
記住我


This study will employ a mixed-methods technique with an explanatory sequential approach for data collection and analysis. Grounded in pragmatic principles and logic, the mixed-methods paradigm combines quantitative and qualitative methodologies to provide a comprehensive understanding of the research questions. In this methodology, the researcher first gathers quantitative data to identify patterns or trends requiring further exploration. Subsequently, qualitative data are collected from individuals who can offer insights to enhance the understanding and interpretation of the quantitative findings [84]. According to this paradigm, merging qualitative and quantitative methods results in a deeper comprehension of the issue [85, 86].
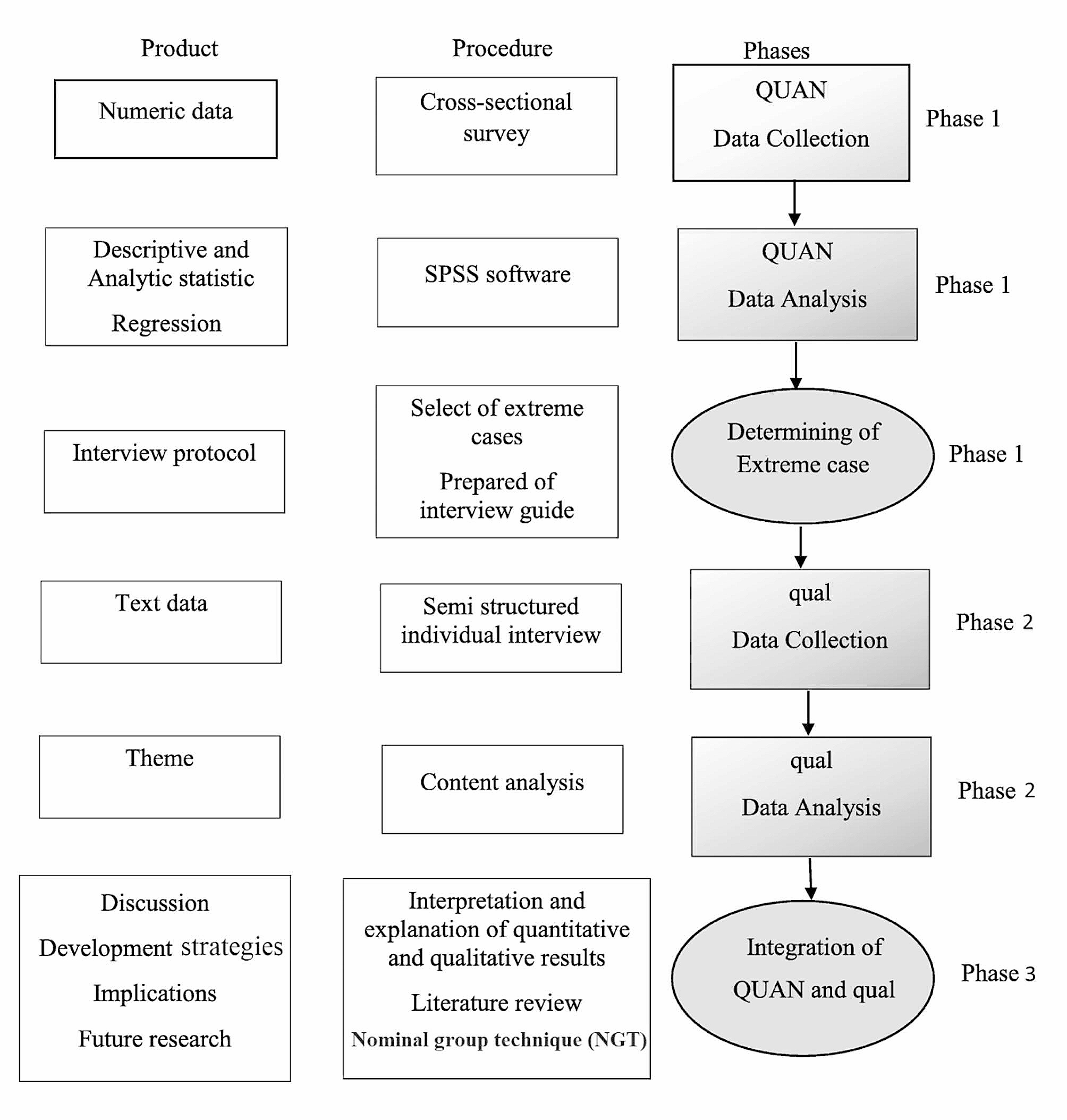
This study will be conducted in three phases. The first phase will be a quantitative study, during which, quantitative data will be gathered. The second phase of this project will be a more detailed exploratory qualitative study of participants’ experiences regarding SUD-related stigma toward and discrimination against people who use drugs at PATCs. At the end of the second phase, the qualitative and quantitative findings will be integrated. The third phase of the study will involve the development of evidence-based and culturally sensitive strategies based on a literature review, the results of Phases 1 and 2, and experts’ opinions using the nominal group technique (NGT) (Fig. 1). Full explanations of each part of the study are provided below.
