
記住我









Participants will be recruited from up to 35 enrolled sites (acute NHS hospitals, community NHS trusts and primary care centres) in the UK. A list of enrolled sites is available in Supplementary File 1.
Eligibility criteriaVenUS 6 will include adult patients with a venous leg ulcer who meet all the inclusion criteria, and none of the exclusion criteria.
Inclusion criteria 1)Aged 18 years or over.
2)Has at least one venous leg ulcer, defined as ‘as any break in the skin on the leg which is either (a) is venous in appearance and accompanied by signs of chronic venous disease or (b) occurs in a person with a history of venous leg ulceration. The ulcer should be purely venous where clinically no other aetiology is suspected’.
Note: The venous leg ulcer must lie wholly or partially within the gaiter region of the leg; venous leg ulcers which lie partially within the gaiter region and extend onto the foot will be included; however, venous leg ulcers that are confined to the foot only will not be eligible for inclusion.
3)Has an ankle–brachial pressure index (ABPI) of ≥ 0.8, taken within the previous 3 months or, where an ABPI measure is not possible, use of locally approved alternative assessments to rule out peripheral arterial disease, i.e. pulse palpation and Doppler auscultation, toe pressure assessment or arterial imaging, also taken within the last 3 months.
4)Is able to tolerate full compression.
Exclusion criteria 1)Is not willing to wear full compression
2)Has leg ulcers of non-venous aetiology or has significant peripheral vascular disease that contraindicates the use of full compression
3)Has ulcers confined to the foot
4)Lacks capacity or willingness to provide consent to participate in the trial
5)Is currently participating in another study evaluating treatments for their venous leg ulcer
6)Has a known allergy to any trial product
7)Has previously been recruited to VenUS 6
8)Is deemed to be clinically inappropriate to take part in the trial (at clinician’s discretion)
9)Has planned treatment to close/remove incompetent superficial veins (e.g. via endovenous ablation, sclerotherapy) within 28 days
Informed consentInformed consent will be obtained by a suitably qualified and experienced member of the research or clinical care team who has been authorised to do so by the Chief or Principal Investigator. The participant must personally sign and date the latest approved version of the informed consent form before any study-specific baseline procedures are performed.
Part of the consent process will also be to ask for consent to potentially follow up participants beyond the end of the trial for a maximum of 5 years. This is to allow future longer-term research to be considered. The consent form will also ask participants if they would like to take part in a semi-structured interview, which forms part of the study’s process evaluation. This is optional and not participating in the interviews will not affect main trial participation. Once informed consent has been obtained, baseline data will be collected.
Additional consent provisions for collection and use of participant data and biological specimensThere are no biological specimens collected within VenUS 6; therefore, additional consent for collection and use is not required.
InterventionsExplanation for the choice of comparatorsComparators were selected as compression wraps and two-layer bandage systems given the current lack of robust evidence for the clinical and cost-effectiveness of these treatments. Evidence-based compression was selected as the ‘control’ treatment arm as it is supported by the most robust evidence base [5,6,7].
Intervention and control descriptionsRegardless of treatment allocation, all participants will receive standard care including dressing changes, as per routine clinical practice and applied in accordance with manufacturer’s guidelines. The use of any primary contact dressing under the compression therapies being evaluated will be permitted.
Compression wraps armAny adjustable compression sleeve secured with hook and loop (Velcro™) fastenings, designed and marketed to be worn on the lower leg and foot, which aims to deliver > 40 mmHg of compression at the ankle with a system to guide this and is CE marked and available via NHS Prescription, will be permitted for use in VenUS 6.
The compression wraps may be used with a compressive or non-compressive liner and/or with the use of foot compression elements at the discretion of the treating health professional, provided the above criteria are met. Compression wraps marketed solely for treatment of lymphedema will not be included.
