1. IntroductionThe main objective of vaccination is to promote an efficient protective immune response against a targeted pathogen to reduce the risk of developing the disease or its complications [
1,
2]. Various vaccines can prevent over 30 infectious diseases with excellent safety profiles and producing effective and robust immunogenicity [
3]. Together with water purification, vaccines have been considered one of the best strategies to reduce morbidity and mortality, and are even more effective than antibiotics [
3,
4] for immune-preventable diseases.In the last decade, the World Health Organization (WHO), the Pan American Health Organization (PAHO) other entities responsible for public health have vaccinated more than 1 billion children, annually preventing 2 to 3 million deaths. However, despite efforts on national and international levels, it is estimated that 19.7 million children under one year of age have not received essential vaccines administered during this period of time [
5,
6], and at least 1.5 million children under five years old die annually because of immune-preventable diseases due to lack of access to fundamental childhood vaccines [
7].Ecuador has experienced difficulties in attempting to comply with the vaccine global action plan established in 2020, whose main objective was to reach national coverage of 90% [
6]. Not only was this goal missed in Ecuador, but according to the evaluation of the immunization strategy of the Ministry of Public Health (MSP, 2017), the proportion of the 2016 vaccinated population is actually lower when compared to 2013 for all the vaccines presented in this
Table 1. Furthermore, the data for 2019 were not encouraging, showing stagnation, and even further decreases in some specific vaccines (
Table 1) [
6,
8,
9,
10]. These trends are worrying, and it remains unresolved why vaccination rate continues to drop.Historically, in the capital city of Quito, Ecuador, childhood vaccination coverage has never surpassed 80%; the last report for 2018 describes coverage up to 79% [
9,
11]. Missed vaccination opportunities appear to significantly contribute to these low values, which occur in instances when a child who is eligible for vaccination, and has no contraindications, visits a healthcare service and does not receive all the recommended vaccine doses [
12]. Health caregivers’ refusal to vaccinate, or inadequate or absent advice from health personnel contribute to the problem of missed vaccinations [
13,
14]. Even rescheduling or postponing vaccinations can result in a lost opportunity to immunize, due to geographical distances between patients and healthcare providers, exasperated by insufficient transport availability, resulting in incomplete immunization schedules [
15].Health personnel oversee administering vaccines and resolving questions or uncertainties related to immunizations within the community. A misinterpretation of vaccines’ indications and contraindications can lead to missed immunization opportunities or unnecessary delays [
16,
17]. Our objective was therefore to understand the current state of physicians’ understanding related to vaccines, in order to determine if the low vaccination rates in the Metropolitan District of Quito could be attributable to unnecessarily missed opportunities, rather than other impediments, such as the inability of patients to reach vaccination points. A more thorough assessment of physicians’ knowledge related to the true contraindications of vaccinations in the capital city is an essential first step if there is to be hope of increasing vaccination coverage of the Ecuadorian population. 2. Materials and Methods 2.1. Study Design
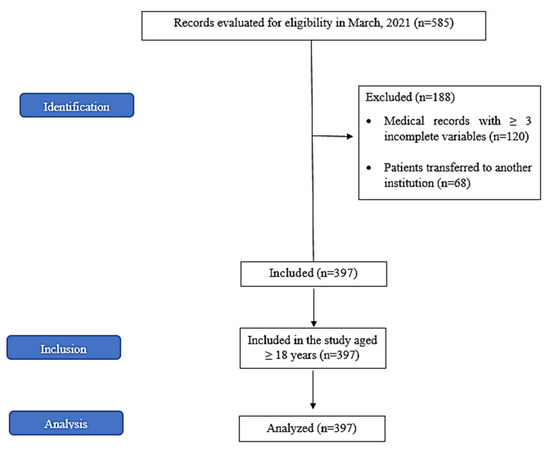
We present a preliminary descriptive, observational, cross-sectional study to meet the proposed objectives. The study was conducted from September to December 2020 in the Metropolitan District of Quito (Quito canton). Participants responded to an online questionnaire sent through all available institutional mails for health personnel from public and private entities.
This questionnaire was sent to the health personnel (specialist doctors, general practitioners, and nursing staff) of primary public health care and the pediatric doctors affiliated with the Ecuadorian society of pediatrics affiliate Pichincha. In total, 626 surveys were sent throw institutional mail, of which 275 replies were obtained, with 273 voluntarily agreed to conduct this questionnaire, and two replies declining participation, leading to a response rate of 44%.
