1. BackgroundSince the outbreak of the SARS-CoV-2 pandemic, the need for the SARS-CoV-2 vaccine has increased to alleviate the number of infections and reduce the severity of the disease [
1]. Many studies have demonstrated the efficacy and safety of SARS-CoV-2 vaccines [
2]. Four types of COVID-19 vaccines are being used worldwide including messenger RNA (mRNA), viral vector, protein subunit, and whole virus vaccines (known as inactivated virus vaccines). The inactivated virus vaccine elicits weaker immunogenicity and lowers clinical protection than the mRNA-based vaccine [
3,
4,
5,
6]. The inactivated viral vaccine (CoronaVac®, Sinovac Biotech) is produced by beta-propiolactone-inactivation of the CN2 strain of SARS-CoV-2 isolated from the patient’s bronchoalveolar lavage, which is closely linked to the 2019-nCoV-BetaCoV Wuhan/WIV04/2019 [
1]. Results of phase 3 trials have shown that the inactivated viral vaccine has a high efficacy rate of 51–84% and a good safety profile [
7,
8,
9]. Glomerular diseases following SARS-CoV-2 vaccines have been periodically reported including minimal change disease (MCD) and IgA nephropathy [
10,
11]. However, only a few cases of de novo or relapsed MN following inactivated viral vaccination have been documented [
12,
13]. A de novo MN with possible relapse stimulated by the second vaccination is reported here. 2. Case Presentation
A 53-year-old male patient presented with intermittent lower extremity edema and foamy urine for 2 weeks, which was spontaneously resolved. He received his first dose of the inactivated SARS-CoV-2 (CoronaVac®, Sinovac Biotech) vaccine a week before the onset of symptoms. He then had his second immunization after 4 weeks from the first dose. He experienced a sudden onset of leg and scrotal edema and puffy eyelids the next day after completing his primary vaccination series. He had abdominal discomfort and gained 5 kg of weight in one week. He denied any symptoms of gross hematuria, headache, or oliguria. Prior to admission, the SARS-CoV-2 virus was not detected by RT-PCR from the patient’s nasopharyngeal swab sample.
On physical examination, the vital signs were as follows: blood pressure 150/90 mmHg and heart rate 68 beats/min. His body mass index was 28.3 kg/m2. He had puffy eyelids without paleness and jaundice. His abdomen was distended with positive shifting dullness. Bilateral leg pitting edema and scrotal edema were also observed. His laboratory tests yielded serum creatinine 1.5 mg/dL, serum urea nitrogen 29 mg/dL, albumin 2.3 g/dL, cholesterol 507 mg/dL, and triglyceride 255 mg/dL. His urinary protein and erythrocytes levels were 3+ and 2+, respectively, and urine sediment depicted 3–5 per high-power field of red blood cells. His urine protein to creatinine ratio was 13.4 g protein per gram of creatinine. Tests for treponemal, HBsAg, anti-HCV, anti-HIV, and antinuclear antibodies were negative. Complement components C3 and C4 were within the normal values. Ultrasonography of the entire abdomen revealed that both kidneys were normal in shape and echogenicity.
