
記住我


Co-located low-threshold transitional housing and clinical services were implemented urgently to address worsening conditions in Boston tent encampments in February 2022. We describe the model, key transitional housing metrics, and preliminary clinical service outcomes. This work was approved by the Boston University Medical Campus Institutional Review Board (protocol H-43035).
SettingBMC established the following services in a former hotel known as the “Roundhouse (RH)” in February 2022:
1.Low-threshold, transitional housing
The RH offers sixty beds of transitional housing for tent encampment residents, with transitional housing eligibility not contingent upon abstinence from substances or SUD treatment engagement. The Boston Public Health Commission (BPHC) refers residents from encampments and manages a waiting list of former encampment residents and other people experiencing homelessness. Rooms are single or double occupancy with private bathrooms and have locking doors. The RH transitional housing program accepts individuals and couples, who have the option of being housed together or separately. Meals are delivered from City Fresh [24] and are available for pick up from the lobby three times daily.
RH transitional housing is staffed by case managers and harm reduction specialists. Due to the ongoing risk of overdose, staff provide around-the-clock safety checks of residents while they are in their rooms in order to help prevent overdose deaths. Harm reduction specialists also distribute harm reduction equipment (e.g., safer injection kits), link residents to community resources, and lead meetings and programming for residents. Case managers meet with residents individually and support connection to stabilization services and navigation to secure permanent supportive housing, based on need. The case manager-to-resident ratio is 1:15, with regular meetings scheduled between residents and their respective case managers on a weekly basis or as required, depending on the residents’ needs. Case managers provide assistance with preparing for, and transitioning to, permanent supportive housing, including obtaining identification documents, clearing warrants, and assisting residents to engage with clinical services in order to stabilize medical, mental health, and SUD issues. They also help enroll clients in benefits programs, provide conflict resolution, assist with family reunification, and provide emotional support.
Security guards are on site 24/7 and perform metal-detector searches for weapons when people enter the facility, but they do not search resident rooms or confiscate harm reduction equipment. Residents are provided with private “personal property lockers” external to the building, which are not searched. Residents are informed that substance use is prohibited in the building; if substances are observed (e.g., at the time of building entry), residents are reminded of facility policies and are guided towards using their lockers to store anything that they cannot bring inside of the building.
Roundhouse housing residents are also supported by other case management and clinical agencies. They are free to engage with any outside service agency, and in addition, several agencies provide personnel who come on-site to provide support. This includes Boston Healthcare for the Homeless Programs, which provides a half day per week of “home visits” to residents in their Roundhouse rooms, with a goal of enrolling residents in primary care or providing primary care services to residents who are not willing or able to attend clinical office visits. A MA Department of Mental Health (DMH) case manager is on site one half day per week, with a primary goal of enrolling residents who are DMH service-eligible into their programs. See Table 1 for a list of example external agencies that collaborate on providing clinical and case management stabilization services for people who are experiencing homelessness in the Mass and Cass area.
Table 1 Agencies and organizations that collaborate to provide services to people living unhoused in the Mass and Cass neighborhood of BostonTable 2 Services offered in the Roundhouse clinical unitsRH clinical services are located on the basement level of the facility and serve both housing residents and other people experiencing homelessness and SUD, who access services primarily on a walk-in basis. Patients are triaged to one of two options:
a.Low-barrier SUD Walk-In Urgent Care Clinic
This outpatient clinic provides medications for SUD, infection treatment/screening/prevention services, contraception, and harm reduction education and supplies.
b.24/7 Short-Stay Stabilization Unit (Fig. 2)
Fig. 2
24/7 short-stay stabilization unit in converted hotel dining room, showing fully reclinable chairs for patient care
This “bedded outpatient” unit manages over-intoxication (both over-sedation and over-stimulation/over-amping), withdrawal, and complications of substance use (e.g., abscesses, HIV risk, psychosis). Patients are assigned to a recliner chair and may receive care for up to 24 h per treatment episode.
The clinical programs are staffed 24/7 with a nurse practitioner, two registered nurses, a registration clerk, and a harm reduction specialist. A secure medication dispensing cabinet allows for rapid administration of medications ordered through the electronic medical record, including methadone for opioid withdrawal management under the provisions of the 72-h rule [23] A case manager offers referral to ongoing treatment 7 days per week.
When patients present to one of the clinical programs with opioid withdrawal they often receive methadone treatment for their symptoms. Initiation of methadone treatment reflects emergency treatment of opioid withdrawal under the federal “72 h rule,” (see Fig. 1). Patients are eligible to return to the Roundhouse for additional methadone treatment of withdrawal symptoms for up to 72 h while being referred to ongoing care, most commonly at an OTP for long-term methadone treatment. Linkage refers to referral to an OTP that agrees to accept them for next day dosing and enrollment for ongoing care. Other patients requested referral to an inpatient medically managed withdrawal program (“detox”) or were referred for inpatient care of an acute medical condition.
Data sourcesHousing data were abstracted from data collection logs that were maintained prospectively by the case management team using a standardized data collection tool. Case managers updated the file after client contacts, which were scheduled to occur at least once weekly, and more frequently based on client need.
Clinical program and patient demographic data were abstracted from a standardized enterprise clinical data warehouse which is derived from the electronic health record. Monthly queries assessing medication orders, clinical encounter data and encounter diagnoses using BMC’s SUD and behavioral health ICD-10 code-sets (2-year diagnosis history) generated outcomes reported in this study. Methadone order data were obtained directly from Medication Administration Reports from the electronic health record, Epic (Epic Healthcare Systems, Verona, WI), and OTP referral and acceptance data were collected in flat files maintained by RH nursing staff, which were quality checked with chart review by program medical directors.