2.2. Data/Measurement SourcesA questionnaire was developed based on the one used by Rivero et al., which tested different scenarios of actual contraindication vaccination knowledge. We created 18 scenarios adapted to Ecuador’s vaccination scheme [
18], which was prepared electronically in the Office 365 program Microsoft Forms©. The survey consisted of scenarios that tested the knowledge of health personnel about vaccination contraindications where each scenario had three response options: vaccinate, do not, or postpone vaccination. All the items in the survey did not constitute a contraindication to vaccination. 2.3. Control of Sources of Bias
Due to the pandemic, primary care personnel shifted employment and subsequently and institutional address, hindering our ability to personally distribute the survey, which could have resulted in a lower response rate than expected.
2.4. Study Size
The sample size was not calculated since it was a non-probabilistic sample, which included all the participants who voluntarily agreed to take the questionnaire.
2.5. Statistical Methods
The data were managed through the statistical program R studio version 1.4.1106, through which it was tabulated, and descriptive statistical analyzes of central tendency and frequency analysis were performed. The ggplot2 package of the R studio program was used for the exploratory study.
3. Results
Replies were obtained from 275 participants, of which 273 (99.3%) voluntarily agreed to carry out this questionnaire, and 2 (0.7%) replied that they declined to participate. Of the participants who answered the survey, 202 (74%) belonged to the public health network and 71 (26%) to the private service.
Specialist doctors predominated the responses of those who agreed to participate in the survey (34.4%, n = 94). Among those, 62 belonged to private healthcare facilities and 32 to the public healthcare system. Nursing personnel constituted 31.2% (n = 85) of replies and were limited to members of the public healthcare system. General practitioners 24.9%, (n = 68) were distributed in the public system (n = 60) and in the private system (n = 8). Finally, primary health care technicians 9.5% (n = 26).
Nearly all medical professionals surveyed (98.2%, n = 268) had denied vaccination at least once in the questionnaire. Surprisingly, among all participants only five respondents (1.8%) answered the entire questionnaire correctly, vaccinating in all presented scenarios, indicating high rates of incorrect rejections for possible vaccinations.
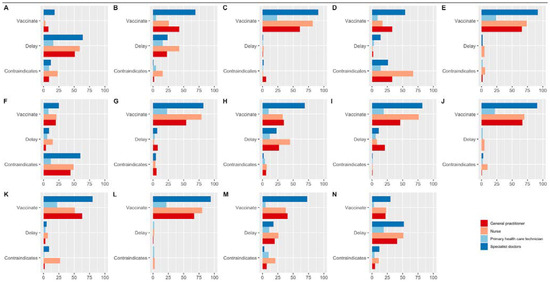
Of the scenarios we proposed in the survey, many respondents responded that they would delay vaccination in children with fever (89%, n = 243) (
Table 2). Regarding the use of drugs, over half of the respondents decided to vaccinate children receiving antibiotic treatment, 52.4% (n = 143). Conversely, 71.4% (n = 195) indicated they would not recommend immunizing a child who was on steroid therapy.Health personnel decided to deny vaccination (72.9% n = 199) in children with autoimmune diseases such as agammaglobulinemia, for vaccinations against chickenpox. Similarly, a slight majority of the respondents (58.6%, n = 160) declined vaccination of the triple viral (measles, mumps, and rubella) for patients with egg allergies. Further specific instances are illustrated in
Table 2 and
Figure 1. 4. DiscussionChildhood vaccination coverage in Ecuador has lagged both national and international goals for 2020. Rectifying any instances where vaccinations are improperly rejected could assist in reducing children’s morbidity and mortality. Vaccines are estimated to prevent almost six million deaths/per year and to save 386 million life years and 96 million disability-adjusted life years (DALYs) globally [
19].One of the leading causes for Ecuador’s failure to achieve the desired vaccination coverage could be due to missed vaccination opportunities. These missed opportunities often occur when a patient without contraindications postpones, or never receives the corresponding immunization. This problem is not novel, in fact it has been described frequently in low- and middle-income countries [
15]. Several reviews suggest that when health personnel misinterpret a vaccines contraindication, these errors could lead to improper postponement or vaccination denial [
20,
21]. According to Tampi et al., missed vaccination opportunities can vary greatly, but total from 5% to 37% of vaccination opportunities in Latin America [
22]. Gaps in the healthcare provider’s knowledge, as well as their attitudes and behaviors related to vaccine contraindications, and patient communication skills with diverse healthcare teams are thought to be responsible for these reductions in vaccination opportunities [
20,
22]. Jimbo-Sotomayor et al. reported a study on 368 children from Quito, illustrating that 33.4% had an incomplete vaccination scheme and only 44.7% of those able of being vaccinated were indeed immunized [
23]. The actors responsible for not vaccinating these youth were attributed to the parent or caregiver (76.2% of cases) as well as health personnel (19%). Although parents/caregivers in this study represent a larger proportion of decision-makers. Yet these missed opportunities for vaccinations equally can occur when healthcare professionals provide misinformation to caregivers or parents, as well as when physicians or medical professionals erroneously deny or postpone vaccinations [
