
記住我

Three mental healthcare institutions in the Netherlands participate in this study: Mentaal Beter (Bergen op Zoom, Roosendaal, Etten-Leur, and Breda), GGz Breburg (Breda), and de Viersprong (Bergen op Zoom). All three of these institutions provide treatments for young people referred for (emerging) mental health problems and offer interventions for a wide range of mental health problems. GGz Breburg provides both MBT-early and CBT, while Mentaal Beter only provides CBT and de Viersprong solely provides MBT-early. Consequently, adolescents referred to Mentaal Beter and randomized to MBT-early will receive treatment administrated by therapists from de Viersprong, while those referred to de Viersprong and randomized to CBT will be treated at Mentaal Beter.
Eligibility criteriaAdolescents are eligible for this study if they meet the following criteria: (a) adolescents between 12 and 18 years old; (b) a depression, anxiety disorder, or both as assessed by the Structural Clinical Interview for DSM-5 Syndrome Disorders (SCID-5-S; [35]); and (c) early stage BPD, defined as three to six features of BPD and mild and moderate disabilities in either school, with family, or with peers or in multiple areas as assessed using the structural clinical interview for DSM-5 Personality Disorders (SCID-5-P; [36]). The exclusion criteria are (a) a primary diagnosis that requires other specialist treatment (e.g. severe autism spectrum disorder, chronic psychotic disorder, severe eating disorder, or severe substance abuse disorder), (b) IQ < 75, or (c) severe disability with regard to functioning in school, at home, and in the peer group representative for later stage BPD [10].
Who will take informed consent?All consecutively referred adolescents between 12 and 18 years old referred to the above mental health care institutions for treatment of presenting symptoms of depression, anxiety, or both, and their parents, will be informed about the study during the first consultation with a mental health professional. They will receive an information letter with detailed information about the study and the screening process. If the adolescent agrees to participate in the screening process, the mental health professional obtains informed consent for the screening process from the adolescent, and from both parents if aged under 16, and asks permission to share their contact information with the research team. The adolescent and parents have at least 1 week to consider their decision about participating in the screening process. After approval for the screening, a research assistant contacts the family to plan the screening. If the inclusion criteria are met, the mental health professional will inform the family that the adolescent is eligible to participate in the study during the second consultation. Again, the adolescent and parents have at least 1 week to consider their decision about participating in the study. If they agree, the research assistant will obtain informed consent for participating in the study from the adolescent, and from both parents if aged under 16, and plan the baseline assessment. After baseline assessment, the adolescent will be randomly assigned to MBT-early or CBT (for more details, see the ‘Assignment of interventions: allocation’ section).
Additional consent provisions for collection and use of participant data and biological specimensAdolescents will be informed that they may withdraw their consent at any moment, while highlighting that data collected up to the point of withdrawal will be used for the study. In addition, they will be asked to give permission to access their data for the purpose of monitoring, by other people from the research team and regulatory authorities that are mentioned in the information letter. Adolescents are also asked if their coded data may be used in follow-up research and if they may be contacted for future research related to this study. Through the consent form, they (and both parents if the adolescent is under [16]) provide their consent for these conditions. This study does not involve the collection of biological specimens.
InterventionsExplanation for the choice of comparatorsTo investigate the effectiveness of early intervention for BPD symptoms in adolescents with presenting depression, anxiety, or both and emerging BPD, CBT for depression and anxiety will be compared to MBT-early. CBT is currently offered as the first-choice psychological treatment for adolescents with presenting symptoms of depression and anxiety, according to the Dutch treatment guidelines [37], following a stepped care approach, where the presenting symptoms of depression and anxiety are typically addressed first, even in the presence of underlying BPD symptoms. Hence, CBT is an appropriate comparative treatment option in the current study as it is currently typically offered to these young people in the Netherlands.
Intervention description CBTCBT [38] is a psychotherapeutic intervention that adolescents with presenting symptoms of depressive and anxiety disorders receive according to the Dutch treatment guidelines [37] as a first-choice psychological treatment. CBT is an evidence-based, goal-directed approach utilizing cognitive restructuring and behavioural interventions. This therapeutic model aims to identify and modify maladaptive thought patterns and behaviours, equipping individuals with practical coping skills to mitigate symptoms and enhance overall emotional resilience. In this study, CBT is offered as an individual treatment following a manualized treatment protocol [39]. The treatment consists of an average duration of 12–16 sessions, encompassing assessment and case formulation, a treatment phase, and a closure phase. Additionally, post-treatment relapse prevention booster sessions may be offered within the first 3 months after treatment.