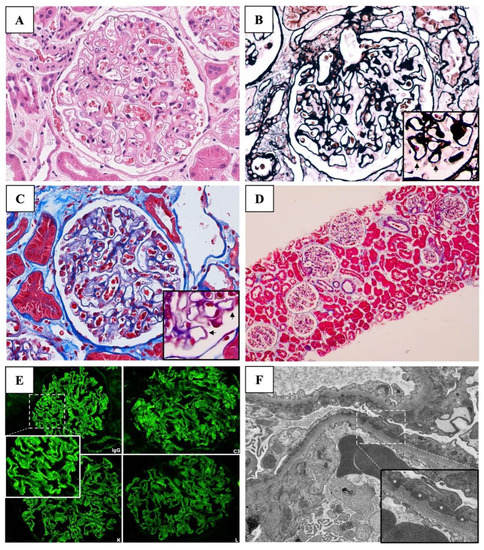
He was clinically diagnosed with an acute onset of nephrotic syndrome (NS) associated with acute kidney injury (AKI). A kidney biopsy was performed, followed by a prescription of daily oral prednisolone at a dosage of 70 mg per day. The kidney biopsy finding showed 20 glomeruli with a normal glomerular basement membrane thickness. No glomerular proliferation and sclerosis were observed. Focal spike formation and scant subepithelial fuchsinophilic granules were detected in the Jones silver and Masson Trichrome stains, respectively, indicating an early stage of membranous pattern on light microscopy (LM). Diffuse interstitial edema was evidenced without accompanying tubular injury and interstitial inflammation. Immunofluorescence staining of 10 glomeruli showed diffuse granular deposition of the IgG (3+), C3 (3+), Kappa, and Lambda light chains (2+) along the capillary wall. MN was diagnosed (
Figure 1).Since the patient was classified as very high risk according to the KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases (accompanying AKI not otherwise explained) [
14], 3-day intravenous methylprednisolone (1 gm/day) was administered, followed by a 1.5-month course of oral prednisolone (0.5 mg/kg/day) and cyclophosphamide (2 mg/kg/day). In week 15, the electron microscopy (EM) report was issued denoting numerous subepithelial electron-dense deposits (EDDs) and a few small deposits in the mesangial, intramembranous, and subendothelial areas, suggesting secondary MN.The serum anti-phospholipase A2 receptor (PLA2R) antibody (Ab) was negative. Other chronic infections and age-related malignancies were excluded. The suspicion of SARS-CoV-2 vaccine-induced secondary MN was raised; therefore, the steroid and immunosuppressive agent were replaced with angiotensin-converting enzyme inhibitors (ACEi). Complete remissions of proteinuria and abnormal kidney function were achieved after 2 weeks of discontinuation of the immunosuppression without subsequent relapses (
Figure 2). 3. Discussion
A case of de novo MN with a possible disease flare or worsening of the clinical expression stimulated by the second vaccination was presented here with a favorable outcome, albeit presenting with AKI. Secondary MN was suspected because of the negative serum PLA2R Ab and the presence of mesangial EDDs. Chronic infections and malignancies had been ruled out. The patient fully recovered after a short course of steroid and immunosuppressive therapy.
Several glomerular diseases have been reported following SARS-CoV-2 vaccination [
10,
11]. The most commonly reported glomerulonephritis (GN) is MCD [
10,
11,
15]. In a recent systematic review of vaccine-induced kidney adverse reactions from 90 case report articles, 134 cases of de novo GN were identified including MCD (52/134, 39%), IgA nephropathy (48/134, 36%), ANCA-associated GN (16/134, 12%), and MN (8/134, 6%) [
16].The mechanism of vaccine-induced MN remains inconclusive [
17]. There is a case report of de novo MN and a case series of MN flares/relapses in patients with autoimmune disease following influenza H1N1 vaccinations [
17,
18]. An immunological response to the vaccination is postulated as the pathogenesis of the MN [
17]. MN has been reported in association with all categories of the SARS-CoV-2 vaccine [
10,
11,
18]. However, the mRNA-based vaccine has the highest number of case reports with vaccine-associated GN compared to the other vaccines, which is consistent with the finding of the highest immunogenicity of the vaccine [
19,
20]. In the systematic review of vaccine-induced kidney adverse reactions, mRNA vaccines contributed to 84% of the vaccine-associated GN cases, followed by viral vector vaccines (13%) and whole virus vaccines (3%) [
16].Recent case reports of de novo MN following vaccination with BNT162b2 (Pfizer-BioNTech) and exacerbation of MN after mRNA-1273 (Moderna) appear to support that vaccination with SARS-CoV-2 triggers MN [
21]. Although the mechanism underlying the association has not yet been well-understood, two possible mechanisms have been proposed to explain how the vaccine may contribute to MN including vaccine-triggering genetically prone primary MN and vaccine-induced cross-immune response (molecular mimicry) [
17,
22,
23]. In addition, numerous autoantibody-driven temporal pathogenesis in SARS-CoV-2 vaccine-associated MN have been postulated including autoantibodies to PLA2R [
10,
11,
12,
24], neural epithelial growth factor like-1 (NELL-1) [
10], and intracellular proteins exostosin 1 (EXT1) [
11]. However, Caza et al. presented cases with negatives of all of these antibodies [
11]. As in the presented case, anti-PLA2R Ab was negative.
