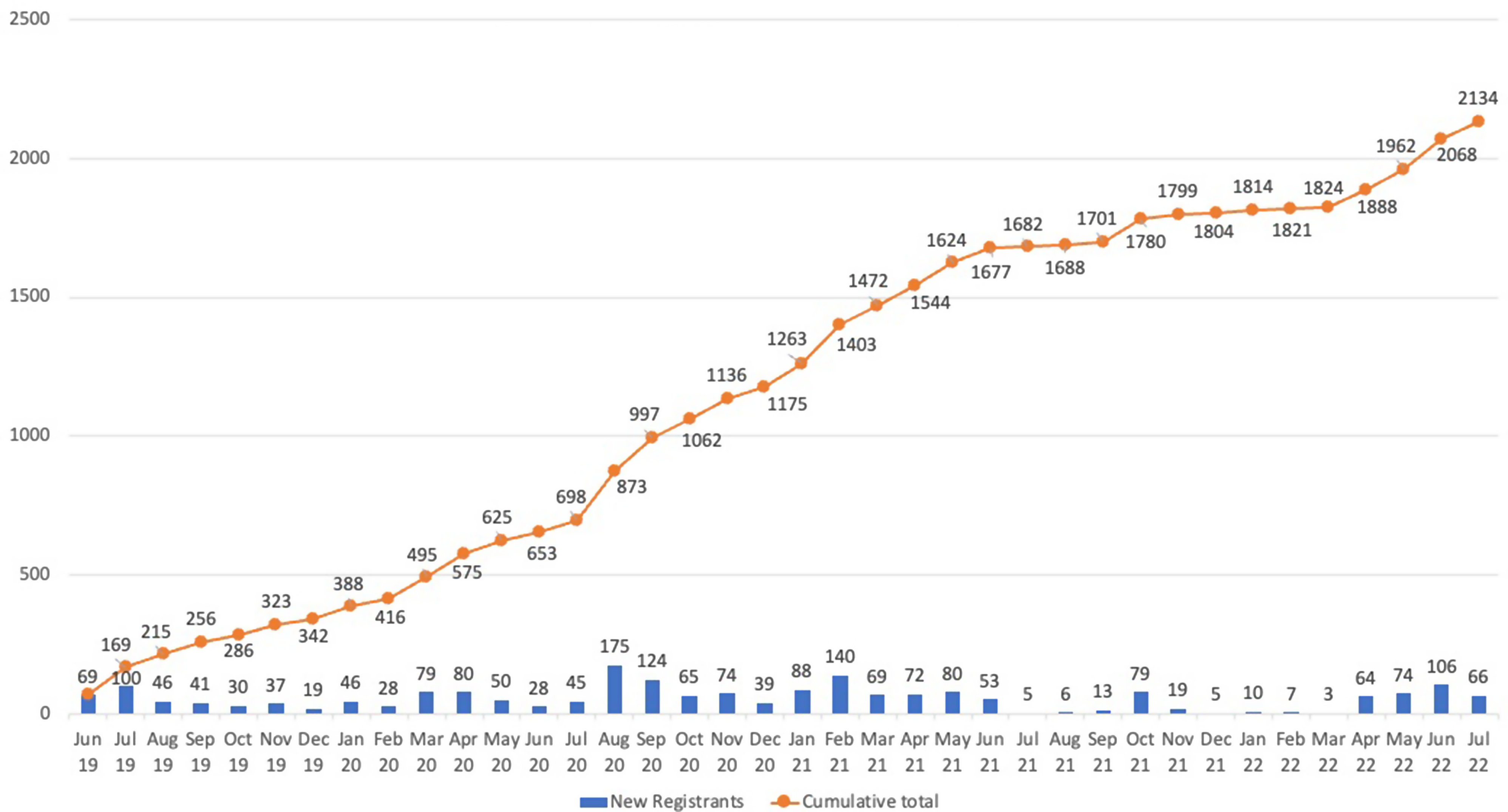
We conducted a retrospective cohort analysis of 343 people who inject opioid drugs, enrolled in the nascent MOUD programme and attained a maintenance methadone dose, during September 2020 and July 2022.
