
記住我









Thyroid gland disorders are of global public health concern and are regarded the most common type of endocrine diseases after diabetes mellitus, accounting for 30–40% of glandular disorders [1]. Endemic goiter which is characterized by thyroid gland enlargement with or without affecting its function tops the list of thyroid gland disorders [2]. This problem disproportionately affects the poor. According to Qasim [3], there is a direct association between societal socioeconomic status, disease occurrence, and surgical outcomes that are dependent on medical care factors. As such, low-resourced countries have high prevalence of goiter, for instance up to 60.2% in Uganda [4], due to consumption of iodine-deficient meals or foods which interfere with iodine uptake. Furthermore, poorer individuals have impeded access to specialized health care and therefore present with advanced disease associated with compressive symptoms such as acute respiratory distress in addition to painful swallowing, hyperactivity of the gland (hyperthyroidism), and poor quality of life [4,5,6].
Thyroid surgery conventionally known as thyroidectomy is the principal treatment for symptomatic goiters that do not respond to medical treatment and remains among the most commonly performed surgical operations [6]. The operation is typically performed when the level of hormones from the gland which reflect its functionality has been normalized, hence the term euthyroidectomy.
Over time, various surgical approaches and anesthetic techniques have evolved to enable removal of a diseased thyroid gland. Historically, euthyroidectomy was associated with numerous post-operative complications that the first reported thyroid surgeon was jailed after the death of his patient in 1646 [7]. Albert Theodor Billroth was the first surgeon to popularize thyroid surgery, which encompassed primarily drainage of the thyroid cysts, although with concerns of post-operative pain and high levels of recurrence [7]. Subsequently, thyroidectomy was for years conventionally performed under regional local anesthesia (LA) resulting in loss of sensation and pain in a localized part of the body [8,9,10] with some series reporting favorable outcomes on over 20,000 patients as of 1990 [9, 11].
Following the advancement of general anesthesia (GA) techniques in which a state of unconsciousness is induced with complete absence of pain and reflexes, the number of thyroidectomies performed under GA increased and ultimately, GA became the preferred method under which thyroidectomy is carried out. In the current surgical practice, majority of surgeons prefer to perform thyroidectomy under GA which offers the advantage of pain-free surgery to the patient, thus reducing their anxiety and enabling a more relaxed operating room environment for the surgeon [8, 9].
Conversely, preference to GA is not without limitations. First, the longer recovery time from anesthesia results in prolonged hospitalization, delayed return to work, reduced patient turnover, and ultimately contributes to the unmet need for surgery. This culminates in patients presenting much later in life with huge goiters that have both local and systemic complications, compromising their general well-being, quality of life, and economic productivity. Secondly, in low-income settings with limited infrastructural and human resources, GA is comparatively undesirable due to concerns related to post-operative care and monitoring after the surgery such as lack of skilled staff and equipped intensive care units [6]. For instance, despite efforts from donor funding and south-west institutional collaborations, Uganda with its 45 million population boosts with only 100 qualified anesthesia providers (fewer than 0.05 anesthesia providers per 100,000 population) as opposed to high-income settings such as the UK with over 18 per 100,000 population [12]. Therefore, performing thyroidectomy under LA would offer the advantage of the anesthesia being administered by the surgeons themselves without putting much strain on the weak health systems.
Henceforth due to drawbacks of GA, in the last two decades, there has been an increase in the number of thyroidectomies performed under regional/LA combined with monitored anesthesia care [11, 13]. These numbers have even increased further with the development of minimally invasive thyroidectomy particularly in short-stay settings [9] and now, a few surgeons in the western world are currently doing thyroidectomies exclusively under LA [8].
Previous studies comparing euthyroidectomy under LA versus GA have shown mixed findings with regard to the benefits and post-operative outcomes. Other than overcoming the need to book for intensive care space and an anesthesiologist [14], which most patients in low-income countries cannot afford in the case of thyroidectomy under GA [15], LA has been associated with less post-operative pain, costs, hospital stay duration, post-operative nausea, vomiting, throat discomfort, and voice changes [9, 16, 17]. According to research in Nigeria [13], India [8], and USA [16], complications such as hematoma, surgical site infection, and colloid occur in less than 4% of cases of thyroidectomy performed under LA. In a randomized controlled study in Germany [9], the occurrences of post-operative complications (pain, nausea, vomiting, throat discomfort, painful swallowing, voice change, and difficulty in breathing were less in the group of patients who underwent thyroidectomy under LA as compared with those under GA in contrast to the prospective study in Uganda [18]. According to the USA [16] and Ugandan [18] studies, GA is also more associated with persistent hypothyroidism although the Kenyan cross-sectional review showed no difference[11].