Table 1 demonstrates the pooled clinical spectra of SARS-CoV-2 vaccine-associated MN from the published literature. MN can occur after the first or boosted vaccination in both native [
10,
11,
12,
13,
21,
22,
24,
25,
26,
27] and kidney transplant recipients [
28]. Clinical manifestation of MN following SARS-CoV-2 virus vaccination is usually full-blown NS with abrupt onset varying from 1 day to 4 weeks (
Table 1).As in this case, we reported acute onset of 1 week to develop symptoms following the first dose and a few days following the second dose of inactivated SARS-CoV-2 vaccines. The second episode might have resulted from a disease flare stimulated by the second vaccination. The early onset of NS has been mentioned in the passive Hayman nephritis, a classic model of human MN [
29]. The MN is induced by a single injection of heterologous antisera to the rat renal tubular antigen extract in susceptible rat strains [
23]. Massive proteinuria occurs in almost all animals within 5 days, followed by low-grade proteinuria lasting 60–150 days [
23]. The onset of massive proteinuria is diminished by 2–3 days if the Ab is boosted [
23]. Zhao et al. also demonstrated the occurrence of de novo MN immediately following immunization with the inactivated SARS-CoV-2 vaccine, and the NS entered partial remission after receiving angiotensin II receptor blocker treatment [
13]. In the presented case, the abrupt onset of the NS was consistent with the early stage of membranous lesions through LM (focal spike formation) and EM (no membrane reaction).The theory of vaccination triggering MN flare is supported by a retrospective study of 245 patients with biopsy-proven MN from a single center. The relapse rate of MN occurred at 5% during the SARS-CoV-2 pandemic era compared to 2% prior to the era [
21]. However, the causal relationship of these findings needs further examination [
11,
30].Treatment of secondary MN following SARS-CoV-2 vaccination is controversial. Based on the evidence of primary MN, conservative treatment and immunosuppressive medication are therapeutic options. Rituximab, obinutuzumab, mycophenolate mofetil, and oral cyclophosphamide have been used to reach partial response outcomes [
10,
19,
21,
24,
25,
26,
27]. The patient achieved complete remission without subsequent second relapse after the short course of immunosuppressive agents, suggesting a causal relationship between the vaccination and secondary MN. Close monitoring of GN relapse after a booster dose of SARS-CoV-2 vaccination is warranted since the same type of vaccine might exacerbate the immunologic response [
13,
25].
In conclusion, secondary MN following SARS-CoV-2 vaccination should call for medical importance. Not only is it spontaneous remission or remission despite a short course of immunosuppressant, but also a high index of suspicion of the association might avoid unnecessary treatment with long-term steroid and immunosuppressive agents. Therefore, further investigation into the pathogenesis is warranted.
Table 1.
Clinical spectra and outcomes of membranous nephropathy following SARS-CoV-2 vaccination.
Table 1.
Clinical spectra and outcomes of membranous nephropathy following SARS-CoV-2 vaccination.
