycoprotein VI platelet) and galectin-3 had not been described before providing a further possible effect for colchicine in CAD treatment. Colchicine has been shown to have broader cellular effects, including inhibition of tubulin polymerization and alteration of leukocyte responsiveness.9–13 Tranilast, a tryptophan metabolite analog, reported to have inhibiting effects in allergic disorders, such as anaphylaxis, bronchial asthma, and hypertrophic scars,14 binds to the NACHT domain of NLRP3 and can suppress the assembly of NLRP3 inflammasome by blocking NLRP3 oligomerization.15 Phase I and II trials studying tranilast administration after PCI in Japan showed that 600 mg of this compound for 3 months reduced the restenosis rate after PCI, even in previously restenotic lesions. A follow-up phase III clinical trial, the PRESTO Trial, failed to show an effect of tranilast on the rates of death, myocardial infarction, or ischemia-driven target vessel revascularization within 9 months or changes quantitative measures of restenosis or its clinical consequences after PCI in patients from the United States. Dr Yu and colleagues used a lower dose of tranilast 100 mg 3 times a day and found no reduction in hsCRP or changes in the levels of the measured proteins. Whether this reflects a lack of efficacy, inappropriate dosing, or a different mechanism remains unexplored.
Oridonin is a traditional Chinese medicinal herb that has a wide range of effects including the binding to the NACHT domain of NLRP3, preventing subsequent NLRP3 inflammasome activation, is now being tested in a cardiovascular setting for the first time. This compound exhibits antitumor, anti-inflammatory, and proapoptotic effects; it is capable of triggering autophagy, enhancing phagocytosis, arresting cell cycle progression, promoting apoptosis associated with the regulation of intracellular reactive oxygen species, Bcl-2/Bax, p53/p21, JNK, nuclear factor-kappa B (NF-κB), MAPK, PI3K, and fatty acid synthesis pathways,16 but up to date, only showed efficacy in clinical trials of peritonitis, type 2 diabetes, and gouty arthritis.17 Dr Yu and colleagues show no effects of oridonin on hsCRP values. This may also reflect an inappropriate dosage or course of treatment.
As for colchicine, the reduction in hsCRP in this trial is consistent with prior trials.8–10 The effects of colchicine on GP6 and galectin-3 further support the anti-inflammatory effects and provide insight into the mechanism of action (Fig. 1). These data are also valuable because they derive from Chinese individuals, a patient group that is generally underrepresented in clinical trials.
 FIGURE 1.:
FIGURE 1.: One month after percutaneous coronary intervention, colchicine, tranilast, and oridonin were administered to patients for an additional 4 weeks. Colchicine reduces microtubule polymerization, inhibits neutrophil activation, inhibits endothelial damage and platelet aggregation, and reduces plasmatic levels of CRP. Tranilast and oridonin failed to show CRP reduction.
1. Abbate A, Toldo S, Marchetti C, et al. Interleukin-1 and the inflammasome as therapeutic targets in cardiovascular disease. Circ Res. 2020;126:1260–1280. 2. Toldo S, Mezzaroma E, Buckley LF, et al. Targeting the NLRP3 inflammasome in cardiovascular diseases. Pharmacol Ther. 2022;236:108053. 3. Toldo S, Abbate A. The role of the NLRP3 inflammasome and pyroptosis in cardiovascular diseases. Nat Rev Cardiol. 2023. doi:10.1038/s41569-023-00946-3. 4. Ørn S, Manhenke C, Ueland T, et al. C-reactive protein, infarct size, microvascular obstruction, and left-ventricular remodelling following acute myocardial infarction. Eur Heart J. 2009;30:1180–1186. 5. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401:1293–1301. 6. Ridker PM. From C-reactive protein to interleukin-6 to interleukin-1: moving upstream to identify novel targets for atheroprotection. Circ Res. 2016;118:145–156. 7. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377:1119–1131. 8. Tardif J-C, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381:2497–2505. 9. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383:1838–1847. 10. Hennessy T, Soh L, Bowman M, et al. The Low Dose Colchicine after Myocardial Infarction (LoDoCo-MI) study: a pilot randomized placebo controlled trial of colchicine following acute myocardial infarction. Am Heart J. 2019;215:62–69. 11. Ridker PM, Devalaraja M, Baeres FMM, et al. IL-6 inhibition with ziltivekimab in patients at high atherosclerotic risk (RESCUE): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. 2021;397:2060–2069. 12. Kalkman DN, Aquino M, Claessen BE, et al. Residual inflammatory risk and the impact on clinical outcomes in patients after percutaneous coronary interventions. Eur Heart J. 2018;39:4101–4108. 13. Opstal TSJ, Hoogeveen RM, Fiolet ATL, et al. Colchicine attenuates inflammation beyond the inflammasome in chronic coronary artery disease: a LoDoCo2 proteomic substudy. Circulation. 2020;142:1996–1998. 14. Darakhshan S, Pour AB. Tranilast: a review of its therapeutic applications. Pharmacol Res. 2015;91:15–28. 15. Huang Y, Jiang H, Chen Y, et al. Tranilast directly targets NLRP3 to treat inflammasome-driven diseases. EMBO Mol Med. 2018;10:e8689. 16. Xu J, Wold EA, Ding Y, et al. Therapeutic potential of Oridonin and its analogs: from anticancer and antiinflammation to neuroprotection. Molecules. 2018;23:474. 17. He H, Jiang H, Chen Y, et al. Oridonin is a covalent NLRP3 inhibitor with strong anti-inflammasome activity. Nat Commun. 2018;9:2550.
留言 (0)