Evidence-based compression armGiven the results of VenUS IV [7], which demonstrated two-layer hosiery is as effective as the four-layer bandage in healing venous leg ulcers, a choice comparator arm is included where allocated participants are offered two-layer compression hosiery, if they are deemed suitable, or a four-layer bandage system. This decision will be based on clinical judgement and participant preference. Any four-layer system delivering > 40 mmHg compression at the ankle will be permitted for use.
Similarly, any recognised two-layer compression hosiery delivering sustained graduated compression of > 40 mmHg at the ankle will be permitted for use. Two-layer hosiery comprises an initial layer of understocking or liner providing light compression over which a second overstocking (i.e. UK class 2 or 3 depending on understocking) is applied. Product-specific measurement tables will be consulted to ensure the participant receives the correct size kit, depending on foot length and ankle and calf circumference. Made to measure hosiery kits will also be permitted.
Two-layer bandage armAny recognised two-layer bandage system, consisting of an initial bandage layer covered with a top cohesive compression bandage, which aims to deliver > 40 mmHg compression at the ankle, will be permitted for use. This includes K-Two (Urgo), Coban 2, Andoflex and Actico2c. Other two-layer bandage kit systems will be considered on a case-by-case basis by the Chief Investigator, Trial Manager, and clinical members of the trial management team prior to use.
Criteria for discontinuing or modifying allocated interventionsGiven the pragmatic nature of the trial, the decision for discontinuation of the intervention or control treatment will be made by the clinical care team in conjunction with the participant. Details of discontinuation and any alternative treatments provided will be recorded during ulcer-related dressing visits and/or monthly follow-up calls.
During the study, modifications may be made to the treatment as required by the clinical care team and details of any changes will be recorded during ulcer-related dressing visits and/or monthly follow-up calls.
Strategies to improve adherence to interventionsDecisions for continuation or discontinuation of interventions will be at the discretion of the clinical care team, in conjunction with the participant, so no specific strategies have been included to improve intervention adherence.
Relevant concomitant care permitted or prohibited during the trialThroughout the study, concomitant medications or treatments deemed necessary may be prescribed.
Provisions for post-trial careAt the end of the trial, participants will return to the care of their treating healthcare professional to determine any further treatment required. This may or may not include compression therapy as appropriate.
OutcomesHealthcare professionals will phone participants monthly to monitor when the reference ulcer (defined as the ulcer with the largest surface area (cm2) where multiple ulcers are present) is healed. Other outcomes assessed in this way are the reference leg being ulcer-free, participant trial status and any clinical events experienced. Calls will continue throughout the study regardless of healing up until the participant exits the trial.
Primary outcomeThe primary outcome for VenUS 6 will be time to healing of the reference ulcer, defined as ‘complete epithelial cover in the absence of a scab (eschar) with no dressing required’ in days from randomisation. Treating nurses will be asked to report the date when they consider the reference ulcer to be healed.
Once healing has been confirmed the treating nurse or participant will take a digital photograph once a week over the next four consecutive weeks. Standardised study specific, photography guidance and a camera will be provided to facilitate this.
Given the increased risk of bias associated with non-blinded outcome assessment for subjective outcomes such as ulcer healing [13], blinded outcome assessment will be undertaken using digital photographs. These photographs will be assessed independently by two clinical experts (experienced tissue viability nurses not involved in the care of VenUS 6 participants) blinded to allocation. Any disagreements will be resolved through a third reviewer. The blinded assessment of the healing date will be used as the primary healing endpoint. Non-blinded assessment of healing will be used as a secondary outcome.
Secondary outcomesSecondary outcomes are:
1.Clinical events including healing of the reference leg, ulcer recurrence, ulcer/skin deterioration, amputation, admission/discharge, planned treatment to close/remove incompetent superficial veins (e.g. via endovenous ablation, sclerotherapy) within 28 days, infection, new ulcer occurrence or death. Details of any clinical events will be recorded during ulcer-related treatment visits and via the monthly telephone follow-up.
2.Changes to allocated treatment and reasons for change will be collected until either the participant’s reference leg is ulcer free or until the participant exits the trial. The date of visit, the type of compression being received and the type of primary contact dressing being used will be recorded. Where changes to the type of compression are made, we will record the date of the change, the changes made, the reason for this change and who requested the change (patient or clinician). Details will be recorded during ulcer-related treatment visits.
