After observing a reduced incidence of COVID-19 in countries continuing universal tuberculosis prophylaxis, various studies were initiated to confirm this hypothesis. The results of studies from different centres are not conclusive, nor is the methodology of the analyses performed.
Weng et al. [
5] studied a cohort of 120 adult patients with COVID-19 in March and April 2020. Eighty-two patients (68.3%) were vaccinated with BCG, and this group had a lower risk of hospitalisation (p = 0.019). However, the authors did not assess anti-SARS-CoV-2 antibody levels, so we cannot directly compare our results with this outcome. In addition, in the above study, people who had never been vaccinated with BCG were present, which is a significant difference.Amirlak et al. [
15] conducted a study in which 280 healthcare workers were offered BCG immunisation. All 280 had been previously vaccinated against tuberculosis; of this group, 71 received an additional dose, and 209 did not. During a follow-up of more than three months, the authors recorded 18 cases of SARS-CoV-2 infection among hospital staff. All cases were in the group that did not receive an additional dose of the BCG vaccine. The authors showed statistical significance, but, as in the work of Weng et al. [
15], antibody concentrations were not assessed here [
15]. Despite the similar age and the population being previously vaccinated with BCG, we cannot compare the results of our serological assessment. Khanum et al. [
16] conducted an observational study on adult participants with a positive polymerase chain reaction (PCR) test for SARS-CoV-2. The study evaluated 103 patients with COVID-19, of whom 64 participants had previously received BCG vaccination (scar-based assessment), and 39 had not been vaccinated against TB. The authors did not demonstrate statistical significance in terms of the severity of the COVID-19 disease in the groups compared. Still, the previously vaccinated group showed significantly lower mortality than previously unvaccinated patients [
16]. We did not evaluate COVID-19 mortality in our study. The different nature of the evaluation—observation of patients with the disease rather than a randomised clinical trial with vaccine administration—also differs from our work in the cited study. Consequently, it is difficult to predict what such a finding would look like in our study population.In another multicentre observational study, Torun et al. [
17] analysed 465 healthcare workers with SARS-CoV-2 infection for a history of contact and exposure to Mycobacterium tuberculosis. The authors showed that the hospitalised study participants had a history of direct contact with tuberculosis patients. In addition, a higher number of working hours in the hospitalised participants was proven. On the other hand, only one person in the study population died due to COVID-19, so the overall mortality rate was low. Such results can probably be linked to the process of ‘trained immunity’, which is influenced by BCG vaccination and perhaps also by direct contact with TB. On the one hand, ‘trained immunity’ enhances the anti-viral response, but, on the other hand, it may stimulate a Th1/Th17-type inflammatory response and generate severe COVID-19 disease symptoms [
18]. The results of the above-cited study could correspond to such a process, but the limitation here is that the study is observational in nature rather than a randomised clinical trial. The authors did not analyse the concentration of antibodies in the participants, either. For these reasons, it is also difficult to directly compare the results of Torun et al. with our study.The results of Rivas et al. [
19], who analysed more than 6000 healthcare workers for BCG vaccination, are different. They also determined IgG-class anti-SARS-CoV-2 antibody titres. A total of 29.6% participants were vaccinated, while 68.9% were not. The reporting of COVID-19 disease symptoms and seroprevalence based on the determination of anti-SARS-CoV-2 antibody titres was significantly lower in the BCG-vaccinated group of medical workers compared to the unvaccinated group. The authors additionally analysed the study participants regarding vaccination against Neisseria meningitidis, Streptococcus pneumoniae and influenza, but did not find any comparable results [
19]. In the above study, some characteristics are similar to ours, such as the participants’ mean age and profession. However, this is not a randomised clinical trial but a retrospective clinical study. In addition, given the different vaccinability of the population, it can be concluded that our results are entitled to differ from those of Rivas et al.The nature of the study by Tsilika et al. [
20] is much more similar to ours compared to the previously cited work. The authors conducted a randomised, double-blind clinical trial on 516 elderly participants (median age 68 years). Ultimately, 301 participants received BCG or a placebo, and the follow-up period was six months. Re-vaccination with BCG reduced the risk of COVID-19 to 68%. In addition, the authors collected blood from 300 participants 3 months after vaccination to assess SARS-CoV-2 antibody levels to detect those who had undergone asymptomatic infection. A positive serological result was obtained in 1.3% (2/153) of the subjects in the placebo group and in 4.7% (7/148) in the BCG group, which was not statistically significant (p = 0.099). A randomised clinical trial was used in the above study, as in ours. The study participants were also previously vaccinated with BCG due to Greece’s vaccination policy. They were not healthcare workers, but, as in our case, no statistical significance was shown. The authors did not analyse other characteristics, such as age or gender, in relation to antibody concentrations, so it is difficult to compare our overall results with the paper mentioned above.Uysal et al. [