Assessment and case formulation
This initial phase involves the assessment of the adolescent’s issues and the formulation of a case conceptualization to identify specific problems and tailor treatment accordingly (2–3 sessions). Collaboratively, the therapist and the adolescent establish goals such as symptom reduction, coping skills development, and improvement in daily functioning.
Treatment phase
The next phase of treatment involves interventions such as psychoeducation, teaching coping strategies (breathing and relaxation techniques, problem-solving skills, and distraction techniques), cognitive restructuring (addressing automatic negative thoughts), and exposure exercises (involving gradual exposure to fearful objects or situations), as well as strengthening coping skills and activation (enhancing daily structure such as attending school, engaging in hobbies, and participating in social activities to counteract passive behaviour and avoidance associated with depression) aimed at improving depressive and anxiety symptoms. Parents are provided with information regarding the adolescent’s presenting symptoms and the treatment plan. They are asked to actively engage in facilitating and executing exposure exercises. Additionally, supplementary supportive interventions for parents may be added, if needed [39].
Closure phase
This phase is aimed at reinforcing and maintaining the skills learned during therapy, preventing potential relapse or setbacks. Sessions focus on the evaluation of the treatment gains in relation to the predetermined goals and teaching of relapse prevention (2–3 sessions). Booster sessions involve additional sessions or follow-up sessions scheduled within the first 3 months after treatment completion (2–4 sessions). The booster sessions aim to consolidate progress, address any emerging issues, and fine-tune strategies to ensure the sustained effectiveness of the treatment over time.
MBT-earlyMBT was originally developed as an intervention for adults with BPD. Several types of MBT for BPD are empirically supported [40,41,42]. MBT-early, developed at de Viersprong and implemented since 2014, has offered preliminary support from a small naturalistic pilot study [43].
The aim of MBT-early is to improve the capacity for mentalizing and social learning (i.e. epistemic trust). Impairments in these fundamental capacities are assumed to underly psychopathology [44]. MBT-early aims to facilitate adolescents and their parents to better understand their own and others’ thoughts, feelings, intentions, and motivations and to foster epistemic trust, i.e. nurturing confidence in one’s own perceptions and beliefs, as well as developing trust in others’ perspectives.
MBT treatment programmes vary in terms of treatment components, duration, and intensity. MBT-early shares with all other MBT programmes that it is highly structured and systemically planned. The three C’s, consistency, constancy, and coherence, form a foundational principle for all MBT treatment programmes (see a detailed description elsewhere, [45]) and thus for MBT-early.
MBT-early is a time-limited specialized treatment for emerging BPD and comprises two phases: an initial intensive treatment phase of 16 weeks, followed by a 6-month booster treatment phase.
Intensive treatment phase
The intensive treatment phase consists of an assessment phase (3–4 sessions), a middle phase (10 sessions), and a final phase (2 sessions). The sessions include 16 individual sessions, 3 family sessions, 2 treatment review sessions, and, if necessary, psychiatric consultations and case management (e.g. consultation with school). These treatment modalities are delivered by 1 therapist, and interventions are tailored to the specific needs of the adolescent and his/her family (e.g. case management may partially replace individual sessions if problems manifest primarily at school). However, this standard package can be downscaled in cases of rapid improvement or upscaled when needed.
Booster treatment phase
The intensive treatment phase is followed by a booster phase with follow-up sessions 1, 2, 4, and 6 months after the end of the first phase. At the final session, the treatment progress is assessed to determine if the therapy can conclude or if a new phase of care is necessary. Additional care can be provided in consultation with the family and the treatment team, even after the closure of the adolescent’s case.
Criteria for discontinuing or modifying allocated interventionsAdolescents can withdraw from the study at any time for any reason if they wish to do so without any consequences for their treatment, i.e. they can complete their current assigned treatment (either MBT-early or CBT), but will not be contacted for further assessments. Previously collected data will be included in the analyses.
The research team will register and follow up all potential serious adverse events (SAEs) that might be associated with the treatment (e.g. suicide), which may ultimately lead to the ending of the study. These SAEs will also be reported and discussed at a trial steering committee (TSC). The TSC may decide to end the study prematurely if a significant difference in SAEs (> 5) is shown between the two treatment conditions. For more details on the SAEs, see ‘Adverse event reporting and harms ’ section.
