
記住我
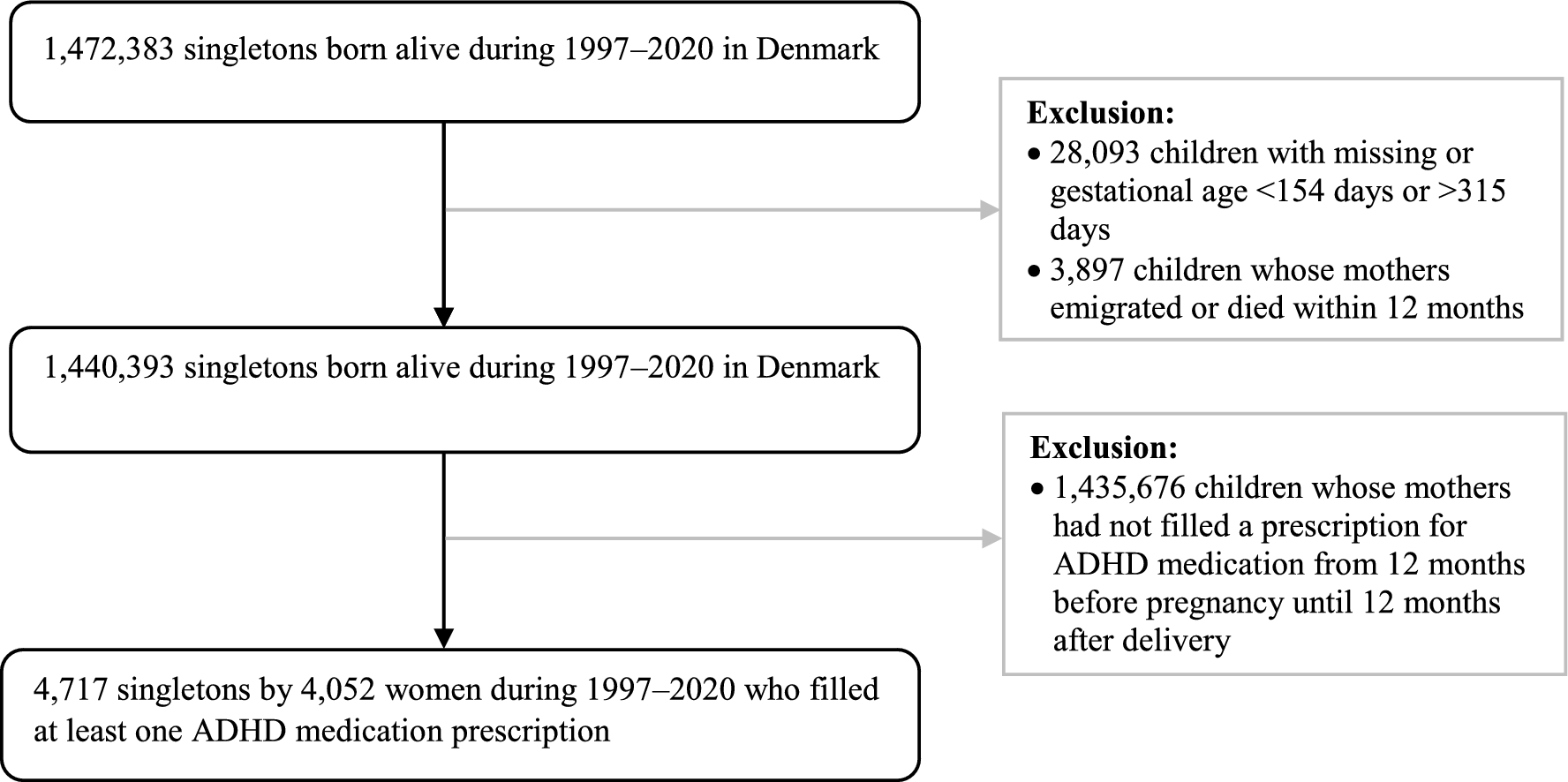
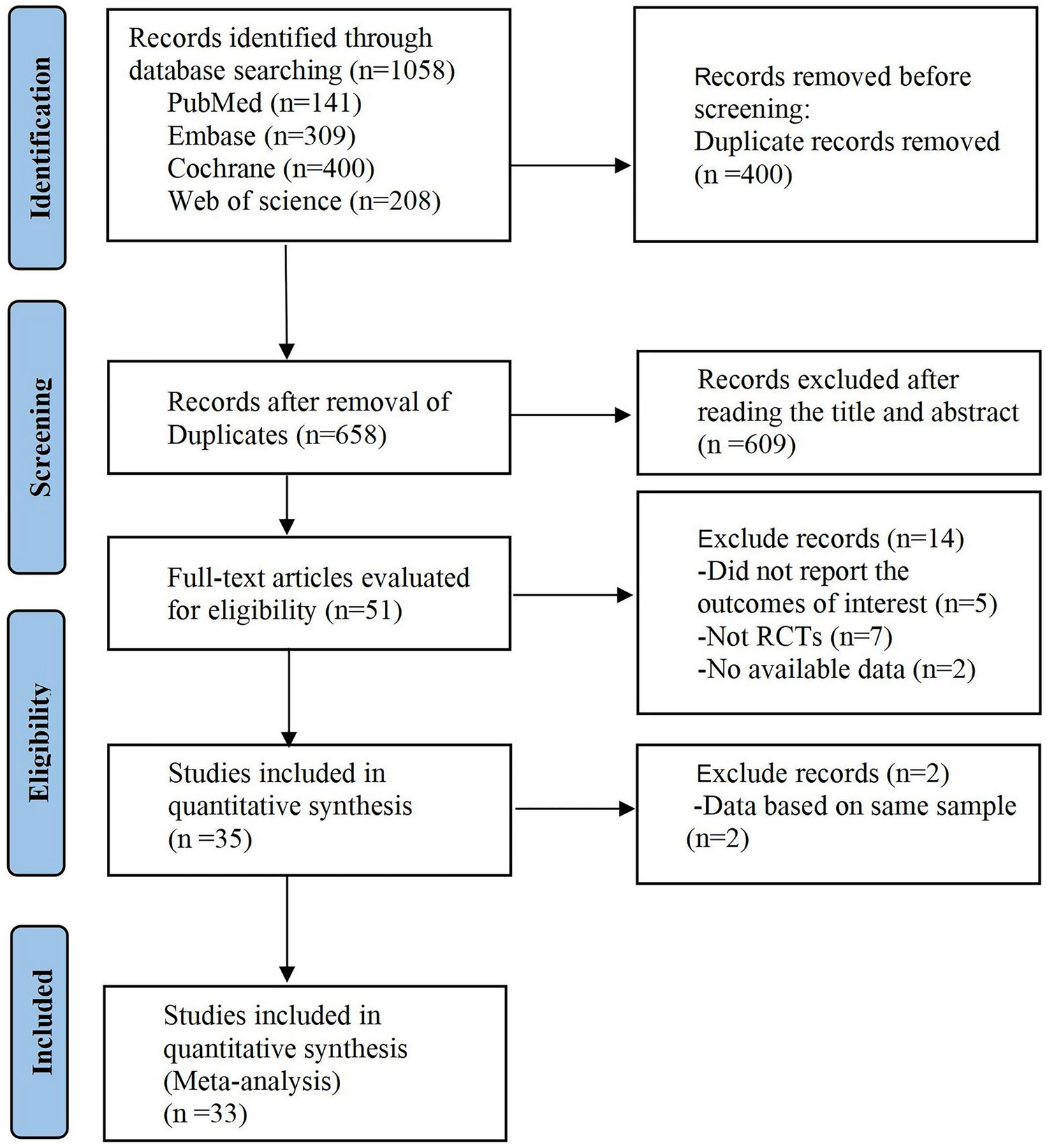
We conducted a population-based cohort study utilizing Danish nationwide registers. All residents in Denmark are assigned a unique personal identification number, enabling data linkage between registers. We first identified all pregnancies leading to singleton live births between 1997 and 2020 from the Danish Medical Birth Register (N = 1,472,383) [19]. To ensure data accuracy, we excluded 28,093 (1.9%) pregnancies with missing or extreme gestational age (<154 days or >315 days), as well as 3897 (0.3%) pregnancies by women who emigrated or died within 12 months after delivery to ensure data completeness for ADHD medication use in the defined period (Fig. 1).
Fig. 1
Identification of the study population. ADHD attention-deficit hyperactivity disorder
2.2 Attention-Deficit Hyperactivity Disorder (ADHD) MedicationWe obtained data on ADHD medication dispensations from the Danish National Prescription Registry, which provides information on the Anatomical Therapeutic Chemical (ATC) classification codes and the date of prescriptions filled in community pharmacies in Denmark since 1995 [20]. We included the following ATC codes to identify all medications that are prescribed for the treatment of ADHD in adults [11] in line with previous work [21] acknowledging that some are third- or fourth-line treatments for ADHD: stimulant ATC codes N06BA01, -02, -04, and -12 (amfetamine, dexamfetamine, methylphenidate, and lisdexamfetamine, respectively), and non-stimulant ATC codes N06BA07 and -09, C02AC01 and -02 (modafinil, atomoxetine, clonidine, and guanfacine, respectively).
