Study setting
The study setting is Danish general practice. The Danish healthcare system is primarily tax-financed, and residents have free and equal access to general practice services. General practitioners (GPs) are self-employed, working on contracts for the public funder and offer services in their practices within the frames of a national agreement with Danish regional authorities that details which services are offered in general practice and how these are reimbursed. Nurses and other healthcare professionals (e.g. midwives, healthcare assistants) are frequently employed and trained to conduct independent consultations, including chronic care consultations in general practice [17]. In this paper, these healthcare professionals are referred to as “general practice staff”, while the term “healthcare professional” refers to both GPs and general practice staff. Currently, reimbursement is provided for up to seven 30-min talk therapy sessions per patient over a 12-month period. However, only sessions provided by GPs are remunerated [18].
Patients with T2D and CHD are typically offered annual chronic care consultations provided by either the GP or trained general practice staff. National and international guidelines on disease management encourage healthcare professionals to pay attention to psychological symptoms, but they do not offer specific recommendations on how to identify and manage mental health issues [11, 12]. Typically, annual chronic care consultations focus on specific diseases and lifestyles and less on mental health. When mental health issues are recognised, patients may be offered talk therapy, medication, or referrals to psychologists or psychiatrists.
A list of participating general practices can be provided upon request by the corresponding author.
Eligibility criteria
The following are the inclusion criteria:
1.
Above 18 years of age
2.
Diagnosed with T2D and/or CHD
3.
Attend annual chronic care consultations
4.
Poor mental well-being, defined as a WHO-5 Well-Being Index score < 50 points [19]
The following are the exclusion criteria:
1.
Severe mental illness (active psychosis, suicidal mental state, or dementia)
2.
Unable to understand, read, and write Danish
All general practices in the Central Denmark Region are eligible (n = 349). Participating healthcare professionals are GPs and general practice staff with experience in conducting independent consultations.
Who will take informed consent?
The healthcare professional delivering the annual chronic care consultation will deliver both oral and written information about the study and obtain informed consent from eligible participants.
Additional consent provisions for collection and use of participant data and biological specimens
No additional consent provisions are necessary and there are no ancillary studies.
InterventionsExplanation for the choice of comparators
This study aims to test the effectiveness of the Healthy Mind intervention, which is provided in addition to the existing annual chronic care consultation. Therefore, usual care is the most appropriate comparator and acts as the control group.
Intervention description
Method used for intervention development
The intervention was developed using the UK Medical Research Council framework for developing complex interventions [20]. The intervention development process consisted of two phases: the initial development phase and the feasibility testing phase. Three approaches for intervention development were applied: the evidence-and-theory-based approach, the target population-centred approach, and the implementation approach [21]. During the initial phase, intervention development was informed by literature reviews, insights from a small-scale study testing PST in the general practice setting, and by attending to the existing frames in general practice [22]. In the feasibility testing phase, perspectives from healthcare providers and patients further informed the intervention development [16]. Our programme theory was refined throughout the development phase, and the intervention was adjusted accordingly.
Problem-solving therapy (PST)
PST is a well-established psychological treatment aiming at improving the patient’s problem-solving and coping skills [23, 24]. The assumption is that a person’s problem-solving and coping skills influence whether negative life events result in psychological symptoms, such and depression and anxiety [23, 25]. The core element of PST is training of problem-solving and coping skills by following five sequential steps: (1) listing problems and choosing one to address, (2) defining the problem in question, (3) generating solutions, (4) analysing pros and cons for each solution and choosing one, and (5) planning and undertaking the implementation of the solution. The PST provider facilitates and guides the process, while the patient takes an active role in deciding which topics to address, generating solutions, and planning and undertaking the implementation of the chosen solution. This behavioural activation is considered the pivotal component of the treatment. Patients learn to cope with their problems in a rational and systematic manner, gaining empowerment through experiential learning, realising their ability to manage encountered challenges [26].
The healthy mind intervention
All patients with T2D and/or CHD attending annual chronic care consultations in general practice are screened for poor mental well-being using the WHO-5 Well-Being Index (WHO-5) [19], described in detail in “Plans for assessment and collection of outcomes ” section and in Table 1. In the intervention protocol, patients with a WHO-5 score < 50 points are offered PST provided by either the trained GP or practice staff. A booklet guiding patients through the five sequential steps of PST, facilitated by the healthcare professional, is provided. The booklet is designed by the research team based on the insights from the feasibility study [16]. Patients are offered up to seven 30-min PST sessions. In the control protocol, patients receive the usual care.
