
記住我

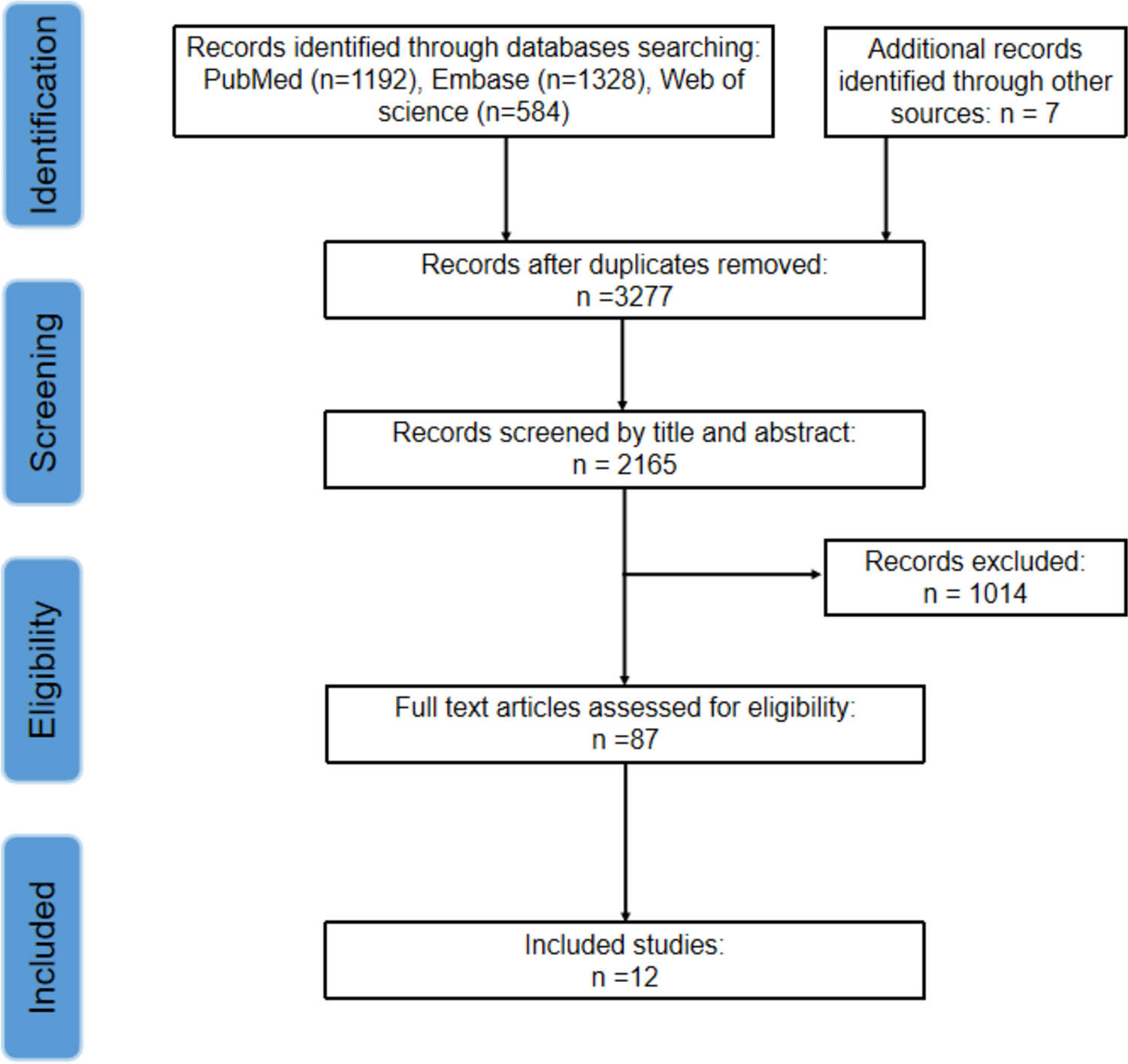

The search strategy — according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) [9] — is shown in Fig. 1. We searched PubMed, Web of Science, and Scopus. Literature search strategies used for each database and the syntax search terms are displayed in Supplementary Table 1. The search retrieved 8422 articles. After removing papers < 2020, duplicated records, reviews, non-human studies, etc., we review 39 papers, discussed in Table 1.