To define ADHD medication treatment status, we identified women who had filled a prescription within 3-month intervals spanning from 12 months prior to time of conception to 12 months after delivery, totaling 33 months and comprising 11 estimation periods (including the 9 months of pregnancy). The 11 estimation periods are (1) from 12 to 9 months before pregnancy start; (2) from 9 to 6 months before; (3) from 6 to 3 months before; (4) from 3 months to pregnancy start; (5) first trimester; (6) second trimester; (7) third trimester; (8) from delivery to 3 months postpartum: (9) 3–6 months postpartum; (10) 6–9 months postpartum; and (11) 9–12 months postpartum. Exposure to ADHD medication was coded as a binary variable (1) if the dispensation date occurred within the 3-month interval, or 0 otherwise. Date of conception was calculated by subtracting gestational age from the date of birth obtained from the Danish Medical Birth Register. Gestational age at birth was derived from ultrasound scans during the first or second trimester, or, if missing, conception was established using the initial day of the mother's last menstrual period [19].
2.3 Sociodemographic and Health-Related Maternal CharacteristicsWe analyzed clinically relevant sociodemographic and health-related characteristics of the mothers to explore their association with ADHD medication use trajectory during pregnancy and the postpartum period. Maternal age at the start of pregnancy (<25, 25–34, ≥35 years), primiparity (yes/no), smoking during pregnancy (yes/no), and calendar year of pregnancy (1996–2005, 2006–2010, 2011–2015, or 2016–2020) were retrieved from the Danish Medical Birth Registry. Marital status (married or co-habiting, single, divorced or widowed), and level of education (mandatory school, above mandatory school) in the year of pregnancy were retrieved from Statistics Denmark's socioeconomic registers [22]. We also considered clinical characteristics, including age at the first ADHD diagnosis, previous prescriptions of stimulants (ATC codes N06BA01, -02, -04, -12) and non-stimulants (ATC codes N06BA07 and -09, C02AC01 and -02), and other diagnosed psychiatric disorders (substance abuse disorders, psychotic disorders, mood/affective disorders, anxiety and stress-related disorders, eating disorders, sleep disorders, personality disorders, and other psychiatric disorders) any time prior to the trajectory period (12 months before pregnancy), inpatient and outpatient treatment for psychiatric disorders and somatic disorders in the year preceding the trajectory period, and sex of the child. ADHD onset was defined as the first ADHD diagnosis recorded in the Psychiatric Central Research Register or the first date of filling an ADHD medication, whichever came first. We also examined co-prescribed psychotropic medications (antidepressants, antipsychotics, opioid analgesics, anxiolytics and hypnotics, antiseizure medications, and drugs used in alcohol or opioid dependence), including any date for redeemed prescriptions from 12 months prior to pregnancy to 12 months after delivery. We considered a woman exposed to a co-prescribed medication if the date of dispensation occurred within a specific 3-month interval. Additional information on the International Classification of Diseases (ICD) Eighth Revision (ICD-8) and Tenth Revision (ICD-10) codes (ICD Ninth Revision [ICD-9] was never implemented in Denmark) for psychiatric diagnoses, and ATC codes for co-prescribed medications, can be found in Online Resource Table 1 and Table 2, respectively.
Table 1 Characteristics of women with attention-deficit hyperactivity disorder, by trajectory group2.4 Statistical AnalysisWe applied group-based trajectory modeling to classify women into subgroups based on the identification of heterogeneous ADHD medication treatment patterns, using ‘traj’ in Stata version 16.0 (StataCorp LLC, College Station, TX, USA). We fitted group-based trajectory models with one to six groups and tested each model with linear, quadratic, and cubic terms to determine the best shapes that fit the data. We then decided the optimal number of trajectory groups based on four criteria: (1) Bayesian information criterion (BIC) and Akaike Information Criteria [23], with a lower BIC and AIC indicating a better model fit [24]; the BIC log Bayes factor approximation was defined as 2 × [ΔBIC] (subtracting a less complex model from a more complex model), and 2 × [ΔBIC] higher than 10 is considered solid evidence in favor of the more complex model; (2) an average posterior probability of ≥0.7 in each group identified; (3) a trajectory group had to constitute ≥10% of the total sample; and (4) clinical relevance, i.e., whether the trajectory groups have practical utility in guiding treatment decisions or interventions. Women were assigned to the trajectory with the maximum posterior group probability [25].
2.5 Sensitivity AnalysesIn a sensitivity analysis, we restricted the analyses to 2710 primiparous pregnancies to address the concern about any dependency between pregnancies by the same woman. Furthermore, we restricted our analysis to 4344 term-born children to evaluate the potential impact of gestational age on the trajectories.
In reporting the study, we followed the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.
留言 (0)