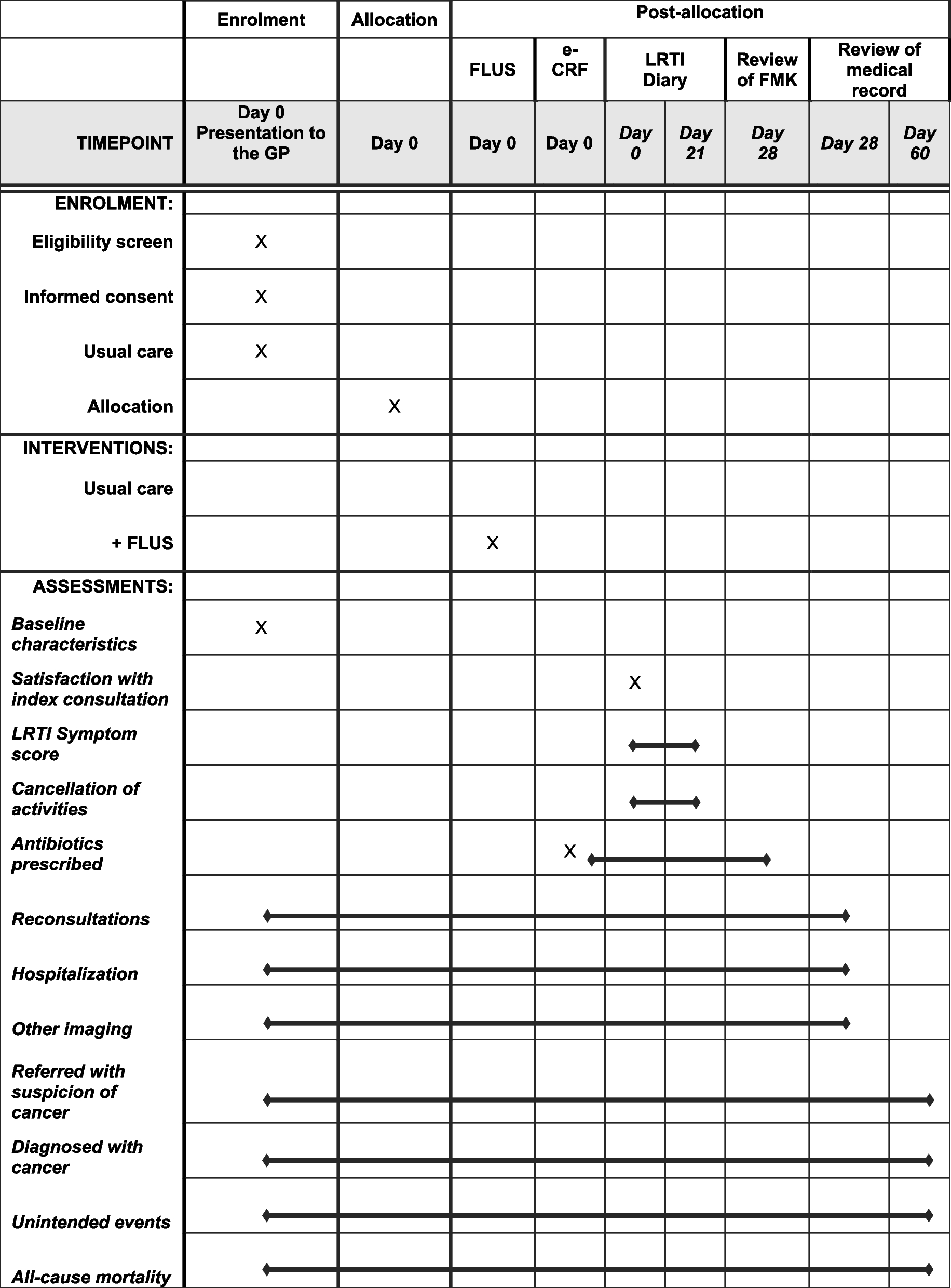
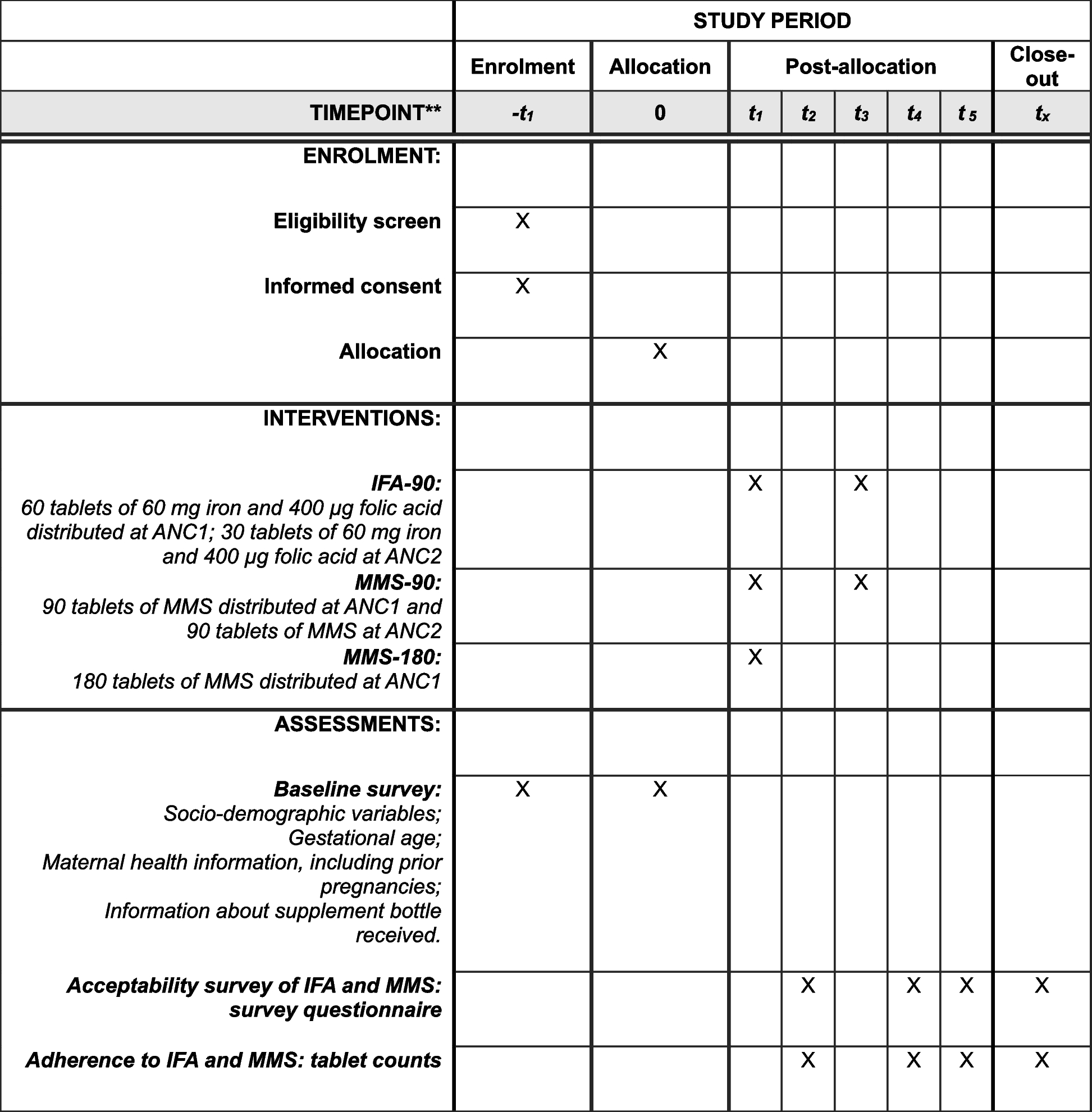
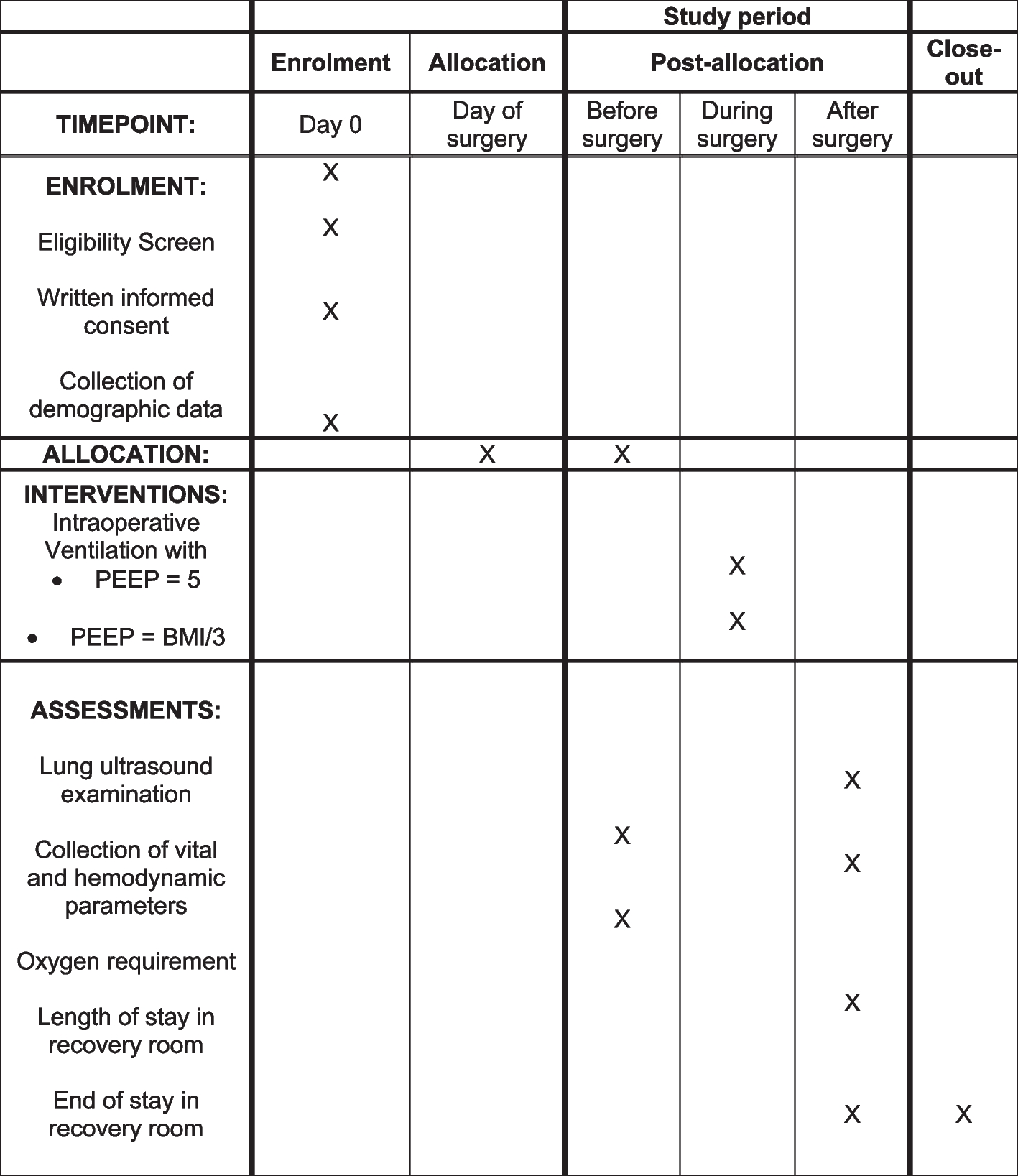
Table 1 Participant timeline
PST training course
Before transitioning to the intervention protocol, healthcare professionals attend a 2-day PST course. The course is designed on the basis of knowledge from a previous small-scale study and further refined by insights from our feasibility study [16, 22]. Healthcare professionals are encouraged to prepare for the course by watching a 30-min video that demonstrates how PST can be delivered.
The training course comprises both a theoretical component and a component focusing on implementation. Two psychologists with expertise in PST facilitate the theoretical component, which includes lectures on PST in combination with hands-on exercises, including role play, to familiarise participants with PST and ensure that they develop sufficient skills to deliver the intervention after the course. Two members of the research team facilitate the implementation component where participants will formulate specific implementation strategies tailored to their particular general practices to ensure that the intervention is properly integrated into each participating general practice.
Criteria for discontinuing or modifying allocated interventions
Patients may discontinue participation at any time. The exclusion criteria ensure that patients with severe psychopathology (psychosis, suicidal mental state, or dementia) are not invited to participate in the study. If a patient develops severe psychopathological symptoms during the study, the intervention is terminated immediately, and relevant standard treatment is initiated. If a patient withdraws from the study, data collected until the withdrawal will be part of the study.