Fig. 1 Phase 1: quantitative study
Phase 1: quantitative studyThe quantitative phase will be a descriptive-analytic cross-sectional study conducted among Iranian people with SUDs living in Mazandaran, Iran. In this phase, we will assess perceived stigma experiences and their relationship with social distance, perceived dangerousness, experts’ discrimination or acceptance, and sociodemographic characteristics among the participants. The target population will consist of people who are referred to PATCs in Mazandaran, Iran. The Perceived Stigma of Addiction Scale (PSAS), Health Professionals’ Attitude Towards Substance Abusers Scale (HPA-SAS), and Social Distance Scale (SDS) will be used. These scales will be validated for use among Iranian people.
Sample size and sampling methodThere is no shortage of research on stigma toward and discrimination against people with SUDs at PATCs and other health-care settings in Iran. Therefore, the sample size is calculated based on Matsumoto’s study [87]. Following Matsumoto et al. [87], the calculated sample size is 240, based on the largest standard deviation related to the sub dimension of stigma (SD = 12.39), with a precision (d) of 0.05 around the mean (m = 35.01), and α = 0.05. In most cases, the design effect’s numerical value is about 1.5–2. In this study, we will apply 1.5, and the final sample size will be increased to 360 substance users, based on cluster sampling.
For this project, fifteen PATCs in Mazandaran will be selected. A cluster sampling method will be employed, with each cluster comprising a comparable number of respondents. Mazandaran will be divided into three areas (west, central, and east). All PATCs within these areas will be enumerated, and five PATCs will be randomly chosen from each area. Individuals with SUDs who are referred to the PATCs will be invited to participate in the project.
The participants will be offered comprehensive explanations of the goals and methods of the research. The sociodemographic questions, the PSAS, HPA-SAS, and SDS will be administered in a “quiet setting” [questionnaire will be presented while maintaining patient privacy] by a research group member and then collected in person. The investigator will fill out the scales to ensure that the same data collection method is used for all individuals. Informed consent will be obtained from the individuals prior to the data collection.
Inclusion criteriaIndividuals will be eligible for the current project if they are adults (aged 20 years or older), reside in Mazandaran province, have a history of any kind of substance use, and have no severe mental difficulties that prevent them from answering the items in the questionnaires.
Exclusion criteriaThe exclusion criteria for participants will be: having a mental disability, having psychiatry history like active bipolar disease, depression with psychosis, or schizophrenia, being deaf or mute, showing unwillingness to continue participating in the study, and not fully completing the questionnaires.
Questionnaires and data collectionQuantitative data will be collected utilizing sociodemographic variables and the PSAS, HPA-SAS, and SDS scales. The sociodemographic section will include questions on age, gender, occupation, duration of employment, and education. The PSAS comprises eight items to measure the perceived stigma towards individuals with substance use disorders. Initially developed and validated among patients undergoing treatment for substance use–related issues in the United States [88]. he items were adapted from a study conducted by Link and colleagues on perceived discrimination-devaluation processes, Content validity was established through review by stigma professionals in the substance use field the PSAS was related to adopted shame, self-concealment, adopted stigma, and depression [89]. The PSAS employs a four-point Likert scale ranging from “strongly disagree” to “strongly agree” for participants to rate their agreement or disagreement with each item. Scores range from 8 to 32, with higher scores indicating greater perceived stigma. The PSAS has demonstrated good reliability, with a Cronbach’s alpha of 0.71 and a reliability coefficient of 0.79 based on the test-retest method in American society [88]. In an Iranian study, the reliability of the PSAS was found to be 0.85, with a test-retest correlation coefficient of 0.81 [90].
