The LEMCAM study shows the experience with alemtuzumab in a real-life cohort of 115 patients treated between 2014 and 2020 and followed a median of 2.8 years in five hospitals in Spain. Results concluded that in patients diagnosed with RRMS for a mean of 7 years, most of them treatment-experienced, two courses of alemtuzumab led to clinical remission and EDSS stabilization, with no unexpected safety issues. Patients were more likely to experience CDI than CDW over time.
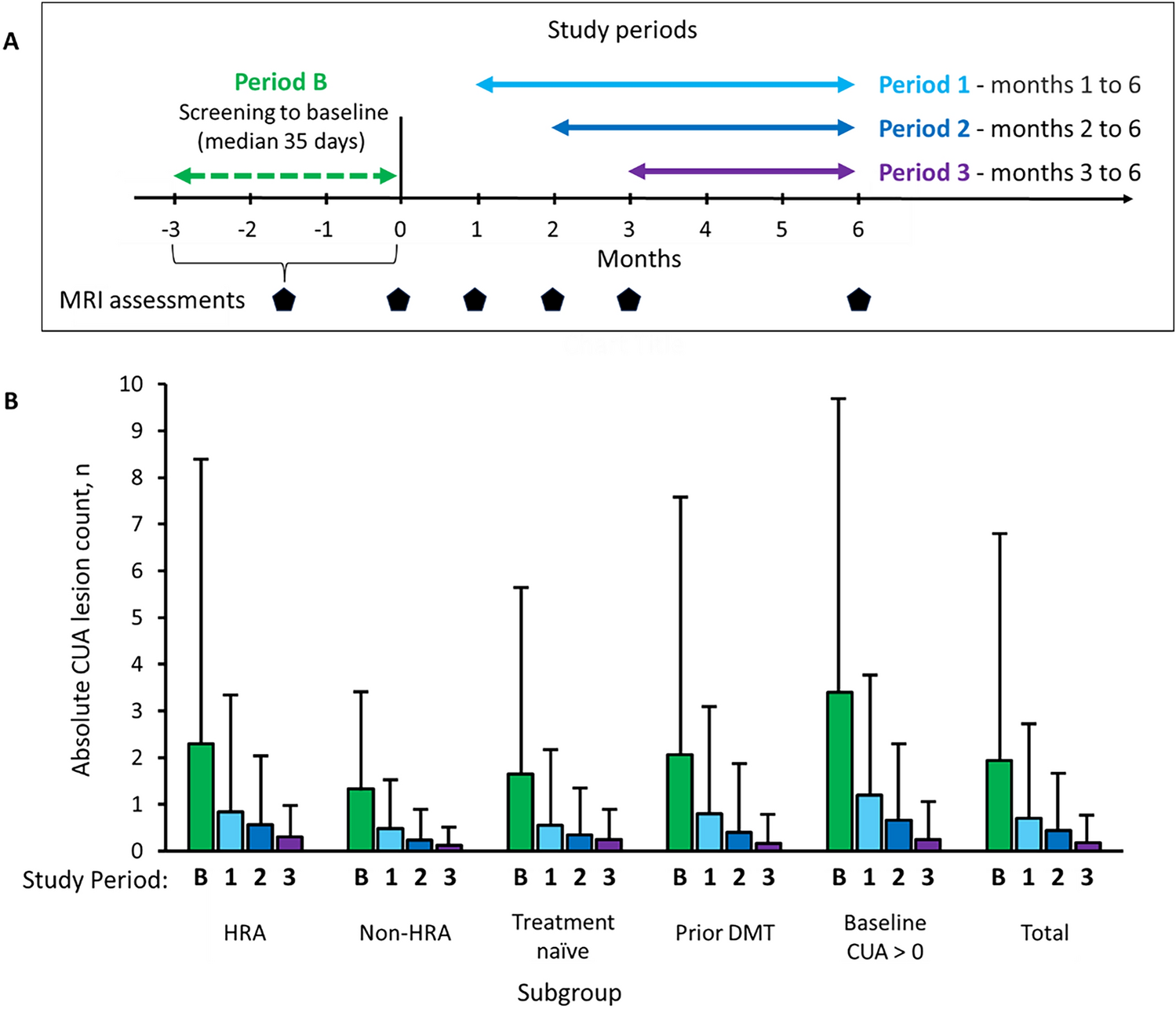
Despite being a clinically active population, with a mean of one relapse in the previous 12 months, patients in LEMCAM achieved clinical disease control with a significant reduction (87%) in the ARR from baseline in year 1 after treatment with alemtuzumab, which remained low from 2 to 4 years, as well as favorable radiological outcomes. However, caution should be exercised when interpreting data from year 4 and beyond due to the limited number of patients.