Strategies to improve adherence to interventions
During the PST course, healthcare providers are trained to deliver the intervention with high fidelity. The booklet used during PST sessions is designed to support adherence to the methodology of PST and facilitate patient involvement.
Relevant concomitant care permitted or prohibited during the trial
All usual care is allowed in both the control and the intervention group, including medical treatment of mental illness and referral to mental health specialists, e.g., a psychologist or psychiatrist.
Provisions for post-trial care
Patients retain their usual continuous free and equal access to general practice prior to, during, and after the intervention.
Outcomes
A programme theory was created to identify anticipated mental, somatic, and process outcomes of the Healthy Mind intervention.
Primary outcome
The primary outcome is the mean change in depressive symptoms measured with the nine-item Patient Health Questionnaire (PHQ-9) from baseline to 6 and 12 months [27]. The PHQ-9 questionnaire is validated and frequently used in similar studies, facilitating comparison with previous studies. The PHQ-9 score was chosen as the primary outcome to maintain independence from the WHO-5 score, the measure used at patient inclusion. This decision was made to ensure the internal validity of the study.
Secondary outcomes
Mental health outcomes
Secondary outcomes include the mean change in general mental well-being measured with the WHO-5 questionnaire [19], the mean change in symptoms of anxiety measured by the seven-item General Anxiety Disorder questionnaire (GAD-7) [28], and, for patients with diabetes, the mean change in diabetes distress measured by the five-item Problem Areas In Diabetes Questionnaire (PAID-5) [29]. Outcome assessments will be made at baseline and after 6 and 12 months.
Somatic outcomes
Somatic outcomes include the mean change in total cholesterol levels (mmol/L), low-density lipoprotein (LDL) levels (mmol/L), and, for patients with diabetes, HbA1c (mmol/mol) from baseline to 12 months.
Process outcomes
Process outcomes include measures of implementation: fidelity, dose, reach, and mechanisms of impact: mediators and unintended consequences.
Participant timeline
The participant timeline is outlined in Table 1.
Sample size
The sample size was calculated according to the following assumptions: We expect 20% of patients with T2D and/or CHD who attend annual chronic care consultations to decline participation or be excluded from the study. We expect 15% of participating patients to report reduced mental well-being (WHO-5 score < 50 points), and 20% of patients participating in the study are expected to be lost to follow-up after 12 months. The intraclass correlation coefficient (ICC) is conservatively estimated at 0.05, reflecting a realistic expectation that a mental outcome is likely to show a larger dependence on the individual general practice than somatic outcomes, where an ICC of 0.01 is often applied. To achieve a significance level of 5% and a power of 90%, the study is required to include a total of 188 patients.
In Denmark, the size of a general practice depends on its number of practice capacities. Each general practice capacity accommodates approximately 1600 patients, with an average of 2.5 practice capacities per practice. Based on these assumptions, we need to include at least 35 practice capacities (corresponding to 14 average-size general practices) to be able to include 188 patients over a 1-year study period.
Recruitment
Recruitment of general practices
An e-mail describing the study is sent by the national health authorities to all general practices in the Central Denmark Region, and interested general practices can sign up for participation. Additionally, general practices who have previously expressed an interest in participating in mental health studies and/or research projects are contacted directly by the research team.
Recruitment of patients
Enrolment of patients relies on the general practices to systematically recruit patients at the annual chronic care consultations. The research team will take a number of initiatives to support the workflow of patient recruitment in each general practice. Prior to commencing the study, initial online meetings will be held between two members of the research team and one GP (practice owner) from each general practice to map the staff composition, current chronic care management, and workflow. Together with the GP, the research team tailors a plan for the management of patient recruitment in each individual general practice. Immediately before the study commencement, a visit is paid to each general practice to inform healthcare professionals and administrative staff about the study and facilitate the implementation of the tailored recruitment plan. One healthcare professional from each general practice is appointed the study contact person and study champion, responsible for patient recruitment and implementation of the intervention. Subsequently, videos demonstrating how to provide oral and written information to patients will be distributed to general practices. Throughout the study period, monthly newsletters are forwarded to the participating general practices with general information about the study and individual statistics regarding patient enrolment and number of conducted PST sessions during the intervention period. Patient recruitment is monitored weekly by the research team and champions are promptly contacted by e-mail, telephone, or a visit in case recruitment rates decline, to explore the underlying reasons and support further recruitment.
Assignment of interventions: allocationSequence generation
A computer-generated cluster randomisation is applied at the general practice level. Randomisation includes stratification by number of practice capacities and geographical location.