Fig. 1
PRISMA 2020 flow diagram of plant-based diets studies (as related to blood pressure) retrieved
Table 1 Recent studies on plant-based diets and blood pressureEvidence on the Effects of Particular Plant-Based DietsMany types of dietary patterns exist in the arena of essentially plant-based diets, including vegetarian diets and their variants, the Dietary Approach to Stop Hypertension (DASH) diet, the Mediterranean (Med) diet, the healthy Nordic diet, and many other high-fruit, vegetable, and whole grain diets.
Vegetarian DietsVegetarian diets usually do not include meat, poultry, or fish, although individual eating patterns do vary. Lacto-ovo-vegetarian diets are based on grains, vegetables, fruits, legumes, seeds, nuts, dairy products, and eggs, excluding meat, poultry, and fish. The lacto-vegetarian diet also excludes eggs besides meat, poultry, and fish. The vegan, or pure vegetarian diet not only excludes meat, poultry, or fish, but also dairy and additional animal products. A meta-analysis of 32 cross-sectional studies, including more than twenty-thousand individuals, indicated that a lower mean BP was related with the intake of vegetarian diets compared to omnivorous ones [10]. Accordingly, a recent meta-analysis, comprising a total of 187 participants from five controlled trials, showed a mean reduction in systolic blood pressure (SBP) (−5.47 mmHg (95% CI, −7.60, −3.34); P < 0.00001) and diastolic blood pressure (DBP) (−2.49 mmHg (−4.17, −0.80; P = 0.004) in subjects using a lacto-ovo vegetarian diet compared with the consumption of comparator diets, with a high certainty of the results for SBP and a moderate one for DBP [11]. Furthermore, a meta-analysis, which included 856 subjects from 15 randomized controlled trials (RCTs), showed that vegetarian diets significantly reduced SBP (−2.66 mmHg (−3.76, −1.55), P < 0.001) and DBP (−1.69 mmHg (−2.97, − 0.41), P < 0.001) compared to omnivorous diets [12]. In the subgroup analysis, a vegan diet showed higher decrease in SBP (−3.12 mmHg; (−4.54, −1.70), P < 0.001) compared to a lacto-ovo-vegetarian diet (−1.75 mmHg, (−5.38, 1.88), P = 0.05). The vegan diet showed a similar trend in terms of DBP reduction (−1.92 mmHg (−3.18, −0.66), P < 0.001), while those in a lacto-ovo-vegetarian diet did not. Conversely, another meta-analysis, including 677 individuals from nine controlled trials, showed that the consumption of vegan diets was not significantly associated with a mean reduction in SBP (−1.30 mmHg (−3.90, 1.29); P = 0.33) and DBP (− 0.81 mmHg (−2.91, 1.28); P = 0.45) compared with the consumption of comparator diets, although the reliability of results was low [13]. Moreover, the authors acknowledge that the use of BP-lowering comparator diets probably underrated the BP-lowering capability of vegan diets. Indeed, when the usual diet of volunteers was used as the comparator, there was a statistically significant overall effect estimate, although reliability remained low.
DASH DietThe DASH randomized trial was designed to evaluate the effects on BP of a fundamentally plant-based diet, which included plant foods, low-fat dairy, and limited amounts of lean meat [14]. During this eight-week trial, volunteers consumed one of the following diets: (1) a “standard” American diet (control), (2) the DASH diet, or (3) a fruits and vegetables diet. Compared to the fruits and vegetables diet, the DASH diet had a reduced fat content and consisted in more daily servings of fruits and grains and fewer meat servings. The DASH diet reduced BP when compared with the control diet, especially in African Americans, and in already hypertensive subjects [15, 16]. The potential impact on BP reduction caused by a plant-based diet was verified in the DASH-sodium trial, which showed that restraining sodium led to further effects on BP reduction in combination with the DASH diet [17] and that higher BP levels at baseline were associated with an enhanced reduction of BP [18]. A recent meta-analysis comprising a total of 1400 participants from 11 controlled trials showed that SBP (−5.53 mmHg (95% CI −7.95, − 3.12); P < 0.00001) and DBP (–3.78 mmHg (–5.51 to –2.04); P < 0.0001) levels were reduced upon consumption of DASH diets compared with the consumption of comparator diets, with a high degree of certainty of the results [13].