Strategies to improve adherence to interventionsBoth the CBT and MBT-early teams consist of therapists with broadly ranging level of experience, background, and educational level. All therapists involved in the study are certified psychologists, sociotherapists, remedial educationalists, or psychotherapists. Clinicians within the CBT teams who are involved in the study have successfully completed a certified CBT basic course or are further trained in CBT. CBT therapists have weekly one-on-one supervision to review case material with their supervisor. MBT-early therapists who are involved in the study have successfully completed a certified MBT basic course at the minimum or are further trained in MBT. Within the MBT-early programme, biweekly team supervision focuses on reviewing case material to increase therapists’ comprehension of mentalizing theory and their competency in working with the principles of MBT and the spectrum of mentalizing interventions. In order to test for adherence, ten randomly selected individual sessions of both CBT as well as the MBT-early will be scored on an, for the treatment appropriate, adherence scale.
Relevant concomitant care permitted or prohibited during the trialBy default, no other interventions will take place during the intensive phase of treatment. However, when it is deemed clinically necessary to add other psychological interventions, concomitant care can be offered within the same mental healthcare institution as the assigned treatment or somewhere else.
Provisions for post-trial careThroughout the treatment, the mental health professional will, in collaboration with the adolescent, evaluate whether the allocated treatment is sufficiently beneficial or if an alternative treatment might be more appropriate, either within the same mental healthcare institution or elsewhere. After dropping out or completing the allocated treatment, participants can also receive the non-assigned treatment (e.g. receiving MBT-early after completing CBT or vice versa). Based on the intention-to-treat principle, adolescents dropping out of the allocated treatment will be followed for research purposes, unless they withdraw their consent to participate in the follow-up assessments.
The sponsor has a liability insurance which is in accordance with Article 7 of the WMO (Medical Research Involving Human Subjects Act; in Dutch: Wet Medisch-wetenschappelijk Onderzoek met Mensen [WMO]). The risks of participating in this study are minimal. The interviews and assessments may be somewhat burdensome but do not carry specific risks. For this reason, the sponsor is dispensed from the obligation to provide insurance for participating in medical research by the Medical Research Ethics Committee (in Dutch: medisch-ethische toetsingscommissie [METC]) of the Erasmus Medical Center (MC).
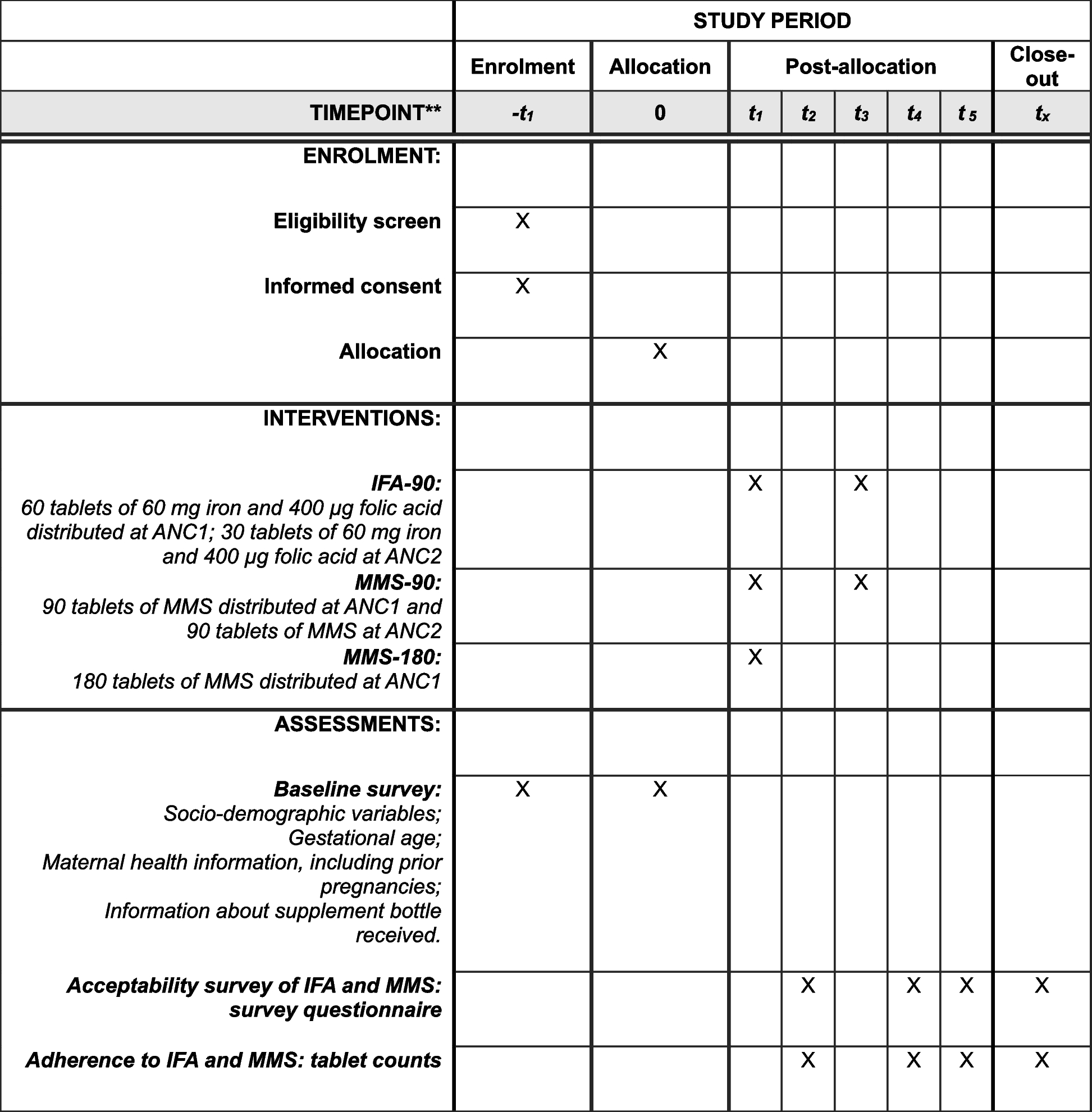
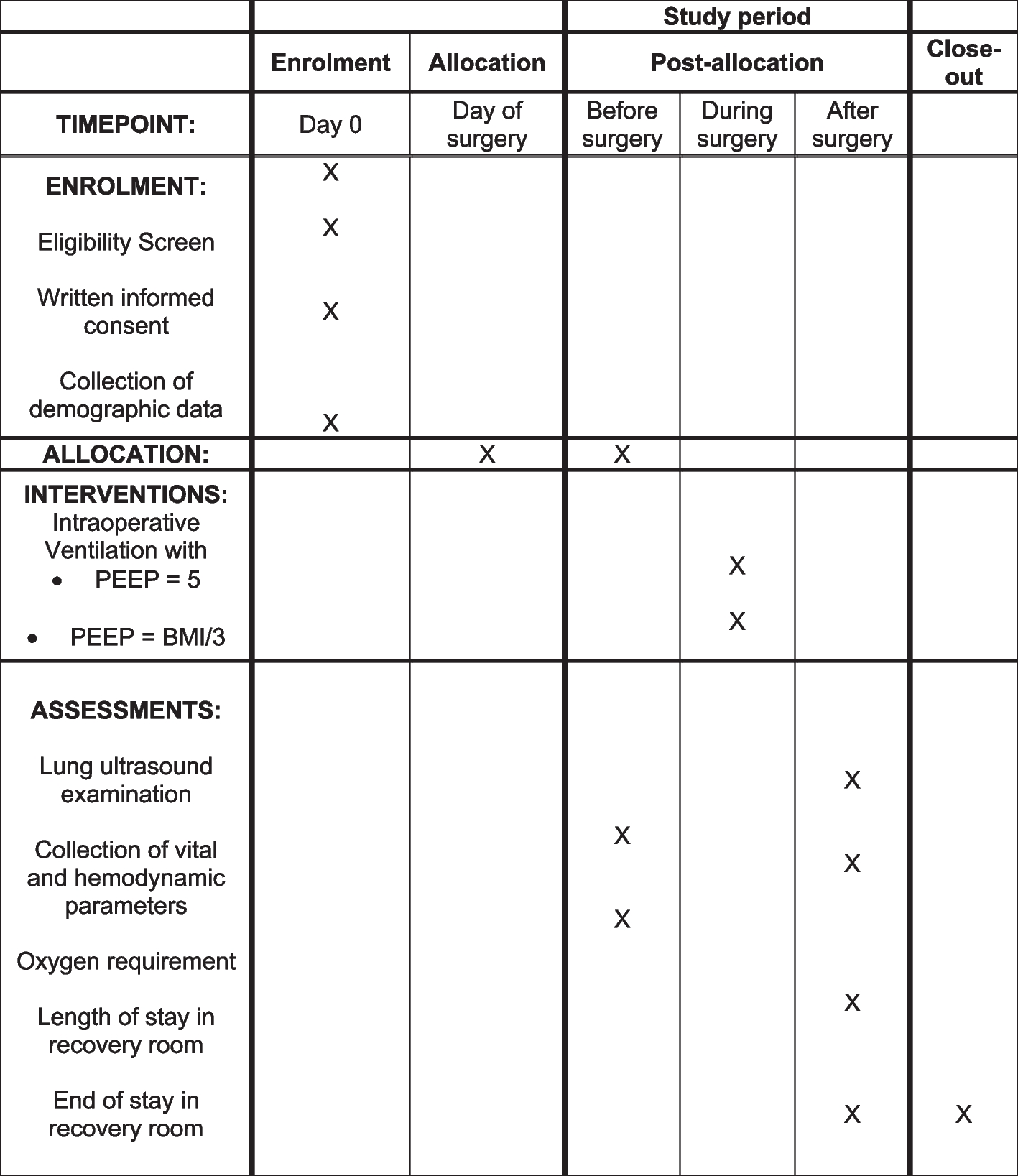
OutcomesTable 1 presents an overview of the time points for each outcome measure.