21] conducted a study to evaluate the serological response after COVID-19 vaccination in healthcare workers, analysing factors such as age, gender, smoking habits, and BMI. The authors only showed a statistically significant difference for smoking, with higher antibody titres obtained in non-smokers. However, no significance was shown in the other parameters, as in our study. Nonetheless, the above study did not assess the effect of BCG vaccination on COVID-19 or serological response.A study relatively similar to ours was performed by Dos Anjos et al. [
22], who conducted a single-centre clinical trial of healthcare workers with revaccination with the BCG Moscow strain. Although the authors presented a reduction in the incidence of COVID-19 in the vaccinated group in their results, they did not reach any statistical significance. However, a placebo was not used in this study. An additional significant difference from our trial was that the participants included in the analysis worked at least eight hours per week in direct contact with patients suspected of COVID-19. Therefore, our results cannot be directly compared.A multicentre clinical trial with placebo control was conducted by Jalalizadeh et al. [
23] on a group of 378 adult patients, not medical professionals but people recovering from the COVID-19 disease. The participants in the BCG group had a greater return of smell and taste within six weeks of follow-up compared to the placebo group. In addition, a reduced risk of ageusia in the following weeks was shown among those vaccinated with BCG. However, these data do not correlate with ours due to the different participant profiles and the nature of the study. In a similar study, Dionato et al. [
24] assessed the safety of BCG revaccination in patients in recovery from COVID-19, finding no adverse effects, and additionally showing a faster return of the sense of smell in the vaccinated group.Moorlag et al. [
25] conducted a randomised trial in elderly patients (>60 years of age) with BCG and a placebo. They focused on assessing the total incidence of respiratory-tract infections requiring medical intervention. BCG did not affect the incidence of infections, including COVID-19, but it is worth noting that, in patients diagnosed with the SARS-CoV-2 infection, antibody titres were higher if the participant had previously received BCG. This result differs from our study, but this was not the authors’ primary aim, unlike in our team. The humoral response and antibody production after COVID-19 infection and the impact of BCG require further study.Another interesting study was conducted by Ten Doesschate et al. [
26]. This was structurally similar to ours: a multicentre clinical trial of healthcare workers randomised 1:1 with BCG and placebo. However, the main difference was in the characteristics assessed; the authors analysed the number of days of absenteeism from work without showing statistical significance. In our study, we did not consider such a parameter at all.A study to evaluate the efficacy of BCG on COVID-19 in a group of adult patients with type I diabetes was conducted by Faustman et al. [
27]. In the BCG-vaccinated group, participants had a lower incidence of COVID-19 and infectious disease symptoms, and lower titres of IgG antibodies to SARS-CoV-2 than the placebo group. However, the promising results of the study only apply to one population, and, in addition, one with a high-risk: Type I diabetes. In our trial, we did not analyse participants by additional comorbidities, but by their profession, age, gender, or BMI [
13].The most similar study to ours was the Australian population trial conducted by Pittet et al. [
28]. This study is also a multicentre phase III clinical trial in which participants —healthcare workers—were randomised in a 1:1 ratio, with one group receiving the BCG vaccine produced in Denmark together with the influenza vaccine, and the other group receiving the influenza vaccine alone. Participants were assessed for a total of 12 months for the frequency and severity of the SARS-CoV-2 virus infection, and, as in our study, blood samples were taken from them to assess antibody levels. Unfortunately, the results of this study, which could be a precious reference to compare to our results, have not been published so far.In the discussion on the current state of knowledge, it is also worth having a look at the comment by Netea et al. [
29]. They highlighted the incomplete status of knowledge on the effect of BCG vaccination on the course of the COVID-19 disease and the need to publish the results of randomised clinical trials. They also mentioned that some studies suggest the efficacy of the BCG effect when the vaccine was administered after birth instead of as revaccination already during the pandemic.
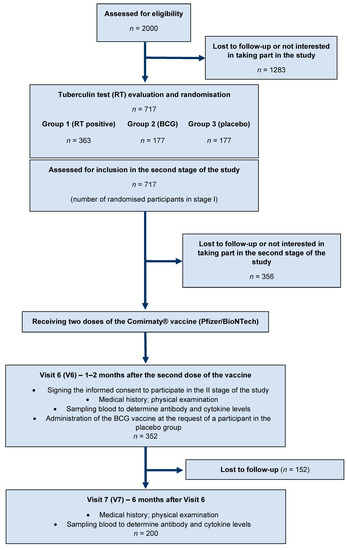
Our study was not without limitations. Primary among these was the lack of baseline antibody concentrations upon vaccination for SARS-CoV-2, which, however, was not the original project assumption. Perhaps because of this, it was impossible to demonstrate relevance in the context of vaccination and the period since the second dose of the vaccine. Another limitation of our study was the lack of a control group, never vaccinated. In the study population, participants received at least two doses of the BCG vaccine, as BCG prophylaxis has been mandatory in Poland since 1955. This fact probably hindered the evaluation and contributed to this result. It is also worth mentioning that the evaluation of antibody concentrations we carried out was of a scientific nature, with no intention of making specific recommendations in practice.
Due to the lack of published results from analogous studies, it is challenging to conclude conclusively whether BCG revaccination can help control the SARS-CoV-2 coronavirus pandemic or reduce the severity of COVID-19. It is also difficult to compare our serological results with other studies, as their different methodologies do not allow complete translation of the results. Further research on the effect of BCG on the coronavirus disease is necessary, not least because of the possible use of this vaccine as an additional tool against a pandemic. This is especially relevant for developing countries, where the availability of SARS-CoV-2 vaccines, as well as storage capacity, is limited.

留言 (0)