Mediterranean DietThe Mediterranean (Med) diet entails a moderate intake of poultry, eggs, seafood, and dairy products and a low consumption of red and processed meats. In this sense, the Med diet can be considered to a large extent to be a plant-based diet, as it comprises a high consumption of plant-based foods such as fruits, vegetables, legumes, grains, nuts, and olive oil [19]. In a meta-analysis of observational studies, including prospective and cross-sectional (four and eight, respectively) studies, representing over 30,000 individuals and 6342 cases of metabolic syndrome (MetS), BP showed an inverse significant association with high adherence to the Med diet (RR = 0.87; 95% CI: 0.77–0.97) [20]. Several RCTs have estimated the effects of the Med diet on BP, and at least three meta-analyses showed consistent results. The first one, which included six trials, comprising more than 7000 people, found that adopting a Med diet pattern for at least 1 year reduced both SBP (− 1.44 mmHg) and DBP (− 0.70 mmHg) levels [21]. Another meta-analysis included three RCTs focused on different healthy dietary patterns and reported an association between the Med diet and a reduction on SBP (− 3.02 mm Hg) and DBP (− 1.99 mm Hg) [22]. Finally, a more recent meta-analysis, comprising a total of 5276 participants from eight controlled trials, showed that SBP (− 0.95 mmHg; 95% CI, − 1.70, − 0.20); P < 0.00001) and DBP (− 0.69 mmHg (− 1.44, 0.06); P = 0.07) levels were lessened upon consumption of a Med diet compared with the consumption of comparator diets, with a moderate certainty of the results [13].
Nordic DietLike the DASH and Med diets, the healthy Nordic diet is essentially a plant-based dietary pattern, consisting of whole grains, fruits, vegetables, legumes, rapeseed oil, fatty fish (e.g., salmon), shellfish, seaweed, low-fat meat (e.g., poultry), and dairy, along with restraining salt and sugar-sweetened products [23]. A recent meta-analysis, comprising a total of 420 participants from three controlled trials, showed that the consumption of a healthy Nordic diet led to a reduction in SBP (− 4.47 mmHg; 95% CI, − 7.14, − 1.81); P < 0.001) and DBP (− 2.32 mmHg (− 3.83, − 0.82); P = 0.002) levels compared with the consumption of comparator diets, with a moderate certainty of the results [13].
Other High-Fruit/-Vegetable/-Fiber DietsDiets not fitting in the previous categories, but that could still be contained in the plant-based diet arena include the ones characterized by increased consumption of fruit and vegetables and high-fiber diets focused on increasing whole-grain and legume consumption. In a meta-analysis including 140 subjects from two RCTs, high-fruit/high-vegetable diets were linked with reduction in SBP (− 0.57 mmHg (− 7.45, 6.32); P = 0.87) and DBP (− 0.96 mmHg (− 3.08, 1.15); P = 0.37) compared with the consumption of comparator diets [13]. Similarly, consumption of high-fiber diets resulted in a decrease in SBP (− 0.65 mmHg (− 1.83, 0.53); P = 0.28) and DBP (− 1.02 mmHg (− 3.86, 1.82); P = 0.48) compared with the consumption of comparator diets (meta-analysis with 316 subjects from two RCTs) [13]. However, in both cases, the certainty of evidence was extremely low.
In line with the results described above, Dinu and colleagues published the first umbrella review focusing on the effects of different popular diets on cardiometabolic risk factors [24•]. Regarding plant-based diets and BP outcomes, the review included meta-analyses of RCTs assessing the DASH (n = 6), Mediterranean (n = 11), vegetarian (n = 9), and Nordic (n = 2) diets, among others. Overall, the findings of this review support that balanced dietary patterns, favoring vegetables, fruits, whole grains, and plant-based protein, and limit sugar, sodium, and red and processed meat, are beneficial in adverse cardiometabolic scenarios. Notably, DASH and, especially, Med diets showed the most consistent findings regarding a reduction in BP accompanied by improvements in other parameters, whereas for the Nordic and vegetarian dietary patterns, only weak evidence of a beneficial effect in BP levels was found. Nevertheless, the authors emphasize that around 80% of the meta-analyses included in the study suffered from low methodological quality and weak strength of evidence and included, for many diets, a reduced number of clinical trials. Furthermore, the authors acknowledge the limitations concerning the understanding, meaning, and applicability of findings in clinical practice. For instance, meta-analyses, in many cases, included RCTs performed on individuals in a variety of pathological settings and the extrapolation of results to the general population is not straightforward.