Table 1 Time point of each outcome measurePrimary outcome Severity of BPD symptomsThe primary outcome variable is the reduction in severity of BPD symptoms from baseline to end of treatment assessed using the Borderline Personality Disorder Symptom Severity Index for Adolescents (BPDSI-IV-ado). The BPDSI-IV-ado is a semi-structured interview to assess the severity of BPD symptoms in adolescents and to detect short-term changes [46]. The BPDSI-IV-ado consists of 72 questions, spread over the 9 criteria for BPD. The total scale ranges from 0 to 90, and the subscales range from 0 to 10. The interview is designed to obtain detailed scores for each BPD symptom and to assess the severity of BPD symptoms over the past 3 months. The internal consistency of the BPDSI-IV-ado is moderate to high (Cronbach’s α ranging from 0.62 to 0.94) and the BPDSI-IV-ado has been demonstrated to be a reliable and valid instrument for the assessment of the severity of borderline symptoms in adolescents [46].
Secondary outcomes Severity of depression and anxietyThe Patient Health Questionnaire (PHQ) is a self-administered version of the PRIME-MD diagnostic instrument for common mental disorders [47]. The PHQ-9 is the depression module, which scores each of the nine DSM-IV criteria from 0 (not at all) to 3 (nearly every day). It is used to monitor the severity of depression and response to treatment. The Generalized Anxiety Disorder Scale (GAD-7) is a diagnostic self-report scale for screening, diagnosis, and severity assessment of anxiety disorders [48]. The GAD-7 is based on seven items, which are scored from 0 (not at all) to 3 (nearly every day). Both PHQ and GAD-7 have been recommended by the International Consortium for Health Outcome Measurement (ICHOM; [49]).
In line with recommendations by ICHOM [49] for personality disorders, and for depressive and anxiety disorders, the Columbia Suicide Severity Rating Scale (C-SSRS; [50]) will be used to assess suicidal thoughts and behaviours. The screener version of the scale assesses whether adolescents meet the criteria for specific forms of suicidal behaviour and consists of 3–6 ‘yes/no’ questions (the number of questions depends on the answers given).
To compare the results of this trial with those of other MBT trials, the Brief Symptom Inventory (BSI; [51]) and the Child Behavior Checklist (CBCL; [52]) are also included. The BSI is a self-report questionnaire that also covers depression and anxiety dimensions and can also be used as a global severity index. Adolescents score each item on a 5-point scale ranging from 0 (not at all) to 4 (extremely). Scores represent the intensity of distress over the past week. The Dutch version of the BSI has a good reliability (Cronbach’s α ranging from 0.71 to 0.88, test–retest reliability ranging from r = 0.71 to 0.89) [51]. The CBCL is a child behaviour questionnaire completed by parents. It assesses the competences and emotional and behavioural problems (e.g. depression and anxiety) of the adolescent in a standardized format. The scores on the different domains indicate possible problem areas for the adolescent, from a parental perspective [52].
Personality functioningImprovement of personality functioning will be assessed by the Level of Personality Functioning Scale – Brief Form, version 2.0 (LPFS-BF 2.0; [53]), as a secondary outcome. This self-report measure consists of 12 items rated on a 4-point Likert scale ranging from 0 (very false or often false) to 3 (very true or often true), reflecting the 12 facets of the LPFS as described in section III of the DSM-5 [54]. The internal consistency of the LPFS-BF 2.0 is satisfactory, and sensitivity to change is high [53]. The LPFS-BF 2.0 fits into the recent tradition of dimensional measures of personality problems and has been recommended by ICHOM [49].