The HPA-SAS consists of 10 items, with questions addressing the attitudes and/or views of health professionals toward people with SUD, their knowledge of addiction, and their training in substance use. The constructs of attitudes will focus on discrimination and acceptance towards people who use drugs. The HPA-SAS was developed utilizing a Likert scale format, with each item offering four response options: (1) strongly disagree (2), disagree (3), agree, and (4) strongly agree, resulting in total scores ranging from 10 to 40. The validity and reliability of the HPA-SAS were established through research conducted by a team of psychological counseling and medical care professionals. The overall Cronbach’s alpha of the original HPA-SAS has been reported as 0.79 [91]. In this study, the validity and reliability of the questionnaire were assessed prior to data collection with a sample of Iranian people who use drugs. The overall Cronbach’s alpha of the HPA-SAS was found to be 0.76, and the test–retest correlation coefficient of this scale was 0.74.
The seven-item SDS, which was created by Bogardus et al. (1925) [92] and then modified by Link et al. (1987) [89], measures the social distance that interviewees wish to keep toward a person with a particular condition (diverse social, ethnic, or racial backgrounds). This scale focuses on respondents’ willingness to engage in a relationship with someone who is dependent on illegal substances. In particular, it measures people’s willingness to take part in a variety of social contacts with a particular group. The SDS consists of seven items presented as multiple-choice questions, which assess social distance by probing the respondent’s willingness to engage in various social interactions with stigmatized individuals: These interactions include scenarios such as being a sub-lessee, neighbor, co-worker, spouse of a family member, caretaker of one’s child, and member of the same social group. Participants will be asked to rate their level of willingness or unwillingness for each item using a four-point Likert scale with the following options: (0) definitely willing [1], willing [2], unwilling, and [3] definitely unwilling. The total score ranges from 0 to 21; scores higher than the mean identify higher social distance. The overall Cronbach’s alpha of the original SDS is 0.75 [89]. The Iranian version of the SDS has found to have a Cronbach’s alpha value of 0.92. The test–retest reliability coefficient for the SDS was 0.89, and the content validity coefficient was 0.75 [90].
Data analysisThe data from the first phase of the study will be analyzed using SPSS Statistics Version 26.0 for Windows (IBM Inc., Armonk, NY, USA). In the cross-sectional phase, descriptive statistics will be applied to describe the sociodemographic factors and perceived stigma of addiction, experts’ attitudes toward people with SUD, and social distance. Univariate analytical statistics will be used to test the correlation between the sociodemographic variables and perceived stigma, experts’ attitudes toward people with SUD, and social distance. Variables with a correlation of p < 0.1 in the univariate analysis will be included in the multivariable logistic model. All statistical tests will be two-tailed, and a p-value < 0.05 will be considered statistically significant. To ensure data quality during this phase of the study, measures such as double data entry and range checks for data values will be implemented.
Phase 2: qualitative studyIn Phase 2, an exploratory qualitative study will be conducted utilizing a conventional content analysis method to explore the experiences of people who use drugs regarding stigma and discrimination stemming from the community, health-care centers, or PATCs as a result of drug use. Additionally, this phase will aim to gain insight into healthcare providers’ perspectives on stigma against people who use drugs in greater detail. Given the objectives of the project’s qualitative phase, employing this method will enable the investigator to gain a comprehensive understanding of the situation, facilitating the clarification of the impact of stigma and discrimination on Iranian people who use drugs at PATCs.
Participants and sampling methodA purposive sampling approach will be used in the second phase of the study. The target population will consist of two groups of people, namely, those who have experienced drug use and staff members at PATCs. The first group of participants (people who use drugs) will be selected from those willing to participate in the quantitative phase of the study and will be based on the mean total score of the stigma experience, which will be collected in Phase 1 of the study. People with 10% upper and lower stigma experience scores will be selected as extreme cases, and will be retained for the next phase. We will seek to interview people with either a stigma or discrimination experience in order to collect more comprehensive information about their stigma experiences and its related factors. Efforts will be made to have variety in terms of gender, level of education, religion, age, socioeconomic situation, and the use of different types of drugs.
The second group of participants will consist of health-care workers and providers at PATCs. This sample will include agents from (i) PATC management, (ii) clinical and medical teams, (iii) health-care program teams and (iv)others according to the setting (e.g., finance). Health-care workers will be enlisted using purposive sampling methods. Four of them will be contacted through education programs with a specific focus on staff involved in drug treatment. The retained persons will be invited to register, and a member of the research team will be in touch to schedule an interview. Health-care workers in specific treatment centers will also receive direct invitations from the investigation team.
