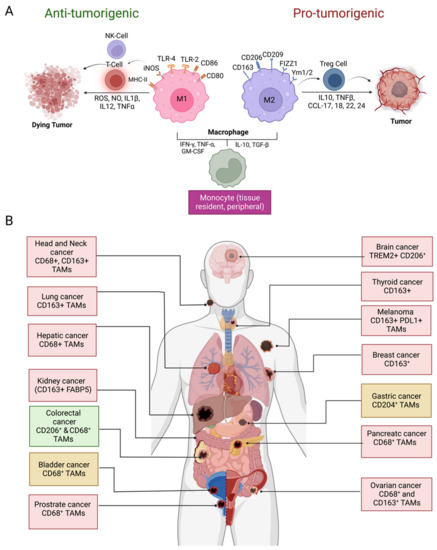
Cancer biomarkers help in characterizing alterations in the tumor. A number of genes associated with lymphocyte regulation, cytokine signaling, lymphocyte markers, checkpoint pathways, and tumor characterization have been identified as a predictive biomarker for cancer. The majority of tumors show evidence of a T-cell-infiltrated phenotype. TME and the immune system play critical roles in cancer progression and clinical outcome where regulatory (Treg) and effector T cells’ infiltration contributes to the maintenance of self-tolerance and an immune-homeostasis-creating immunosuppressive environment by suppressing antitumor immunity in the TME. T-cell-inflamed TME is characterized by the elevated expression of type 1 interferon, as well as promigratory chemokines that result in the recruitment of activated CD8+ effector T cells into the tumor parenchyma [
30]. Anticancer can be segregated into three main phenotypes: the immune-excluded phenotype, the immune-desert phenotype, and the inflamed phenotype. An immune-excluded tumor represents a specific chemokine state that is characterized by the presence of different immune cell types in the aggressive margin or stroma of the tumor but cannot infiltrate into the tumor parenchyma [
31,
32]. On the contrary, the immune-desert phenotype is caused by immunological ignorance, which is characterized by the absence of appropriate T cell priming or activation in the parenchyma or stroma of the tumors and poor response to immune checkpoint inhibitors treatment [
33,
34]. Inflamed tumors are highly infiltrated with number of immune cells subtypes, including immune-inhibitory regulatory T cells, myeloid-derived suppressor cells, suppressor B cells, and cancer-associated fibroblasts. It contains proinflammatory cytokines that should provide a more favorable environment for T cell activation and expansion [
35]. Therefore, utilizing the role of cytotoxic T cells to kill cancer cells can be an effective immunotherapy. The presence of activated CD8+ T cells, both within the tumor and in the peritumoral stroma, has been shown to have significant positive prognostic import [
36,
37]. A high ratio of CD8+ T cells to Foxp3+ regulatory T cells (Treg) in the ovarian cancer tumor microenvironment has been associated with a particularly favorable clinical outcome [
38]. A study was conducted to identify factors associated with success or failure of checkpoint therapy, in which they performed transcriptomes analysis in immune cells from tumor samples of melanoma patients treated with checkpoint therapy (anti-PD-1, anti-CTLA4+PD-1, and anti-CTLA4). Their results highlighted how the transcription factor 7 (TCF7) is selectively expressed in memory-like T cells, which is a top marker associated with responding lesions. It is a part of the Wnt/β-catenin signaling involved in the differentiation, self-renewal, and persistence of memory in CD8+ T cells. Next, they determined the states of immune cells by applying high-dimensional single-cell RNA sequencing (scRNA-seq) because the association of T cell states with clinical responses is well established. They found more TCF7+CD8+ cells in responding samples, whereas more TCF7−CD8+ cells were in non-responding samples, which suggests the ratio of CD8+TCF7+ to CD8+TCF7− tumor-infiltrating lymphocytes is strongly correlated with improved response and survival in melanoma patients treated with anti-PD-1 [
34,
39]. Tumors showing a high expression of PD-L1 and indoleamine-2,3-dioxygenase (IDO) display an increased percentage of CD4+CD25+Foxp3+ Tregs cells [
40,
41,
42]. Spranger et al. suggested that upregulation of PD-L1 and IDO is driven by IFN-γ produced by CD8+ T cells in vivo. Furthermore, the accumulation of Treg cells is also CD8+ T cell-dependent through the production of the chemokine CCL22 via CCR4 [
43,