In terms of cost, it has been arguably stated that performing thyroidectomy under LA might require additional training and capacity building in endocrine surgery which has cost implications, though comparatively similar costs would be incurred on supplies, critical care, and longer hospital stay [19, 20] more so in the error of COVID-19 where GA would increase in-patient risks. Cost of procedures is one of the limiting factors to access health care, and therefore, all measures should be taken to minimize the cost at which the surgical services are provided. A study done by Budhathoki et al. [20] in Nepal found out that the overall cost for thyroidectomy was less when done under LA as compared to when it is done under GA. The authors found that the cost of procedure included operation charge, material cost, medicines, and general ward bed charges. The mean cost in the participants that underwent thyroidectomy under GA was US $107.85 as compared to those under LA (US $65) [20]. Researchers Mamede and Raful in Brazil [19] found that the total cost of thyroidectomy was R$ 203.20 under GA compared to R$ 87.40 under LA. However, the significant difference in cost was only noticed in cost of treatment (drugs) with no significant statistical difference in the cost of hospital daily fees. In an Indian study by Shukla et al. [21], the mean cost incurred on patient from admission till discharge was Rs. 2189.32 for thyroidectomy under LA group versus Rs. 5520.00 in GA group. Such cost-effective studies are necessary in East Africa particularly in Uganda where there are budgetary constraints attached to health care, limited insurance coverage with most of the cost being paid out of pocket.
Further, in terms of patients’ level of satisfaction, which is a key patient-centered outcome, existing research in USA [16], Brazil [19], and Nepal [20] have shown no significant statistical difference in patients satisfaction for thyroidectomy done under LA versus GA and their participants would recommend to others to use either of the methods. In fact, a recent prospective comparative study in Nepal showed that the mean post-operative pain score using Likert scale was actually higher in LA versus GA group [20]. However, in East Africa where goiter is endemic, there have been no robust studies to compare the two anesthetic techniques in a randomized control setting. A Kenyan showed no difference between LA versus GA in terms of duration of surgery, operative complications, or length of facility stay [11]. Notably, the study had a smaller sample size of only 7 participants whose effect size could have limited the difference from being observed given the low incidence of such complications.
Study rationaleAccording to Hisham and Aina [22], the prejudice to what technique works for the system resources is constrained by fear, doubt, and disbelief in the context of diverse cultures as to what constitutes safety, cost containment, and patient satisfaction. In addition, high level of evidence is pre-requisite to clinical application of research findings [23]. Recently, Schmidtke et al. have documented how lack of validation trials and complementary studies contribute to a huge gap between surgical research and clinical practice [23]. In this regard, until 19 March 2023, to the best of the authors’ knowledge, there are no systematic reviews and meta-analyses conducted to consolidate findings on this subject. Moreover, a majority of studies on the subject are observational and a paucity of randomized trials on the topic such as Snyder et al. [16], surgery was performed by a single surgeon with inter-operator reliability limiting the level of evidence to influence uptake into surgical practice. Validation randomized control studies are necessary to guide local medical practice particularly in low-income settings where there are competing priorities for resource allocation. To allow for local and regional comparisons, this study could inform the feasibility of using LA as a comparable alternative in the context of limited human and infrastructural resources in low-income Uganda. Most importantly, the findings will inform the applicability of either technique in surgical camp setting which is the most used avenue to address the unmet need for surgery in developing countries.
Main objectiveThe aim of this randomized control trial is to compare euthyroidectomy under LA versus GA among patients with grade 1–2 goiter in Uganda.
Specific objectivesThe specific objectives of this study are as follows:
1To compare the occurrence rates of early 30-day post-operative complications (pain, hematoma, surgical site infection) following euthyroidectomy under LA versus GA
2To compare the cost implications of euthyroidectomy under LA versus GA
3To compare the patients’ level of satisfaction for euthyroidectomy under LA versus GA
HypothesisThere is no difference in the early post-operative outcomes, cost, and patients’ satisfaction between euthyroidectomy performed under LA versus GA.
Trial designThis study will be a prospective equivalence randomized single-blind controlled trial where the outcome data collectors will be blinded about the participants’ arms. The study is designed to be implemented in accordance with the SPIRIT guidelines for clinical trial protocols [24].