No.StudyAgeGVaccine TypeDoseOnsetSerum
Albumin
(g/L)Serum
Creatinine
(mg/dL)Hematuria
(/HPF)Proteinuria
(g/g Creatinine)De Novo/
Relapse
GNType of MNTreatmentOutcome1.This case53MSinovac2nd 1 d2.31.53–5 13.4De novoNeg only PLA2RGC, CY 3 mo.Response2.Aydin [
12],
202166FSinovac1st 2 wk2.62.78N/A9.42RelapsePLA2RN/AN/A3.Caza [
11], 202154MModerna2nd 1 d3.41.3Pos3+De novo1 PLA2R, 1 EXT, 1 neg PLA2R/
EXTGC
RituximabNo response4.68MJ + J1st <4 wk3.23.3Neg0.6De novoConservativePartial response5.47MModerna2nd 6 d2.30.7Pos2.7De novoNonePartial response6.Klomjit [
10],
202150FPfizer2nd 4 wk3.50.73–106.5De novoNELL-1ConservativeResponse7.39MPfizer2nd 1 wk21.133–108.7RelapsePLA2RTACResponse8.70MModerna2nd 4 wk2.72.1<316.6RelapsePLA2RObinutuzumabN/A9.Gueguen [
25], 202176MPfizer
Moderna1st
2nd 4 d
N/A1.6
2.20.86
1.15Pos
N/A6.5
3.8De novo
RelapsePLA2R
N/AConservative/RituximabPartial response10.Da [
31], 202170MPfizer1st 1 wk1.71.29N/A4.4De novoTHSD7AConservativeNo response11.Liang [
32], 202162FModerna2nd 1 moN/A1.6N/A11.2RelapsePLA2RConservative/RituximabN/A12.Chavarot [
28],
202266MPfizer2nd 8 wkN/A1.36N/ANegDe novo post-KTPLA2RConservativeN/A13.Psyllaki [
24],
202268MPfizer1st 7 d2.9GFR 70 mL/min/1.73 m2N/A19De novoPLA2RRituximabPartial response14.Fenoglio [
22],
202282FPfizer2nd 88 dN/AN/AN/ANSDe novoNeg PLA2R, THSD7AGCN/A15.67FPfizer2nd 89 dN/AN/AN/ANSDe novoNeg PLA2R, THSD7ARituximabN/A16.82MPfizer2nd 29 dN/AN/AN/ANSDe novoPLA2RRituximabN/A17.Rashid [
27],
202256MModerna1st 4 wk2.213.96Blood 2+12.2De novoPLA2RHemodialysis
RituximabResponse18.Visch [
21],
202280MPfizer2nd 4 wk2.61.32N/A5RelapsePLA2RRituximabNo response19.60MPfizer2nd 6 wk1.71.92N/A5RelapsePLA2RRituximab/CY/
GCResponse20.77FPfizer1st 4 wk2.20.7N/A12.5RelapsePLA2RTacrolimusResponse21.78MPfizer2nd 1 wk3.41.87N/A4.9RelapseN/AGCResponse22.48MPfizer2nd 3 wk3.11.41N/A1.7RelapsePLA2RConservativeNo response23.56MPfizer2nd 2 wk3.21.47N/A3.4RelapsePLA2RConservativeNo response24.84MPfizer2nd 10 wk3.31.55N/A3RelapsePLA2RTacrolimus/GC→ RituximabResponse25.39MPfizer2nd 4 wk1.81.38N/A3.7De novo
WorseningPLA2RRituximab/CY/
GCResponse26.75MPfizer2nd 2 wk2.10.88N/A8De novo
WorseningPLA2RRituximab/CY/
GCN/A27. 48MPfizer1st 2 wk2.51.26N/A2.22De novo
WorseningPLA2RRituximab/CY/
GCResponse28.58MPfizer2nd 3 wk2.41.02N/A8De novo
WorseningPLA2RTacrolimusResponse29.Zhao [
13], 202257WSinovac1st
2nd 1 d
1 dN/A
2.85N/A
0.42N/A
1+N/A
1.6De novo
RelapsePLA2RConservativePartial response30.Paxton [
26], 202222MPfizer2nd 4 wk80.72N/A7De novoPLA2RRituximabPartial response31.Saigal [
33], 202232MAstra ZenecaN/A14 dN/AN/AN/AN/ADe novoN/AGC/CYPartial response32.47MAstra ZenecaN/A11 dN/AN/AN/AN/ADe novoN/AConservativeResponse32.Pitre [
34], 202265FJ + J1st 5 moN/A1.7N/A1.7De novoPLA2RGCPartial response33.Ma [
19], 202242FAstra Zeneca1st 2 wk1.60.8N/A16N/AN/AGC/MMFResponse

留言 (0)