Related to improvements in personality functioning are improvements in mentalizing abilities. The Reflective Functioning Questionnaire (RFQ; [55]) is a brief self-report screening measure of reflective functioning. It consists of eight items (e.g. ‘People’s thoughts are a mystery to me’), which are scored on a 7-point Likert scale ranging from 1 (completely disagree) to 7 (completely agree). This instrument assesses the level of certainty (RFQc) and uncertainty (RFQu) about mental states. Internal consistency of RFQc and RFQu respectively are α = 0.65 and α = 0.77 in a clinical sample and α = 0.67 and α = 0.63 in a non-clinical sample, respectively [55].
Social functioningThe World Health Organization Disability Assessment Scale (WHODAS 2.0) assesses disability in psychiatric populations [56]. The 12-item version assesses impairment in six domains: mobility, self-care, understanding and communication, interpersonal relationships, life activities, and community participation. The WHODAS 2.0 has also been recommended by the ICHOM [49].
The adolescents’ quality of life will also be assessed as a measure of social functioning. The KIDSCREEN-10 is an international cross-culturally comparable quality-of-life assessment instrument validated for children and adolescents between 8 and 18 years. It consists of ten items, which provide a global measure of health-related quality of life [57]. The KIDSCREEN-10 has also been recommended by the ICHOM [49]. The EQ-5D-5L is a self-report questionnaire comprising five dimensions for measuring health-related quality of life: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is divided into five levels (no problems, slight problems, moderate problems, severe problems, and unable to/extreme problems). The adult version of the EQ-5D-5L will be used to consistently assess the quality of life during the study, as the youth version of this questionnaire was designed to be used in adolescents up to age 15 years [58].
To assess how social relationships improve, the Dutch translation of the Network of Relationships Inventory-Behavioural Systems Version (NRI-BSV; [59]) is used. Adolescents answer 24 items regarding their relationships with important people in their social network on a 5-point Likert scale (1 = little or none; 5 = the most), which assess support and conflict in social relationships. The NRI-BSV will also be administered to parents to include their assessment of changes in the parent–child relationship.
Academic functioningTo assess academic functioning, adolescents will answer questions concerning their school attendance in the past month (e.g. ‘Have you been to school in the past month?’, ‘Why did you not go to school in the past month?’, ‘Did you skip classes in the past month?’), taking school holidays into account.
Economic evaluationThe intervention costs of MBT-early and CBT will be calculated using a mixture of bottom-up and top-down approaches and will include personnel costs, implementation costs (e.g. hosting and coaching), and overhead costs associated with the treatment (e.g. facilities for coaches).
An adapted version of the Trimbos/iMTA questionnaire for Costs associated with psychiatric illness (TiC-P; [60, 61]) will be used to calculate medical costs beyond the intervention costs specific to MBT-early and CBT. We will use the parent-form questionnaire (TiC-P Kinderen, in Dutch) to assess health care utilization at baseline, end of treatment, and at 12-, 18-, and 24-month follow-up. We slightly adapted the questionnaire by adding questions about the frequency and duration of (suicidal) crisis (with hospitalization needed) and removing questions that are not related to the problems of the target population (e.g. ‘How many appointments did your child have with a dietician in the past 3 months’).
In line with the iMTA Valuation of Informal Care Questionnaire [62], additional costs of parents that are needed for the treatment of their child will be assessed separately (e.g. taking leave from work to bring their child to therapy, transportation costs, having less leisure time). Parents will answer questions concerning this invested time (e.g. ‘Did you take leave from work for your children’s therapy at “Mentaal Beter/GGz Breburg/de Viersprong” in the past 4 weeks?’ or ‘Did you make any extra costs because your child had therapy in the past 4 weeks? E.g. extra travel expenses or arranging a babysitter’). These questions will be assessed at the end of treatment and at 12-, 18-, and 24-month follow-up. QALYs will be estimated by calculating the area under the EuroQol EQ-5D/time curve [63].
Demographic variablesAt the initial assessment (prior to randomization), adolescents will answer questions regarding demographic variables including their living situation, nationality, level of education, and their current school status, employment, or both.