Methods: participants, interventions, and outcomesStudy site and settingsThe study will be conducted in camp settings of Bulamu Health Care Organization that are performed monthly in different regions of the country (Uganda).The Bulamu Healthcare is a well-established non-government (NGO) not-for-profit organization that was formed in 2016 as a branch of Bulamu Healthcare International. The Bulamu Super camp model is a uniquely cost-effective program that provides health care to impoverished families of rural Uganda. Bulamu plays the role of “Great Organizer” and brings the different government agencies and non-profit NGOs together in these camps and provide free services to Ugandans. Bulamu provides medical, surgical, obstetric, and gynecological care, public health, ophthalmology, dental care, and imaging services. The camp typically attracts over 15,000 patients in a week, approximately 3000 per day. In 2019, a total of 1433 surgeries were performed of which 53 (4%) were thyroidectomies. Over 150 to 400 surgeries are performed per week. Through the third quarter of 2019, the organization managed 49,449 patients. Both LA and GA resources are available in these camps. All operations are performed by senior consultant surgeons assisted by surgery residents. The recruitment shall be done within 4–5 camps (Figs. 1 and 2).
Fig. 1
Conceptual framework (outcomes)
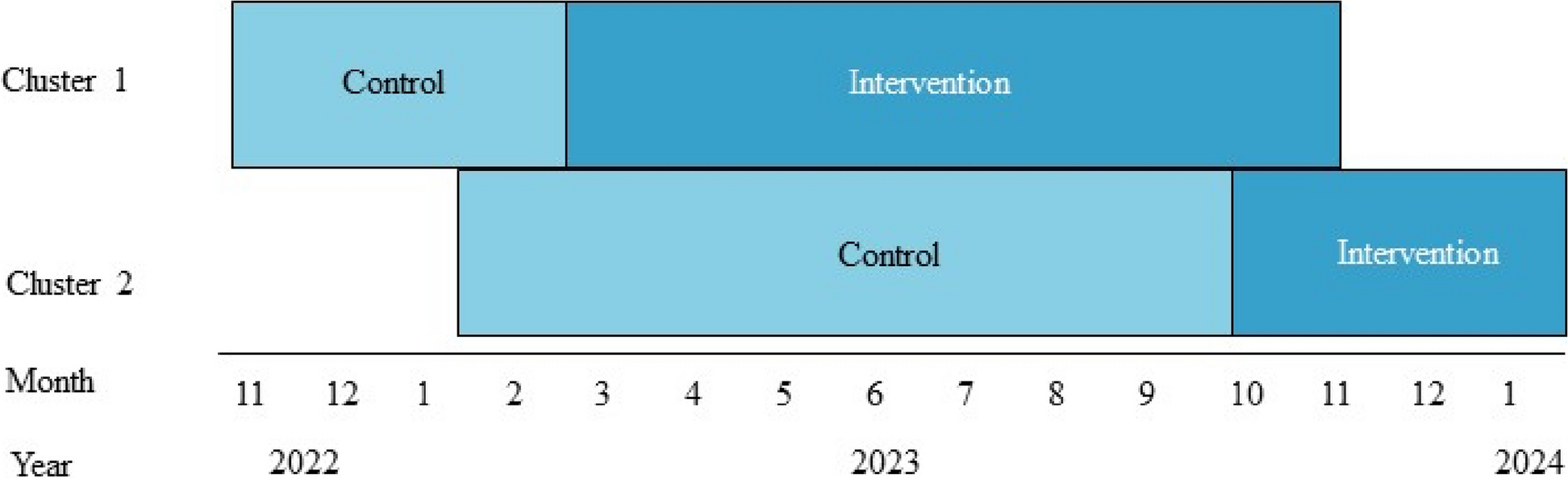
Fig. 2
Participant timeline/study period
Study periodThe study will be limited to a period from October 2022 to April 2023; thus, May 2023 will be the follow-up month for the last recruits.
Eligibility criteriaInclusion criteria of participantsPatients between 18 and 65 years with euthyroid goiter/or made euthyroid that will attend Bulamu Healthcare camps during the study period will be given equal chance to consent and participate in the study.
Exclusion criteria of participantsAll patients with factors that have been previously documented to independently impact the outcome of thyroidectomy and are known indications for GA [13], including:
1Grade 3 goiter,
2Retrosternal goiter,
3Goiters with features of infiltration to surrounding tissues such as fixity underlying structures,
4Obesity,
5Previous neck surgeries, and
6Diabetes mellitus.