3.Health-related quality of life will be collected using the VEINES QoL [14] and EQ-5D-5L [15] which will be completed by the participant at baseline and 3, 6 and 12 months, with the EQ-5D-5L also collected at 1 month post-randomisation.
4.Adherence to treatment and ease of use questionnaires will be completed by the participant at 1, 3, 6 and 12 months, including views on the compression treatment received, volume of treatment use and reasons for reduced dose.
5.Ulcer-related pain using the 21-point Box Scale (BS-21) divided into units of five ranging from 0 (no pain) to 100 (the worst pain imaginable). This will be completed by the participant at baseline and 1, 3, 6 and 12 months.
6.Resource use, i.e. ulcer-related consultations received from the NHS, will be completed by participants at 3, 6 and 12 months. Details of ulcer-related dressing changes (frequency, type, activity) will also be collected at every nurse visit.
Additionally, data including demographics, diabetes status, venous leg ulcer surgical history, reference ulcer assessment, physical measures (i.e. stature, mass, and mobility), current ulcer treatments and an ulcer photograph will be collected at baseline.
SWAT outcomesThe primary outcome of SWAT 1 (use of infographic at recruitment) will be the recruitment rate, i.e. the proportion of participants in each group who are randomised into the host trial. Secondary outcomes will include the proportion of patients in each group who are screened but do not go on to be randomised, and the cost-effectiveness of the intervention.
For SWAT 2 (newsletter and/or thank you card), the primary outcome will be the questionnaire response rate, i.e. the proportion of participants who return their completed questionnaires at month six in each group. Secondary outcomes will include response rates at 12 months, whether a reminder notice is required, completeness of response, and cost of the intervention per participant retained.
For SWAT 3 (pen with questionnaire), the primary outcome will be the questionnaire response rate, i.e. the proportion of participants who return their completed questionnaires at month three in each group. Secondary outcomes will include response rates at 6 and 12 months, whether a reminder notice is required, completeness of response, and cost of the intervention per participant retained.
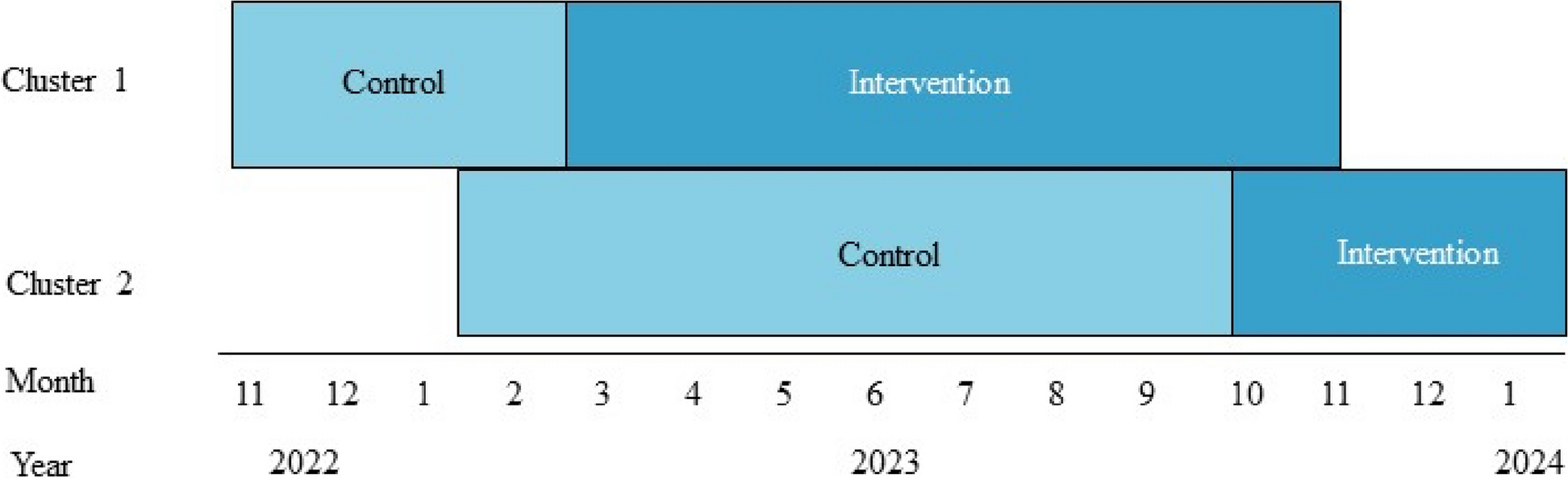
Participant timelineSee the participant timeline in Fig. 1 and SPIRIT figure in Table 1.