Study setting
The MOUD programme commenced in September 2020 at Butabika National Referral Mental Hospital in Uganda’s capital city, Kampala, as a learning site to inform programme scale-up. The MOUD clinic, located in the alcohol and drug unit, has a separate access entrance used by only MOUD clients, and staff. The separate entrance allows MOUD clients to access the clinic with minimal security checkpoints versus what other clients have to go through to access other services at the hospital; minimizes the chance of inpatients (under rehabilitation treatment for alcohol use and other drug-related problems) accessing illicit drugs through the MOUD clients; and improves retention on long in-patient care.
In addition to offering tertiary mental health services, Butabika National Referral Mental Hospital also provides integrated primary health care (PHC) services such as HIV, TB and STI diagnosis and treatment. This one-stop services integration model enables the hospital to offer a person-centered delivery model.
Participants
The Uganda Harm Reduction Network (UHRN), a community-based organisation, provided information to PWID community members on the availability of MOUD services and referred interested and eligible participants to the clinic for enrollment. The screening process involved establishing the participant’s opioid use disorder (OUD) status. The diagnosis of OUD was made based on the Diagnostic and Statistical Manual of Mental Disorders [19]. The screening/preparation process also involved establishing the participant’s interest in enrolling in the programme; education on harm reduction; social support; determining the acceptability of MOUD; baseline assessment of clinical and mental health status, HIV sero-status, hepatitis C status, urine toxicology, and Clinical Opiate Withdrawal Scale (COWS) score at enrolment [20, 21]; and developing a treatment plan. Participants 18 years and above with confirmed opioid use disorder, a history of injecting drug use in the last 3 months, were willing to adhere to the clinic dos and don’ts, and provided written consent to enroll on MOUD were eligible and accepted in the study. Participants with coexisting severe alcohol use disorder, severe liver disease or chronic pain were referred for appropriate management. To understand the relationship between the maintenance methadone dose and retention, we analyzed only participants who attained stable dose at 14 days. The 14-day time point is important because, at this point, unlike during the induction phase, OUD patients are stable and are expected to be receiving a maintenance dose with full benefits of methadone, where the psychosocial problems inherent in opiate addiction are relieved upon the methadone maintenance. Studies by Kling MA et al. (2000) and Gavin Bart (2012 separately demonstrated that during stabilization, methadone binds to approximately 30% of mu-opioid receptors, thereby allowing the remaining receptors to carry out their typical physiological functions in pain, reward, and mood modulation [9, 22].
The intervention
The medication used for MOUD is oral methadone provided as a daily observed dose. Each day participants were received by a peer at the clinic reception for triage, to receive daily methadone dose, visit a counsellor/psychologist or clinician. The decision of what services a participant received was guided by the presenting complaints, including the need for clinical review, dose review, PrEP, or other medication refills and summarised in the treatment plan.
Induction and follow-up and termination
The MOUD initiation involved starting patients on a minimum safe dose of methadone that reduces craving or withdrawal symptoms, carefully increasing this dose to reach a maintenance dose over a period of 14 days. Participants with signs of opioid intoxication or sedation had to abstain from drug use for at least six hours before induction. The initial induction dose was 10 mg methadone, adjusted upward on a 5 mg scale until stabilization was reached. The dose was adjusted upward or downward based on participant needs, preferences, and clinic attendance. For example, participants who missed more than three consecutive days of clinic attendance, had their methadone dose reduced based on clinical assessment. The participants came to the clinic daily for observed methadone dosing. The participants were also required to visit the clinician and or counsellor every three months for physical, mental, social, and or treatment plan review. Participants were required to attend weekly group education sessions at both the MOUD clinic and the referring community drop-in-centre. Counsellors and peers provided individual and group counselling, education sessions, and psychosocial support services. Peers used their lived experiences with drug use to effectively deliver on their role of counselling and educating their clients and communities.