Evidence Coming from Recent RCTsIn the last 3 years, evidence generated from RCTs on the effect of plant-based diets has been plentiful. Limiting this list to trials where at least one arm included a recognizable plant-based diet as the main exposure of interest and where BP and/or hypertension were outcomes of interest returned 39 papers (Table 1). Most studies concern the exposure of overweight/obese subjects at (high) risk of cardiometabolic disease, e.g., metabolic syndrome, type 2 diabetes mellitus (T2DM), and non-alcoholic fatty liver disease (NAFLD), to diets based on the Mediterranean or DASH dietary patterns, although vegan and vegetarian diets, among others, were also investigated. Healthy/pathological context scenarios other than the above mentioned include rheumatoid arthritis and chronic kidney disease, etc. The main results of these studies regarding BP values and/or hypertension reinforce the conclusions of the above-mentioned umbrella review and several other meta-analyses. Sub-studies from the PREDIMED and PREDIMED-Plus trials confirm that a high adherence to the Med diet is associated with lower BP values (vide infra). Of note, non-treated participants following a Med diet showed less need for the use of antihypertensive drugs [25]. Indeed, Med diet adherence was associated with decreased need of escalating antihypertensive therapy in patients who were using two drugs at baseline and attenuated the association of antihypertensive drug use with the risk of cardiovascular events [25]. As for the PREDIMED-Plus trial, at baseline, a tendency was found towards a lower Med diet adherence for participants with the highest validated MetS severity score, which (among many other parameters showing unfavorable readings) were characterized by high BP levels [26]. On the other hand, also at baseline, adherence to eight a priori high-quality dietary scores did not show inverse associations with hypertension [27]. Longitudinal analysis showed that the reductions in SBP and DBP were enhanced with higher carbohydrate quality index (categorized in quintiles and based on four criteria: total dietary fiber intake, glycemic index, whole grain/total grain ratio, and solid carbohydrate/total carbohydrate ratio) [28]. Decreases in SBP were significantly associated with increased nut consumption [29], although results from a 2-month crossover RCT showed non-significant intra- and inter-group differences in SBP and DBP in MetS subjects who consumed a Med diet or a non-Med diet plus nuts (50 g/day) [30]. Some studies propose that, alongside a higher adherence to Med diet, other factors, such as physical activity, low sedentary time, or low depression risk, could contribute to enhance the positive effects seen on hypertension (among other CVD risk factors) [31, 32].
Apart from the PREDIMED trial, in the last 3 to 4 years, many RCTs on the effects of Med diets have been published in different physio-pathological contexts. Adherence to Mediterranean-based dietary patterns was associated with favorable effects on BP in apparently healthy individuals [33], overweight/obese at high risk of CVD [34-38], MetS [39], prediabetic [40], T1DM [41], T2DM [42], NAFLD [43, 44], heart or lung transplant recipients [11], obstructive sleep apnea [31], HIV [45], rheumatoid arthritis [46], and cancer patients [47], among others. However, in general, the differences observed were not significant between the intervention groups on the Med diet and other groups. In some cases, neither intra-group nor inter-group significant differences were found, as was the case of individuals without major CVD who consumed the Atlantic diet, for 6 months. This diet has several characteristics in common with the Med diet such as high consumption of vegetables, fruits, whole grains, beans, and olive oil as a key fat source. It is also characterized by high intake of fish and seafood, starch-based products, nuts, milk, and cheese. In professional female handball players who consumed a free diet, a Med diet, or a high antioxidant diet, for 12 weeks, there were no significant differences in BP over time or between groups [48, 49].