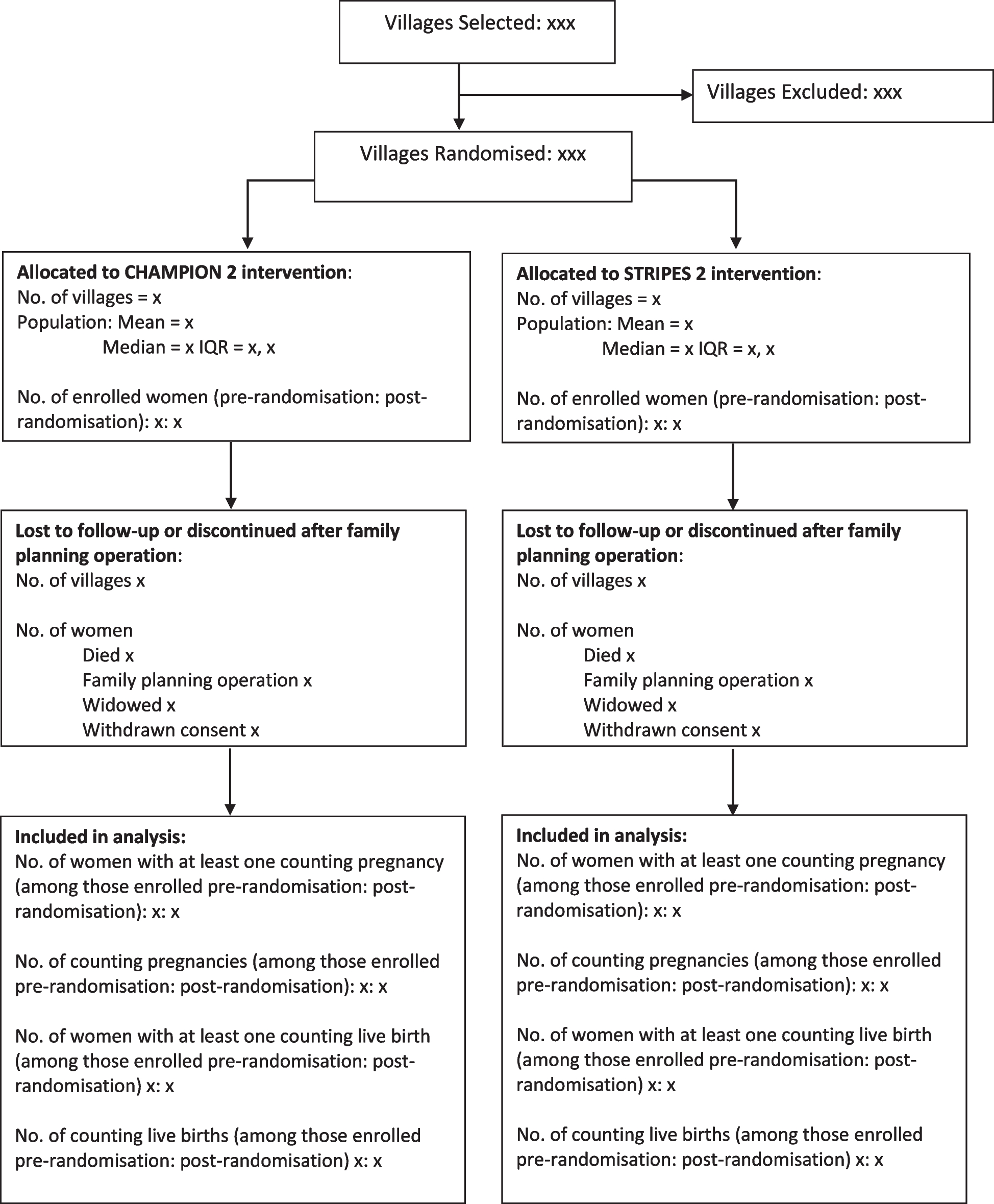
Participant timelineFigure 1 shows the participant timeline.
Fig. 1
Consolidated Standards of Reporting Trials (CONSORT) flow chart
Sample sizeThe sample size is determined by the predicted difference between the groups on the primary outcome, the BPDSI-IV-ado [46]. Consistent with previous studies on MBT for adolescents [43, 64] and MBT for adolescents compared with treatment as usual [27], we expect a medium effect size (Cohen’s d = 0.50) difference between MBT-early and CBT. Based on the BPDSI-IV-ado and with a two-sided α = 0.05, a power of 0.80 and a correlation of 0.50 between the repeated measures, based on Bales et al. [65] and Hutsebaut et al. [43], we require 59 participants in each treatment group (118 in total) with at least 1 follow-up measurement. Because of the vulnerable and unpredictable target population, we anticipate a 10% attrition rate and therefore intend to recruit at least 66 participants per group.