Cessation and management of missed doses
Close dose monitoring for treatment compliance was performed using an automated methadone dispenser that provided a daily print-out list of participants who missed their doses. Because a clinically significant loss of tolerance to opioids may occur within as little as three days without methadone, the participant’s dose was adjusted if they missed three or more consecutive doses and rapidly increased once the response to the lower dose was assessed.
Participants were supported to voluntarily terminate their participation through counselling and a stepwise down titration of methadone, and this was viewed as self-cessation. Participants who violated the programme conditions(as described in the consent form) were involuntarily terminated. A participant was declared not retained if they missed the methadone dose for 30 consecutive doses. In this evaluation, participants who returned after being declared not retained, underwent medical and psychosocial assessment and were advised to restart methadone on meeting the enrollment criteria, as a new participant.
Measurements
Baseline variables recorded during enrollment included sex, age, housing status (assigned as stable or unstable based on whether the participant had a place of abode, easy to locate by the peer and had stayed in the area for at least one month and was not planning to shift to a place outside MUOD programme catchment areas in the next three months). Other variables included distance between residence and MOUD, alcohol use based on audit tool [23], imprisonment during the previous 3 months, HIV status assessed following the Uganda national testing algorithm, mental illness and COWS score. At follow-up visits, any change in a participant’s residence was recorded. The daily dose of methadone was recorded using a Meta-measure dispenser [24]. Urine drug screening (UDS) using enzyme immune assay based rapid test strips, was done at enrollment and randomly during follow-up to guide the tailoring of individualized intervention toward relapse prevention.
In this evaluation, the main outcome, one-year retention, was determined by collecting data on each participant who received methadone from the MOUD clinic reached maintenance dose at 14 days, and followed for 12 months.
Data management
Data extraction followed the data management protocols at the clinic. For methadone daily dosing, data were electronically extracted from the meta-measure system by the pharmacist. The MOUD clinic staff trained on the protocol, conducted a participant chart review, and extracted data on the demographic, social, clinical and psychiatric characteristics. The data was reviewed by the first and second author before it was keyed into an open data kit database. The different data sets were saved in a comma-separated version (CSV) delimited format and imported into Stata version. 14.2 (College Station, Texas) for cleaning and analysis.
Data analysis
The analysis includes participants who reached 14 days of follow-up, a point after which a participant was presumed to be at a stable methadone maintenance dose (the primary independent variable examined. Baseline data were summarised using medians and interquartile ranges for numerical variables and proportions for categorical variables. For each participant, the median daily methadone dose was computed for all doses taken after the initial 14 days when a participant was on a maintenance dose. The median dose was a better estimate measure of methadone exposure compared to the mean doses because methadone dose data were not normally distributed.
The median dose was then categorized as a low dose equivalent to less than 60 mg, and a high dose equivalent to 60 mg and above [11, 25]. The variations in participants’ characteristics based on the main predictor dose of methadone (low versus high dose) were assessed using the Pearson Chi square test. The number of days from the date of enrollment until the date the participant was lost from care, died, discharged, or until the end of follow-up was taken to calculate retention duration in treatment using the Kaplan‒Meier method. The life table method was used to calculate the cumulative retention rate. The clients discharged from the programme after successful cessation of drug injection or who remained in the programme 12 months from the enrollment date were considered retained. However, participants who died or were lost from care were classified as failing(non-retention). Participants enrolled in MOUD who dropped out during the first 14 days were excluded from further analysis because these had not attained the optimal maintenance dose, the main predictor in this analysis. Using Cox’s proportional hazards model, we determined the factors associated with retention on MOUD. Independent variables were enrolled in bivariate analyses, and variables significantly associated with retention (p-value < 0.1) and or known to have clinical association with retention in the MOUD programme, were included in the Cox regression multivariate analyses. Hazard ratios (HRs) and 95% confidence intervals are estimated. All independent variables were transformed into categorical variables. All analyses were performed using Stata version. 14.2 (College Station, Texas).








留言 (0)