Data analysis will commence after the first interview, focusing on elucidating the intricacies and interactions among key concepts and categories derived from the exploration of the primary data. Consequently, the selection of participants will persist until theoretical saturation is achieved, ensuring a comprehensive understanding of the relationships between the study concepts and components [93]. In the current study, sampling will continue until the investigator determines that no further data can be garnered through data analysis and coding, signifying theoretical saturation. However, it is recommended by experts that a minimum of 12 participants be interviewed for a qualitative study to ensure a robust and comprehensive analysis [94].
Data collectionData will be collected by two methods: in-depth interviews with individuals with SUDs and focus group discussions with PATC staff members.
Semi-structured, in-depth interviewsIndividual, in-depth, semi-structured interviews featuring open-ended questions will be employed to gather data. These interviews will focus on exploring participants’ perspectives and experiences related to stigma and discrimination against individuals with (SUDs within healthcare settings. The target group for this part of the study will consist of people who use drugs who have been referred to PATCs in Mazandaran, Iran. Before the qualitative phase of the study, the interview protocol questions will be prepared based on the results of the first phase of the study as well as the literature review. Interviews will be held in locations, such as clinics, where respondents will feel safe and relaxed. All individual in-depth interviews will be recorded using a digital tape recorder after the applicant’s permission. In addition to the audio recordings, the interviewer will take notes. If participants decline to be audio-recorded, only notes will be employed for data gathering. Furthermore, non-verbal cues, such as facial expressions, tone of voice, and the respondents’ state, will also be noted by the interviewer, together with the date and place of the interview.
All interviews will be conducted by the first author of this study, who is familiar with qualitative research methods and the topic, and who has conducted similar studies on addiction,. Participants will be encouraged to discuss their experiences related to strategies to reduce addiction-related stigma and discrimination in public addiction treatment centers. Further, they will be encouraged to discuss sociocultural and ecological components that might have had an effect on the level of using these strategies in this regard.
The interviews will be focused on the following three main questions:
How was the experience with stigma toward and discrimination in health-care settings?
What strategy and procedure have they applied to reduce and cope with stigma and discrimination in health-care settings?
How have the strategies and procedures affected their coping strategies in this regard?
Based on the responses to these questions, follow-up questions will be asked. After each question, participants will be invited to explain more thoroughly their answer, by probing questions such as “What do you mean?” or “can you explain this more”.
Interviews will be performed during a single meeting with each participant and is estimated to last between 40 and 60 min, although this can differ slightly based on the experiences of each participant. The investigator will start with explaining the significance of the study in order to gain their confidence. All interview questions will be reviewed after the first interview, and all interviews will be taped. Data collection will be continued until saturation is reached.
Focus group discussionsFollowing semi-structured interviews, the principal researcher (first author), who is an expert in qualitative studies, an expert in qualitative studies, will conduct focus group discussions with staff members at Patients with Substance Use Disorders Treatment Centers (PATCs), which comprise the second target group of this phase of the study. These focus group discussions aim to validate the emerging themes from the individual interviews and gain deeper insights into the identified themes. The focus group discussions will be guided by the two main research questions: (i) What is providers’ understanding of stigma towards and discrimination against persons with SUDs? and [2] What are the providers’ opinions regarding a response to stigma and discrimination? Furthermore, more detailed investigative questions will be incorporated, such as: What types of SUDs do your clients typically present with? Are there any other community-level factors that could influence experiences of stigma and discrimination against individuals with SUDs?
Data analysisImmediately following data collection, the coding process will be initiated, and the data will be analyzed. The main themes will be identified using a conventional content analysis method of Graneheim and Lundman [95], in which themes and subthemes are identified to reveal participants’ perceptions and experiences toward stigma and discrimination against Iranian people who use drugs at PATCs. This process will employ inductive reasoning, which introduces concepts and categories via a detailed exploration of the data by the researcher.
In Graneheim and Lundman’s method, qualitative content analysis addresses the obvious content of an interview, along with explanations of content that can be construed or added from the interview but are not obviously detailed in the transcript [95]. Further, coding classifications are derived directly from the transcription data. Without laying on preset themes or prior theoretical opinions to categorize extracted codes from interviews, the conventional content analysis method is a suitable technique for advancing coding categorizations from the raw interview transcripts.