13,
15,
23]. Therefore, understanding under which circumstances healthcare professionals inaccurately reject or delay is vital to increasing vaccination rates. Mild fevers were one of the main scenarios which were regularly misinterpreted by health personnel as a contraindication for immunization. It is common for health personnel to postpone vaccination when a patient presents with a mild fever (≦38 °C) or in case of a mild infection that present a mild fever, despite the fact both scenarios there is no evidence to consider it as a contraindication for vaccination [
21,
24,
25]. This misunderstanding is not unique to Latin America, it has been also reported by Rivero et al. where 77% of European healthcare providers delayed or refused vaccination due to mild fever. In our study, a similar percentage (69.6% of health workers) recommended postponing vaccination, and 19.4% considered not vaccinating a patient with a mild fever. Postponing vaccination may be justified if the patient has a serious disease (e.g., severe infection), if the objective is to avoid incorrectly attributing fever symptoms to the vaccine; however, it does not justify denying vaccination in all cases of mild fever where a physical examination shows no indication of pathology [
18,
24,
25].The use of medications as a justification for not vaccinating Is a frequent stigma that health personnel must resolve; among the most common are when patients are taking antibiotics and/or steroids. It is generally accepted that the use of antibiotics has no effect on the immunogenicity of the vaccine, nor does it cause any adverse effects [
24,
25]. While most health workers (52.4%) in our study decided to vaccinate children taking antibiotics, 47.6% unnecessarily delayed or denied immunization, suggesting misinformation or ignorance of established guidelines, likely resulting in potentially unvaccinated patients. Like antibiotic treatments, the use of low-dose steroids is not a reason to postpone immunization [
25]. Our result suggests that most health personnel similarly delay vaccination when patients are on steroid medications. The history of preterm labor can ”e pe’ceived as a precaution but not a contraindication when it presents associated disorders such as heart disease, bronchopulmonary dysplasia, neurological disorders, recurrent infections, apnea, and chronic pharmacological therapies [
24,
25]. Therefore, the scenario we presented to respondents did not contraindicate immunization. Yet 12.5% of medical professionals opted to postponed, and 60.4% of the participants contraindicated vaccination, suggesting significant ignorance of vaccine contraindications in a patient with immune alterations.Most of the severe reactions after administration of the MMR vaccine (measles, mumps, and rubella) occur in children who are not allergic to eggs. These vaccines are produced in chicken embryo fibroblasts, not eggs [
25]. Therefore, the MMR vaccine is just as safe as any other vaccine, is not contraindicated by egg allergy, and can be administered routinely without preliminary testing, like for the influenza vaccine. However, in our sample, 51.3% of the health personnel contraindicated the MMR vaccine administration [
24,
25,
26]. Although nearly 60% of the respondents’ state that they know that immunization can be administered, a significant percentage of respondents still decided to postpone or deny vaccination, which could result in vaccination opportunity loss as Ecuador has rural and urban regions, many of them with geographical barriers that make it challenging to comply with the vaccination schedules.
In this study, most participants were health workers from primary care centers in the public system. Being a preliminary study and with a small sample of participants and from a single city in Ecuador, we acknowledge albeit likely, we cannot generalize the results at the national level. We highlight that all health personnel, especially those on the first line of care, should possess up-to-date knowledge of vaccines, regardless of profession or specialization. The specialist doctors and/or nurses applying vaccines must specifically have standardized knowledge related to specific vaccinations and their respective contraindications. It is possible that many healthcare workers may not be directly in charge of the child’s immunization, still, they are important sources of information to parents and caregivers, and can spread the disinformation related to contraindications. Together this misinformation can result in lost vaccination opportunities, resulting in suboptimal vaccination status in Quito, and perhaps nationally. On the other hand, the lack of clear practice guidelines on vaccines could cause health personnel to make individualized decisions, giving rise to significant discrepancies in the application of immunizations among medical personnel. Institutional regulations and adequate and up-to-date information on the indications, precautions, and contraindications of vaccines could help educate health personnel, which will undoubtedly contribute to increasing vaccination coverage in the population.

留言 (0)