Concealment mechanism
Due to the nature of the intervention design, concealment is not possible.
Implementation
The allocation sequence is generated by a statistician independent of the research team. Details regarding participant and patient enrolment are outlined in the “Recruitment ” section.
Assignment of interventions: blindingWho will be blinded
Due to the nature and design of the intervention, blinding is not applicable. To avoid a potential impact on the healthcare providers’ professional behaviour, they only receive cursory information about PST during the control period.
Procedure for unblinding if needed
Blinding is not applicable in this study.
Data collection and managementPlans for assessment and collection of outcomes
Information about patients is entered into the Healthy Mind website database by healthcare professionals upon enrolment. For patients with a WHO-5 score > 50 points, sex, age, and diagnosis (T2D and/or CHD) are registered. For patients with a WHO-5 score < 50 points, additional registration of social security number, name, contact information, and WHO-5 score is made.
Mental health outcomes
Upon enrolment, an automatically generated link to a questionnaire is sent out to participating patients with a WHO-5 score < 50 points. The questionnaire assesses the primary and secondary mental health outcomes as described above. This link is sent via email/SMS at baseline, as well as after 6 and 12 months. Reminders are sent to non-responders by email/SMS after 1 and 2 weeks, followed by a reminder telephone call after 3 weeks. Patients who are unable to access the electronic questionnaire are provided with an identical paper version at baseline and receive follow-up paper questionnaires by mail after 6 and 12 months. The questionnaires are forwarded to the research team and entered manually into the Healthy Mind database by a data manager independent of the research team. Non-responders to mailed questionnaires receive a reminder telephone call after 3 weeks. The Healthy Mind database mandates that all questionnaire items must be completed before submission, and duplicate registrations cannot be entered, ensuring comprehensive and accurate registrations. More detail on questionnaire properties is provided in Table 2.
Table 2 Overview of mental health outcomes in questionnaires at baseline and after 6 and 12 months
Somatic outcomes
Somatic outcomes are obtained through the local LABKA II database, which contains all results of blood samples analysed in the Central Denmark Region.
Process outcomes
The process outcome data are part of an explanatory sequential mixed methods process evaluation, guided by the UK Medical Research Council framework for process evaluations [30, 31]. Quantitative process outcome data are collected continuously throughout the study via the Healthy Mind website database. Information about fidelity and dose is collected through questionnaires completed by healthcare providers during the registration following each PST session. Reach data are extracted from trial-monitoring records, while data on mediators and unintended consequences come from questionnaires completed by both healthcare providers and patients after the patient’s final PST session.
Qualitative data will be collected through semi-structured interviews with purposefully selected patients (n = 10) after their final PST session. The interview guide will focus on reach, fidelity, mediators, and unintended consequences and will be informed by quantitative process measures from each individual patient. Qualitative interview data will be transcribed verbatim and analysed thematically. The process evaluation will be supplemented by ethnographic case studies exploring the role of context.
Co-variates
At baseline, the Brief Health Literacy Scale for Adults (B-HLA) [32] is applied to measure the level of health literacy. Socioeconomic status data is obtained from the national registers.
Plans to promote participant retention and complete follow-up
General practices receive remuneration for providing information (written and oral), screening eligible patients and completing PST sessions. Remuneration will match the standard remuneration for equivalent services. This incentive will facilitate continuous patient recruitment and delivery of the intervention.
Moreover, healthcare providers are encouraged to monitor patient attendance and ensure that new PST sessions are scheduled upon cancellation or non-attendance.
The number of questionnaire items is kept at a minimum to prevent item attrition, and both electronic and paper questionnaires are available.
Data management
In compliance with the General Data Protection Regulations (GDPR), the study is listed in the record of processing activities at Aarhus University (journal number: 2016–051-000001) [33]. Upon completion of data collection, the data set will be checked for errors, which will be resolved if possible. Computers and servers used for data management will be password-protected. The secure data management system and the Healthy Mind website database are provided by Aarhus University. Data from registers are managed through IT infrastructure provided by Statistics Denmark in accordance with the data management agreement between Statistics Denmark and Aarhus University.
Confidentiality
Data collection, storage, and access will comply with the GDPR regulations [33]. Access to the collected data will only be granted to members of the research group.
Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in this trial/future use
No collection of biological specimens for genetic or molecular analysis is made in this study.


留言 (0)