Regarding the effects of DASH-based diets on BP, a longitudinal analysis was conducted with one-year data of changes in the DASH diet score and its association with cardiometabolic risk factors in PREDIMED-Plus trial [50]. After adjusting for several potential confounders, higher DASH diet scores were significantly associated with lower SBP (− 0.57 mmHg) and DBP (− 0.15 mmHg). Furthermore, in a RCT with individuals with untreated high normal BP or stage 1 hypertension, Japanese cuisine-based DASH (J-DASH) diets, which are in accordance with the nutritional composition of the DASH diet (but have less total fat and saturated fatty acids), improved home measured BP and stabilized its variability compared to a group who consumed their usual diet [51]. An investigational diet mimicking the average East Asian diet, but retaining common characteristics of the Med and DASH diets, also produced positive effects on BP, in subjects with T2DM [52]. Finally, in CVD risk patients with MetS, a modified DASH diet with additional emphasis on plant-based and Med diets to optimize refeeding also led to a reduction in SBP after 3 months. According to the results of this study, volunteers who had a 5-day fasting prior to following the modified DASH diet showed a sustained reduction both in 24-h ambulatory SBP and mean arterial BP (MABP). Indeed, subjects undergoing fasting reduced their intake of antihypertensive medication in 43% of cases, whereas on DASH alone this happened in 17% of cases.
In the context of RCTs aimed at assessing the effects of vegan and/or vegetarian diets where BP values were evaluated a few studies are worth discussing. In a crossover RCTwith overweight individuals, SBP and DBP values decreased (−9.3 and −7.3 mmHg, respectively) in subjects on a Med diet compared with a vegan diet (−3.4 and − 4.1 mmHg, respectively) [53]. In contrast, 6 months of a vegetarian diet (very-low-protein diet) significantly lowered SBP and DBP more effectively than a Med diet or a Med diet supplemented with essential amino acids and ketoanalogs (Med diet + KA) [54]. In another study, subjects with cardiometabolic risk factors were instructed to consume ad libitum whole-food plant-based diets, consisting of vegetables, grains, legumes, and fruits and avoidance of animal products. Compared to the control group, who consumed an omnivorous diet, there was a tendency for more favorable effects in SBP and DBP [55]. In another study, a low-carbohydrate vegan diet, high in canola oil and plant proteins, was compared to a vegetarian therapeutic diet in type 2 diabetics [56]. There were no changes in BP medications and no treatment differences in BP. However, within treatment, significant reductions in SBP and DBP were seen on the low-carbohydrate vegan (−4.12 and −3.54 mmHg, respectively) and on the vegetarian diet (−5.91 and −4.13 mmHg, respectively). Still on vegetarian diets, a plant-based diet built on the USDA healthy vegetarian meal plan, with modifications to exclude eggs and dairy products, was compared with the same diet except for eggs being permitted (2 eggs/d for 6 weeks while preserving an isocaloric condition) in individuals at risk of T2DM. SBP, DBP, and MABP decreased from baseline in both groups (statistical significance was only found for plant-based diet + eggs), yet changes were not significantly different between groups [57]. On the other hand, a plant-based diet with either 2 eggs/d or the equivalent amount of egg substitute showed no effect in SBP and DBP in MetS subjects [58]. A study carried out in prediabetic subjects who consumed one of three isocaloric-restricted diets: (1) Med diet, (2) a traditional Jiangnan diet high in plants, or (3) a control diet low in plants, for 6 months, showed significant decreases from baseline in SBP and DBP for all diets but differences between groups were non-significant [40]. In a another RCT, rheumatoid arthritis patients completed a 7-day fast followed by an 11-week plant-based diet or a 12-week standard Deutsche Gesellschaft für Ernährung (DGE) diet [59]. Neither dietary protocol lowered SBP, although there was a tendency to decrease DBP in the fasting + plant-based diet group. In another study, all 3 healthy eating patterns: (1) plant-based diet, (2) AHA diet, or (3) Med diet, were associated with similar statistically significant improvements in SBP and DBP, in children with BMI > 95% age/sex predicted [60].