RecruitmentAdolescents will be recruited at three mental healthcare institutions in the Netherlands: Mentaal Beter, GGz Breburg, and de Viersprong. These settings treat young people referred for (emerging) mental health problems and offer interventions for a wide range of mental health problems. Adolescents and their parents are informed during the admission by the clinician about participating in this study and will receive written information. The information folder also includes an infographic about the study. The research team is available to answer questions about the study and will ask for informed consent, if the adolescent is eligible. In cooperation with the involved institutions and local government, informative meetings will be scheduled to inform referrers about this study and the information folders will also be made available to referrers.
Assignment of interventions: allocationSequence generationParticipants will be randomized to either MBT-early or CBT using a computerized 1:1 allocation sequence generated by an independent statistician. Randomization will be blocked with random permuted blocks of sizes 4, 6, and 8.
Concealment mechanismParticipants are randomized by an independent researcher, following a password-protected computer list with the 1:1 allocation sequence. Allocation will be only revealed to the adolescent, therapist and trial coordinator upon randomization by the independent researcher. The research assistants will not be informed about the allocation.
ImplementationAfter informed consent is provided and baseline assessment has taken place, an independent researcher will generate the allocation and inform the trial coordinator about the result. To keep the research assistants blind for the allocation, the trial coordinator directly informs the adolescent (and parents) and therapist about the assigned treatment.
Assignment of interventions: blindingWho will be blindedResearch assistants are kept blind for the treatment allocation. The trial coordinator, adolescent (and parents), and therapist will not be blinded but are strongly inculcated to not disclose the assigned treatment during end-of-treatment assessment and follow-up assessments. To check whether research assistants are still blinded for the assigned treatment during the study, research assistants are asked after each assessment to which treatment the adolescents was allocated.
Procedure for unblinding if neededN/A. Only research assistants will be blinded. There is no need to unblind research assistants, as the trial coordinator, participants, and therapists are all not blind in this trial.
Data collection and managementPlans for assessment and collection of outcomesTo assess the primary outcome, semi-structured interviews will be administered by trained research assistants at baseline, end of treatment and at 24-month follow-up. To assess the secondary outcomes, questionnaires will be collected through the online database BergOp (https://www.bergop.info), to minimize data entry errors. For a detailed description of the instruments used in this trial, see the ‘Outcomes ’ section. For the administration of the BPDSI-IV-ado and C-SSRS, research assistants will be trained and supervised by senior researchers. The research assistant writes a report on the results of the BPDSI-IV-ado and, if requested, provides this report to the adolescent.
All data will be anonymized and saved in a folder on a secured server of ‘de Viersprong’, which can only be accessed by the research team. The data will be stored, coded, and cleaned before analyses (e.g. checking for duplicates, coding of missings and date of entry) in SPSS.
Plans to promote participant retention and complete follow-upResearch assistants will follow and motivate adolescents for the assessments during the study. To limit the burden related to follow-up, questionnaires are provided through an online program, and semi-structured interviews will only be administered at the end of treatment and 24-month follow-up. Adolescents have the opportunity to do the interviews at the location or through video conference. Travel expenses will be refunded and adolescents receive a small gift (with a value of €15) after every completed assessment.
Adolescents are allowed to refuse to participate in an assessment and are not obliged to give a reason for not participating. They will be invited for the next assessment planned unless they withdraw their consent for participating in the study. Adolescents may withdraw from the trial at any time for any reason, without any consequences (i.e. they can complete their assigned treatment) and will not be contacted for further assessments.
Data managementEvery adolescent receives a unique key code, not based on their initials, birthdate or medical record. In the data files, used for monitoring inclusion and data collection, and for the statistical analyses, only the unique key code of each adolescent will be used and no personal identifiable data. The identification code list that connects adolescents with the research data is encrypted and only available to the research team.
Questionnaires will be administrated online through BergOp (https://www.bergop.info), and the results are stored in SPSS. The output of the interviews is also kept in SPSS, and the written reports are stored in a secured folder. Any data on paper (e.g. scoring forms) is stored in a locked room at de Viersprong. All data stored in a secured folder on the network of de Viersprong can only be accessed by the research team. All changes made to the raw data and steps taken in the analyses will be kept in a logbook.
ConfidentialityAs stated under the ‘Data management ’ section, in the research data only the unique key code will be used and no personal identifiable data. Only the research team can store, manage, and access the research data. No personal identifiable data will be reported in publications. Data will be stored for 15 years at de Viersprong, according to the Medical Ethical Committee guidelines.
Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in this trial/future useN/A. No biological specimens will be collected or stored in this study.
留言 (0)