Interventions: description/study procedureEligible participants based on our screening log will sign an informed consent document and undergo pre-anesthetic assessment 24 h prior surgery. This assessment will be undertaken in the designated tents used for our camp settings. All participants will be subjected to the Bulamu Healthcare fasting protocol of 6 and 2 h for solid and liquid diet respectively and will receive 1 g of intravenous ceftriaxone 60 min prior surgery. It is also a routine practice in Bulamu Healthcare to record all patients’ vital signs at 24 and 0 h prior surgery. These include but not limited to pulse rate, oxygen circulation, blood pressure, and ECG monitoring. All procedures are carried out under aseptic techniques. Following the procedure, all participants will receive intramuscular injection of diclofenac sodium 7 mg stat followed by 100 mg of oral diclofenac sodium 8 hourly for 5 days. Patients will be discharged home when they score at least 9 post anesthesia discharge scoring system [25] at the discretion of attending clinicians. Review at the 30th day will be in outpatient setting upon call by the outcome assessors. Telephone follow-up interview assessment option will be available for those who will reasonably be unable to attend an outpatient visit.
InterventionFor group L (intervention group), as adopted from a study done by Aliyu et al. [13], infiltrative local anesthesia to achieve an anterior field block in this study will involve mixing of 0.5% bupivacaine, 2% lignocaine with 1:200,000 adrenaline.
The maximum dose of bupivacaine will be 3 mg/kg and the maximum dose of 2% lignocaine with 1:200,000 adrenaline will be 7 mg/kg [13].
The total calculated dose will be made up to 60 ml using water for injection or 0.9% normal saline; 20 ml of the mixture will be used for anterior field block which extends from the supra-sternal notch below to the cricoid cartilage above to the lateral borders of sternomastoid muscles.
Ten milliliters will be given along the incision line and another 10 ml under the investing layer of the pre tracheal fascia after raising sub-platysma muscle.
The remaining 20 ml will be given at 5 ml at each of the thyroid poles to minimize discomfort during mobilization.
Patients’ position and operative field preparation will be as in surgery under GA, but during draping, patient’s mouth and nose will remain exposed to allow continued communication and spontaneous breathing.
The communication will assure the surgeon of the safety of the recurrent laryngeal nerves.
The remaining operative steps will be carried out in accordance to the standard operative texts for thyroidectomy under GA [8, 13, 17]. In brief, the steps will include (a) positioning, painting, draping, (b) skin crease-incision and sub-platysma flap, (c) incision of investing layer of deep cervical fascia, retraction of strap muscles, and or division of middle thyroid vein, (d) superior pedicle handling, (e) recurrent laryngeal nerve and parathyroid gland safeguard, (f) thyroid gland identification and inferior thyroid vessel handling, (g) thyroid bed dissection, (h) repeat steps (f-g) on the contralateral side, (i) hemostasis with or without drain placement, and (j) wound closure.
For group G (control group), euthyroidectomy under GA will be as per the routine protocol described by Aliyu et al. [13]. Not to restrict a list of drugs that might be required in emergency situations during general anesthesia, the list is left open, and costs associated will be documented for each participant.
Interventions: modificationsAdverse events and trial discontinuation for individual participantsThe participants are anticipated to experience pain discomfort and or other complications due to the surgery as the main treatment for goiter not because of the study. In addition to breach of trial protocols, too much pain during surgery using LA will result in converting to GA (cross over) and advancing to stronger analgesics other than prescribed in protocol with ultimate discontinuation of individual participant from the trial.
Interventions: adherence to intervention protocolInclusion and exclusion criteria will be strictly adhered to. The questionnaires shall be checked for completeness and accuracy of the data. The research assistants (doctors on duty) will be adequately trained and routinely supervised by the principal investigator and study supervisors to ensure correct use of data collection tools and adherence to ethical principles.
Interventions: concomitant careNo relevant concomitant care or interventions will be prohibited during the study.
Outcomes measuresThe following outcome measures were selected based on existing literature and will be reported in conformity with Zarin et al. [26].
Primary outcome measuresThe primary outcome measures will be early 30-day post-operative complications (harms), including: pain, nausea, vomiting, hematoma, transient voice changes, and surgical site infection rates.