In T2DM [61] and in normotensive women [62], increasing the amount of vegetable, fruit and whole grain dietary intake produced favorable effects in BP. On the other hand, BP did not improve in children, adolescents, and adults included in an intervention group instructed to eat more healthy food items, such as fruits and vegetables, legumes, fish, nuts and seeds, and olive oil, compared to the control group [63]. Furthermore, 12 weeks of consumption of a traditional Brazilian Diet (DieTBra), consisting of plenty of tropical fruits, rice and beans, raw and cooked vegetables and legumes, moderate consumption of dairy products, small portion of red meat, and predominant use of soy oil, did not produce a significant reduction in BP in severely obese individuals (BMI ≥ 35.0 kg/m2) [64].
Plant-Based Diet Components with Hypotensive ActionsVitamin CFruits and vegetables are sources of vitamin C, whose effects on BP have been investigated both in clinical trials and in basic biochemistry experiments. Indeed, there is solid evidence from clinical studies that vitamin C treatment restores endothelial function in patients with coronary artery disease or coronary risk factors [65-67]. Of note, there are at least two meta-analyses [68, 69] that conclude that provision of vitamin C (usually 500 mg/d) significantly reduce SBP and DBP and that this effect is more pronounced in hypertensive patients. Yet, it is unfortunate that the near totality of internists or cardiologists do not prescribe ascorbic acid as supplement.
In terms of mechanisms of action, there is clear biochemical evidence that ascorbic acid stimulates endothelium-derived nitric oxide (EDNO) synthesis [70, 71] and that it does so mainly by increasing the intracellular levels of tetrahydrobiopterin, i.e., the most important cofactor for eNOS activity [72, 70]. Even though ascorbic acid is an important antioxidant [73, 74], it does not affect GSH levels in human aortic endothelial cells (HAEC), and it does not increase the GSH/GSSG ratio. Therefore, based on the literature [72, 71], it is unlikely that ascorbic acid directly improves the intracellular redox environment and, consequently, EDNO synthesis. The most conceivable mechanism of action involves the maintenance or even increase of tetrahydrobiopterin levels by reducing dihydro- or trihydrobiopterin back to tetrahydrobiopterin [75], as also shown by basic experiments in which ascorbic acid was found to stimulate purified eNOS activity directly, despite limiting concentrations of tetrahydrobiopterin and without the contribution of GSH [72]. One caveat is that data obtained from in vitro experiments should be interpreted with caution, as culture media are devoid of vitamin C. Indeed, cultured cells are in scorbutic states [76] and exogenous vitamin C first replenishes their stores and then, eventually, exerts biological effects [77].
A critical issue is that of the optimal dose of vitamin C that augments BP. The only complete pharmacokinetic study carried out with vitamin C is that of Levine et al. [78••], who concluded that vitamin C daily doses above 400 mg have no evident value. Also, a review of over 200 articles on vitamin C and health concluded that a daily intake of 100 mg of vitamin C is associated with lower incidence of heart disease, stroke, and cancer [79]. It should be noted that these amounts (1) are consistent with those reported by Levine et al. to saturate cells [78••]; (2) are consistent with the maximal velocity of the vitamin C transporter [80]; and (3) are achievable through a balanced diet [81]. Indeed, it is worth underscoring that, despite some propaganda on mega-doses, ascorbic acid’s concentrations are tightly regulated in the body [82, 83]. One way to overcome such limitations is to administer vitamin C intravenously [84] in order to reach millimolar plasma concentrations. However, the scant clinical trials of intravenous ascorbic acid for cancer treatment yielded negative results [85] and much more well-performed research on a large number of patients is needed to clarify this issue. However, pertinent to this review, Bruno and colleagues demonstrated that acute vitamin C infusion (3 g i.v. in 5 min) significantly lowers BP in hypertensive patients, but not in normotensive subjects [86]. These data confirm those of Heitzer et al. [87], who reported anti-hypertensive effects vitamin C infusion is smokers (whose endothelial function is notoriously impaired). Hence, there might be room for future high-quality trials in hypertensive patients, even though it might be quite impractical to perform ascorbic acid infusions in an outpatient setting.
In summary, ascorbic acid may play a key role in the plant-based diet beneficial effect on BP. These effects are likely not mediated by redox modulation and involve maintenance of cofactors such as tetrahydrobiopterin [88]. Based on the literature, we advocate the use of vitamin C by clinicians and patients as adjunct therapy of hypertension.