Fig. 1
VenUS 6 participant timeline
Table 1 VenUS 6 SPIRIT figureSample sizeBased on parameters from VenUS I [5, 6] and VenUS IV [7], a hazard ratio (HR) of 1.33 will be used as the non-inferiority margin for the comparison of the two-layer bandage arm and evidence-based compression arm. We assume a median time to healing of 2.3 months in the evidence-based compression group, an average follow-up time of 12 months and 10% attrition (pre-healing). We also assume that there is truly no difference between evidence-based compression and two-layer bandage under the alternative hypothesis for this test (i.e. HR = 1). Under these assumptions, 225 patients per group are required to obtain 80% power for a one-sided test of size 2.5% of the null hypothesis that two-layer bandage is inferior to evidence-based compression by a clinically relevant amount (i.e. HR = 1.33).
We also plan to recruit 225 patients to the compression wraps group. Under the same assumptions regarding healing rate in the evidence-based compression group, length of follow-up time and attrition as stated above, and assuming a hazard ratio of 1.33 (comparing compression wraps with evidence-based compression) under the alternative hypothesis, this sample size (i.e. 225 per group) obtains 80% power for a superiority comparison of evidence-based compression and compression wraps using a two-sided test of size 5%. If the two-layer bandage and evidence-based compression groups are combined and compared 2:1 against compression wraps, then under the same assumptions as the superiority comparison outlined above, this sample size (i.e. 450 vs 225) would obtain 90% power for a two-sided test of size 5%.
We will only combine the evidence-based compression and two-layer bandage groups for the superiority comparison with compression wraps if two-layer bandage is found to be non-inferior to evidence-based compression (i.e. the null hypothesis of the non-inferiority comparison is rejected). If the null hypothesis of the non-inferiority comparison is not rejected, then the evidence-based compression and two-layer bandage groups will not be combined, and compression wraps will be compared with each of these groups individually (i.e. compared 1:1:1). Under the same alternative hypotheses (i.e. HR(evidence-based compression/two-layer bandage) = 1 and HR(compression wraps/evidence-based compression) = 1.33) and assumptions (i.e. median healing time of 2.3 months in the evidence based compression group, average follow-up time of 12 months, 10% attrition) as above, the power to detect superiority of compression wraps over evidence-based compression or evidence-based compression and two-layer bandage combined is approximately 86%.
For the SWATs, as is usual with nested trials, a formal power calculation to determine sample size has not been conducted as the sample size is constrained by the number of patients approached about, or recruited into, the study, respectively [16].
RecruitmentPotential participants will be identified through clinical caseloads and screened for eligibility in the participating acute, community or primary care sites. It is however anticipated that most participants will be recruited from community NHS Trust settings.
Potential participants will be approached with further study details, including a PIS by a member of the clinical care or research team. The participant will be allowed as much time as required to consider the information and what giving informed consent involves and will be given the opportunity to ask any questions to relevant parties.
It will be made clear to individuals that they are free to withdraw from the study at any time for any reason without prejudice to future care, and without giving a reason for withdrawal. Should new information arise during the study which may affect an individual’s willingness to take part, this will be reviewed for addition to the PIS and a revised consent form will be completed, as necessary.
A recruitment SWAT is also included in the study, as previously described.
留言 (0)