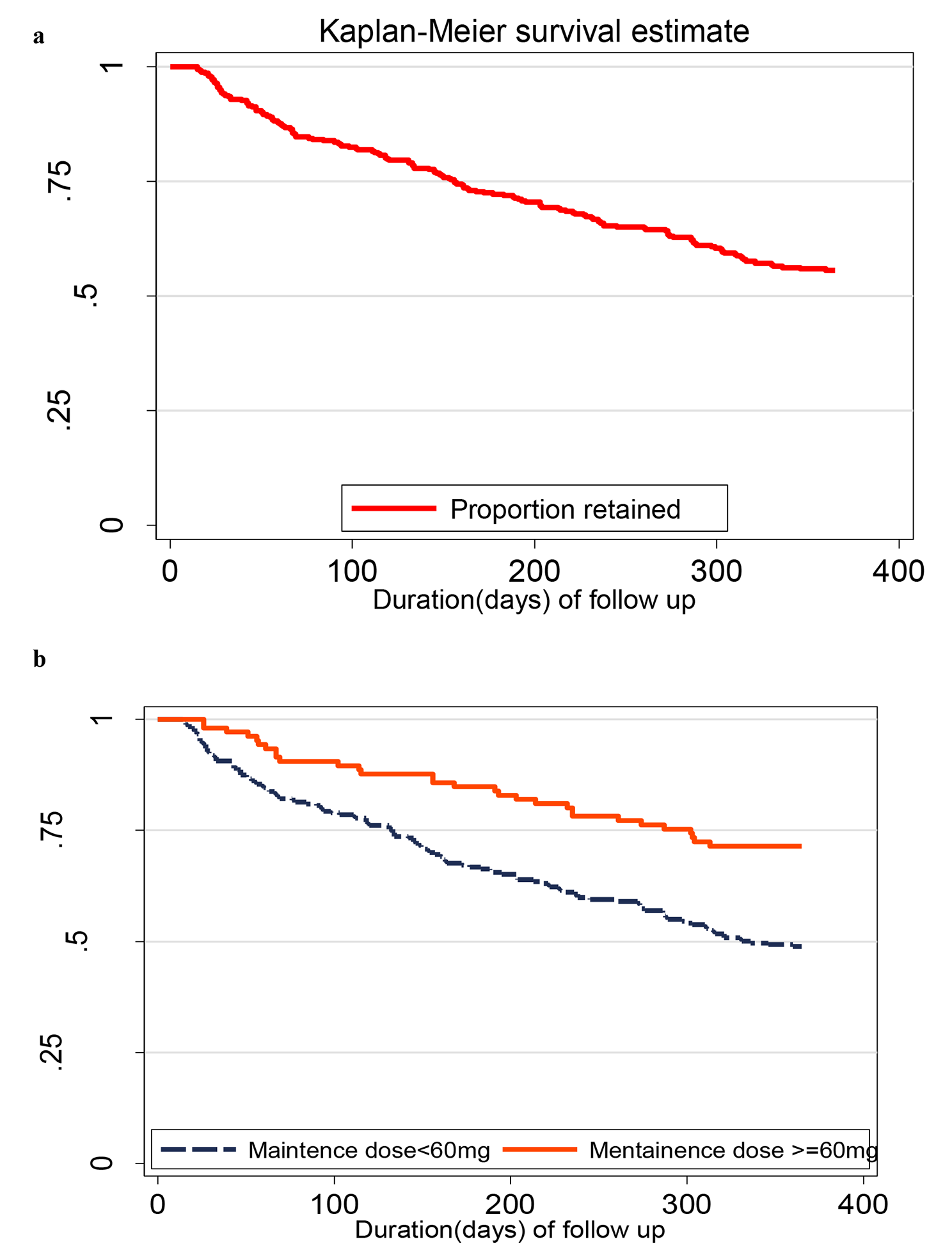
OutcomesHousing outcomes are reported for residents who entered RH housing during the 12-month period February 1, 2022–January 31 2023. Housing program key performance indicators include retention in transitional housing, transition to permanent housing, engagement in SUD treatment, and engagement in case management. Housing program residents were considered ‘retained’ if they resided in the RH for at least 3 months or transitioned to permanent supportive housing or a residential SUD treatment program. When calculating housing retention rates, residents who were incarcerated (n = 4) were excluded from the measure, as were those admitted to the RH less than 3 months before the end of the study period (n = 6).
Clinical program outcomes are reported for all patients who had an encounter at the RH clinical programs between February 1, 2022–January 31, 2023. In addition, separate clinical outcomes are reported for the subset of RH residents who also utilized RH clinical services.
Clinical program key performance indicators include visit volume and initiation on methadone for opioid use disorder. Due to historical data capture of Hispanic ethnicity as a race in our system, patients were considered Hispanic if they had Hispanic as a documented race or ethnicity. Race is presented as non-Hispanic White, non-Hispanic Black, Hispanic, and other race.
Statistical methodsDescriptive statistics were used to summarize key outcomes. Not all residents will have had equal time to receive case management services, such as referral to permanent supportive housing, so summary statistics are provided for length of stay of housing program residents.
留言 (0)