The complications will be reported verbally to nursing or to attending physicians for evaluation and recorded on a questionnaire in accordance with MedDRA® version 4.21 standardized reporting on medical and surgical procedures. The post-operative pain will be measured based on visual analogue scale of 0–10 where 0 means no pain and 10 means the worst possible pain. The pain will be assessed at an interval of 6, 12, and 24 h and at 30 days. The mean pain scores will be compared at using Student’s t-test, assuming normal distribution; otherwise, medians will be compared using non-parametric Kruskal–Wallis rank sum test.
The nausea and vomiting will be reported to nursing or attending physicians and recorded to the questionnaire using a nausea score on a scale of 0–9 where 0 means no symptom and 9 means very severe. The symptoms will be assessed at an interval of 6, 12, and 24 h and at 30 days. The mean nausea scores will be compared using a paired Student’s t-test, assuming normal distribution; otherwise, medians will be compared using non-parametric Kruskal–Wallis rank sum test.
Complications: hematoma, transient voice changes, and surgical site infection rates will be assessed at 6, 12, and 24 h and at 30 days will be reported in accordance with the Clavien Dindo classification of surgical complications [27], where grade I represents complications that do not require any additional intervention, grade II requires pharmacological treatment but not radiological or surgical intervention for instance blood transfusion, grade III requires radiological or surgical re-intervention, e.g., neck exploration and hematoma evacuation, grade IV representing life-threatening complications with at least one organ dysfunction such as respiratory failure that requires intensive care admission. The difference in proportions will be compared using Wilcoxon sum rank test.
Secondary outcome measuresThe average procedure costs in USD and mean duration of hospital stay (number of days away from work) will be recorded based on extracts from the patients’ case files and compared between the two anesthetic techniques.
Tertiary outcome measuresThe patients’ level of satisfaction regarding the procedure and overall experience will be reported verbally to nursing and recorded on the questionnaire based on a 5-point Likert scale where a minimum score of 1 = very dissatisfied whereas a maximum score of 5 = very satisfied. In addition, their willingness to undergo a similar surgery using the same anesthetic technique will be documented as “yes” or “no” and proportions will be compared for the two groups.
Independent variablesInformation will be captured on baseline characteristics such as sex, age, comorbidities, and ASA classification.
Participant timeline (see Table 1).
Sample size estimationSample size estimation in this study assumes a null hypothesis that there is no difference in early post-operative outcomes for euthyroidectomy under LA versus GA (equivalence study). In a study that evaluated the measurement of acute post-operative outcomes amongst patients who undergo surgery, a patient acceptable symptom state, i.e., the value beyond which patients considered themselves well, was documented at 33% [28]. Based on a study at the Scott and White Memorial Hospital, in Texas, the proportion of patients who underwent euthyroidectomy under LA with no identifiable complication were 83% as opposed to 79% who underwent GA [16]. Therefore, assuming a statistical power of 80%, type 1 error of 0.05, and a threshold for equivalence in effect with a dichotomous outcome that LA is no better or worse than GA by a minimal clinically important difference of 33% in the primary outcome measures; the sample size estimation based on Cleveland Clinic sample size estimation in clinical research (https://riskcalc.org/samplesize/) [29] will be 26 for each arm (1:1 allocation), including additional 10% to cater for loss to follow-up.
RecruitmentThis prospective equivalence randomized; single-blind controlled trial protocol will be conducted among eligible participants with grade 1–2 uncomplicated euthyroid goiters. The recruitment processes will start in October 2022 and end in April 2023.
Methods: assignment to treatment armsThis study will be a parallel trial where different groups will be randomly allocated to receive different interventions concurrently during the study.
Randomization, blinding and allocation concealment and implementationPatients who meet the inclusion criteria will be assigned randomly by research assistants to either local anesthesia group (L) or general anesthesia group (G) using envelope concealment. Half of these concealed envelopes will contain letter L and the other half letter G to represent LA and GA, respectively. Permuted balanced block randomization will be performed by the study supervisor to derive a random sequence of numbers that will represent the two arms in an allocation ratio of 1:1. The random sequence numbers will be generated using a web-based software (https://www.random.org/). A set of 52 numbers will be generated beginning with a minimum of 1 and maximum of 52. The numbers will then be used to label the sealed envelopes sequentially and will be concealed to research assistants. The content of the envelope will be concealed only to be opened in the operating room for the anesthesia providers to know what anesthetic technique is to be used for the research participant.
The s
留言 (0)