In this method, data analysis begins with a comprehensive reading of the entire text to ensure a thorough understanding. Subsequently, the text is examined word by word to extract codes, initially identifying specific words that may encapsulate the main concepts. These texts are derived from notes documenting the initial opinions of the interviewees and the preliminary analysis conducted. Codes that are indicative of more than one main thought are tagged and then categorized based on their dissimilarities and similarities. The greatest benefit of a conventional content analysis is attaining data directly from the study without imposing preplanned and defined categories, themes, or theories. However, one problem with this kind of analysis is that it interjects with other qualitative methods (i.e., grounded theory or phenomenology). While these approaches share similarities with initial analysis, they are emphasized for their relevance to theory advancement. Additionally, they hold significance for model development. To evaluate the trustworthiness of the results in this phase of the study, four criteria —reliability, portability, credibility, and verifiability— will be employed [96]. MAXQDA software will be used for data processing.
Phase three: integration of quantitative and qualitative data and the development of strategiesIn this phase, cultural evidence-based strategies aimed at reducing stigma and discrimination associated with substance use of Iranian people at PATCs will be developed This will involve integrating insights from the literature review, the findings of the preceding study phases, and input from experts. The target group for this aspect of the study will comprise PATC experts residing in Mazandaran, Iran.
Upon completion of the second phase of the study, the quantitative and qualitative results will be merged to glean additional insights that will inform the design and implementation of appropriate strategies to mitigate stigma and discrimination against individuals with SUDs at PATCs. Three techniques can be employed to integrate the quantitative and qualitative findings: combining the data into a discussion, utilizing a matrix for combination, or employing a side-by-side display and transformation. n this study, the data will be combined into a discussion format. Some researchers often commence this approach with a section outlining the quantitative findings, followed by a section detailing the qualitative findings. Alternatively, researchers may present the quantitative findings while substantiating claims with quotes extracted from them. Another less common technique involves initially presenting the quantitative results and subsequently confirming and validating them with descriptive qualitative findings [97, 98].
To develop strategies for reducing stigma and discrimination against people who use drugs at PATCs, the research team will start with formulating guidelines after a comprehensive review of the available literature. Systematic review and interventional studies will be conducted to find approaches. The search will encompass English-language databases (including Cochrane Library, APA PsycNET, MEDLINE, Web of Science, Embase, Scopus, ProQuest) as well as Persian databases (such as Magiran, Irandoc, SID, and Barakat). No restrictions will be imposed, particularly with regard to publication dates, to ensure comprehensive coverage of relevant studies. A uniform search strategy will be applied across all databases, utilizing the intersection of three fields via the Boolean AND operator. To define search terms, the Medical Subject Headings (MeSH) dictionary will be referenced. Upon identification of relevant documents, their quality will be assessed using the GRADE approach, followed by evidence analysis. Insights gleaned from the literature review will also be incorporated. Subsequently, the recommended strategies developed will be offered to Nominal Group Technique (NGT) experts.
NGT will be applied will be employed to devise and implement effective strategies aimed at diminishing stigma and discrimination against individuals with SUDs at PATCs. NGT is a structured, group-based method utilized to achieve consensus. Participants are encouraged to independently generate viewpoints based on predetermined and organized questions facilitated by a moderator [99]. To initiate the NGT process, primary strategies will be extracted from the findings of the first and second phases of the study, in addition to insights gathered from a literature review and examination of relevant rules and regulations A meeting will then be held with the experts who must meet the inclusion criteria of being residents of Mazandaran, Iran, possessing a minimum of one year of relevant work experience, having comprehensive familiarity with Iranian culture and customs, and being employed in a clinic associated with the treatment of people who use drugs. During this meeting, specialists will be invited to share their opinions on the developed strategies in relation to the key study questions, with all ideas and suggestions being meticulously recorded. Subsequently, these suggestions will be organized and prioritized to formulate consensus-driven strategies for effectively reducing stigma and discrimination against Iranian individuals with SUDs.
Ethical approvalThe Ethics Committee of the Mazandaran University of Medical Sciences in Mazandaran, Sari, Iran, has approved the protocol for the present study [code number: IR.MAZUMS.REC.1401.192]. Informed written consent will be obtained from all participants during the quantitative and qualitative stages. Participants will be assured of the confidentiality of their data and identities. Additionally, they will be informed that they have the right to withdraw from the project at any phase of the intervention, and that their decision to refuse participation at any time will not impact or alter the quality of services provided to them.
留言 (0)