These findings are consistent with other observational studies supporting the effectiveness of alemtuzumab on clinical activity in patients with different treatment histories, regardless of the number of prior relapses and level of disability. If we focus on two of the larger cohorts, the TREAT-MS study showed similar longitudinal reductions in ARR and sustained EDSS from baseline status [16] in mainly pretreated patients, with more relapses and lower EDSS scores than patients in LEMCAM before treatment with alemtuzumab [20]. Russo et al. [13] found a decrease in disease activity comparable to LEMCAM in patients with similar EDSS scores and lower baseline ARR. The cumulative improvement in disability after 2 years of alemtuzumab was, however, lower in LEMCAM.
Two recently published studies, one of which was conducted in Spain, also showed significant reductions in ARR in cohorts that differ notably in terms of patient age, disease duration, and disability [10, 14]. We observed very low rates of disability worsening during the first 2 years of starting treatment with alemtuzumab, and no patient experienced 6-month confirmed disability progression over years 4–5. The probability of CDI was higher than the probability of CDW. The rates of CDI observed in our cohort are lower than those reported in the CARE-MS I and CARE-MS II clinical trials and their respective 5-year extensions [2, 4,5,6], which ranged from 22 to 43%. This is probably because our patients had higher disease activity and disability, were older, and had received more previous treatments before alemtuzumab, the latter two being associated with worse outcomes [21]. The differences we also observed in the proportion of patients achieving CDI compared to other real-world studies (from 11.8 to 48.8%) [9, 10, 12, 14] may be the result of the diverse range of alemtuzumab-treated patients in clinical practice. When interpreting our CDI results, it is important to consider the stability of the EDSS scores in this cohort without significant improvements, as the CDI is a measure that captures sustained and clinically meaningful changes.
The proportion of patients who reached NEDA-3 at 1, 2, and 3 years were 72%, 79%, and 80%, respectively, and 37% maintained NEDA-3 status through the 5-years of follow-up. Although differences in methods and populations make comparison challenging, these results mirror those obtained in the extension of the CAMMS223 trial (as high as 63–78% per year) [7] and CARE-MS I (62% at 3-year follow-up) in naive patients [6], the extension of CARE-MS II after mainly two DMTs (53% at 3-year follow-up) [5], and the observational cohorts of Russo et al. (58.9% at 2-year follow-up) [13], Prosperini et al. (45% at 3-year follow-up) [12], and di Ioia et al. (67% at 3-year follow-up) [9] in patients exposed to a mean of three and four prior treatments. In LEMCAM, treatment with alemtuzumab led to an overall high NEDA-3 rate irrespective of previous DMT, including in treatment-naive patients (16%).
Alemtuzumab has a special dosing regimen, which may partially explain the low discontinuation rate we found. In our study, only 3% of patients discontinued alemtuzumab due to a lack of effectiveness and fewer than 1% for safety reasons. Safety findings were consistent with those reported in clinical trials, despite differences in age, disease duration, baseline EDSS, and previous treatments, and no new safety concerns were identified in our practice setting. As expected, the most frequent AEs were IRRs, generally easily managed, but the incidence was higher in LEMCAM (95%) than in the recent real-world cohorts of Brecl Jakob et al. (59%) [22], Bose et al. (80%) [21], and di Ioia et al. (78%) [9]. Infections were also more frequently reported in LEMCAM (74%) than in these cohorts (ranging from 2.8% to 27.5%) [9, 12, 21, 22]. However, we found a lower incidence of thyroid autoimmune disorders than in those studies and a similar incidence of ITP [9, 21, 22]. Given that safety was a major concern for the investigators, AEs were thoroughly collected regardless of the possible relation to the drug. The main limitations are the retrospective nature of the study, as the data were derived from medical records not intended for research purposes and therefore some information may be missing, and the lack of a comparator group for reference. We acknowledge the likely heterogeneity in clinical management due to the multicenter nature of the study and that a systematic follow-up performed with standardized timings would have strengthened the study results. Also, the different follow-up periods between the study participants and the small number of patients from year 4 and beyond limit the ability to draw conclusions about the long-term benefits of alemtuzumab.

留言 (0)