44]. A study conducted by Balatoni et al. on surgical tissue samples from 30 patients with metastatic melanoma treated with ipilimumab evaluated the prognostic and predictive associations of immune cell infiltration and overall survival after treatment. A higher prevalence of several immune cell types including CD4+, CD20+ B cells, CD134+ and CD137+ cells, and NKp46+ cells was seen, particularly FOXP3+ cells and CD8+ T lymphocytes [
34,
45].A substantial body of evidence suggests that NK cells contribute to host control of hematologic malignancies and contribute to tumor control in solid tumors [
44,
46,
47]. Association between TAMs and anti-PD-1 response has been reported in melanoma cases. It has been established that the association between Fcγ receptor (FcγR), expressed by the host bone marrow cells and Fc domain glycan of the drug, could determine the ability of PD-1-TAMs to capture anti-PD-1 drugs from the surface of T cells, leading to PD-1 inhibitor resistance [
48,
49]. In addition, anti-PD-1 response also affect cytotoxic T cells, indicating an increase in CD8+ T cells and NK cells and a decrease in macrophages [
34,
50,
51].Recently, a study conducted by Crist et. al. has shown that the antidiabetic agent metformin slows tumor growth and progression in vitro and in combination with chemoradiotherapy in patients suffering from head and neck cancer squamous cell carcinoma (HNSCC) in their phase 1 clinical trial (NCT02325401). It increases the activated peripheral NK cell populations, enhanced HNSCC NK cell cytotoxicity, and inhibited the CXCL1 pathway while stimulating the STAT1 pathway [
52]. It also influences anticancer immunity in esophageal squamous cell carcinoma (ESCC) in both humans and mice, via triggering an AMPK activation and STAT3 inactivation. In clinical trials, low-dose metformin recruits a greater number of CD8+ cytotoxic T lymphocyte and CD20+ B lymphocyte while enhancing tumor-suppressive (CD11c+) and reducing tumor-promoting (CD163+) macrophages in TME [
53]. In addition to this strategy, mannose-modified, macrophage-derived microparticles (Man-MPs) loading metformin (
[email protected]) were used to effectively target M2-like TAMs to transform them into M1-like phenotypes. This strategy reprogrammed the TME towards an inflamed anti-tumor microenvironment by increasing the recruitment of CD8+ T cells. The
[email protected] approach boosted the anti-PD-1 antibody therapy and developed long-term memory immunity [
54]. Interestingly, the anti-tumor efficacy of the PD-L1 depression strategy was found to be superior to the conventional anti-PD-L1 therapy in terms of selectivity and efficacy. This group has developed a mitochondria-oxidative phosphorylation (OXPHOS) depression nanosystem using IR-LND (conjugate of mitochondria-targeted heptamethine cyanine dye IR-68 with mitochondrial complexes I and II depression agent lonidamine (LND)) assembled with albumin (Alb) to form
[email protected] nanoparticles [
55]. Another promising therapy that has the same limitation of causing severe hypoxia and PD-L1 over-expressed immunosuppressed TME is photodynamic therapy (PDT). A recent study had constructed a
[email protected]@MnO2 nanoparticle system to depress the PD-1/PD-L1 axis with two-step oxygen regulation, where Buformin (Bu, an OXPHOS disrupting agent with PD-L1 depression and oxygen reversion ability), and methylene blue (MB) as a PDT drug with PD-1 inhibition capacity were composed with manganese dioxide albumin (
[email protected]) as a carrier of this nanosystem. This resulted in selective delivery to tumor tissues and enhanced T cell infiltration and improved its tumor cell-killing ability, reverting the immunosuppression [
56]. PDT not only induces ROS production to damage tumor cells but also promotes the antitumor immunity of T cells through stimulating the production of IFN-γ. Therefore, another composite of metformin (Met) and IR775 in liposome (
[email protected]@Lip) had been studied to solve this problem. The
[email protected]@Lip was found to reverse tumor hypoxia by enhancing ROS production to elicit more damage and downregulate PD-L1 [
57].
In conclusion, targeting immune cells in TME could be a great predictive biomarker for immune checkpoint inhibitors.

留言 (0)