PotassiumPotassium is the most abundant intracellular mineral, and its role in the regulation of BP is well established [89], even if there is no agreement among authors [90]. Unfortunately, the contribution of potassium to the healthful effects of a plant-based diets is often overlooked [91] in favor of, e.g., (poly)phenols (vide infra). However, many vegetables such as green leafy vegetables and some fruits such as bananas are rich in potassium [92], which might at least in part explain [93] why vegetarian diets are associated with significant reductions in BP compared with omnivorous diets [12]. Historically, humans have been consuming quantities of potassium that were much higher than the current ones [94]. Life expectancy was much shorter, but current potassium intakes are often much lower than the recommended levels [95].
The first clinical evidence of the effects of potassium on BP is likely that of WL Addison [96], and some researchers have been investigating the mechanisms of actions that underlie potassium’s BP-lowering activities [97, 93]. One proposed mechanism involves the stimulatory effects of potassium on the sodium–potassium ATPase, which hyperpolarizes cells [98], hence decreasing cytosolic calcium concentrations and leading to augmented vasomotion. Also, potassium has been suggested to directly stimulate EDNO synthesis [99] and increase natriuresis [99, 91, 97] by inhibiting renal sodium reabsorption.
Finally, we propose an indirect effect of high potassium intake, i.e., that high consumption via a plant-based diet largely replaces that of sodium, either as a natural component of meats (especially smoked and cured meats), some comfort foods, e.g., pizza and savory snacks, or added as part of salt to enhance flavor and taste [100].
(Poly)phenolsAs mentioned, nitric oxide synthesis can be modulated by dietary factors [101]. Many constituents of plants and, hence, plant-based diets are non-nutritional compounds that play key roles in plant physiology and interactions with the environment [102, 103]. The most actively studied minor components are (poly)phenols, which have been long investigated for their supposed antioxidant activities. Indeed, there is negative correlation between (poly)phenols intake and blood pressure [104]. Even though research has disproven their direct antioxidant actions, their effects on various enzyme activities appear to be even more interesting in terms of health protection: research in this area should be and, indeed, is further extensively promoted [105].
Among the various biological activities of (poly)phenols, their actions on endothelial function have been researched by various groups. Our own group reported the vasomodulating activities of wild plant extracts rich in (poly)phenols (namely wild artichoke and thyme) in vitro [106] and in vivo [107]. Others studied the vasodilator effects of olive extracts, rich in oleuropein, hydroxytyrosol [108, 109], and hypotensive peptides [110, 111] and used as decoction in folk medicine [112, 113].
As mentioned, direct antioxidant, free radical-scavenging activities of (poly)phenols have been ruled out due to their poor bioavailability and reactivity [114•, 115]. However, in biochemical terms, plasma membrane-associated eNOS is considered to be more constitutively active and extremely sensitive to agonist-induced intracellular Ca+2 fluxes. In addition to post-translational regulatory mechanisms dictating eNOS function, redox changes in the endothelium do indeed modify both enzyme activity as well as EDNO production, in turn adversely affecting vasomotion [116]. As discussed for ascorbic acid, eNOS synthetic activity is dependent on maintaining tetrahydrobiopterin in a reduced state. When the tetrahydrobiopterin/biopterin ratio is high eNOS produces NO, however, when that redox ratio declines, the internal electron transport chain of eNOS becomes uncoupled, which actually generates superoxide anion rather than NO [117]. Thus, in a pro-oxidative milieu [115], eNOS may not only become a target of oxidant species, but also may exacerbate oxidative stress and endothelial dysfunction, hence impairing vasomotion and leading to hypertension. In brief, even though (poly)phenols are not direct antioxidants, they contribute to maintain a proper endothelial redox status and contribute to the hypotensive actions of a fruit- and vegetable-rich diet.
In addition to epidemiological data (often related to the Mediterranean diet [118]) linking a plant-based diet with lower blood pressure [119], some human studies provided direct evidence of the (poly)phenol-induced increase in vasomotion. Three examples are worth mentioning. One is tea, whose intake (chronic or acute) increases flow-mediated dilation (FMD) in healthy subjects and hypertensive patients [120, 121]. The effects are highly likely due to catechin and its derivatives, given the juxtaposition of their plasma kinetics with FMD [
留言 (0)