
記住我
The ethic commission of the veterinary faculty of the LMU Munich approved the use of canine serum samples in the proposed study (reference number 327-20-09-2022).
The study was conducted in a veterinary practice in Amberg (Upper Palatinate, Bavaria, Germany) receiving dog patients from the city of Amberg with a low LB risk of 23.75 reported human cases (RHC) per 100,000 inhabitants (I), the district Amberg-Sulzbach with a medium-high LB risk of 201.95 RHC per 100,000 I, and the districts Schwandorf (292.48 RHC/100,000 I), and Neumarkt in der Oberpfalz (125.14 RHC/100,000 I) [41]. Due to the medium-high risk of human LB in the districts of Amberg-Sulzbach, Schwandorf, and Neumarkt in der Oberpfalz and many cases of tick attachment to dogs leading to anaplasmosis and LB in the region of this veterinary practice, many dog owners are willing to vaccinate their companion animals against LB, resulting in a high vaccination rate in this district. Therefore, this practice was especially suited to study the effectiveness of vaccination schedules retrospectively in an animal-experiment-free setting.Owners asking for a LB vaccination in the practice were given the choice to either vaccinate their dogs with the standard vaccination (i.e., vaccination on days 0, 21, and 365) or to vaccinate with an additional booster (i.e., vaccination days 0, 21, 180, and 365). All dogs were tested before the first vaccination for antibodies specific to LB infection with the commercially available SNAP 4Dx Plus test (IDEXX Laboratories Inc., Westbrook, ME, USA) conducted according to the manufacturer’s instructions to rule out an active infection at the time of vaccination (i.e., day 0). An active infection would have made the treatment of dogs with antibiotics necessary before vaccination. The immunization of dogs who were tested negative in the SNAP 4Dx Plus test was then conducted using the vaccine Merilym 3 (Boehringer Ingelheim Vetmedica GmbH, Ingelheim am Rhein, Germany), which was approved for its use in dogs in March 2013 by the Paul-Ehrlich-Institut (PEI) in Lagen, Germany (PEI.V.11652.01.1). A 1.0-mL dose of this lysate vaccine contains the inactivated Bbsl-complex species B. garinii, B. afzelii, and Bbss. As a preservative, 0.5 mg of formaldehyde are incorporated, and aluminum hydroxide serves as an adjuvant. The vaccination of the dogs was performed subcutaneously in the dorsolateral thoracal region using 24-gauge needles (0.55 mm × 25 mm; B. Braun SE, Melsungen, Germany).
When blood from the vaccinated dogs was collected for diagnostic purposes in the veterinary practice and leftovers were available, these leftover blood samples were stored upright at room temperature for 60 to 180 min until complete coagulation. Samples were then centrifuged at 4000× g for ten minutes. Afterward, the serum was transferred into screw cap microtubes (Sarstedt AG & Co. KG, Nümbrecht, Germany), which were labeled and stored at −20 °C until serological analysis. Blood was collected by either puncturing the right Vena cephalica antebrachii or the right V. saphena lateralis with a 20-gauge needle (0.90 mm × 40 mm; B. Braun SE) and 9-mL Serum-Monovettes Z-Gel (Sarstedt AG & Co. KG). All owners of vaccinated dogs whose blood was collected for diagnostic purposes and residuals were available for LB antibody testing agreed to the transmission and serologic analysis of their dogs’ blood at the Chair of Bacteriology and Mycology of LMU Munich. Serum samples were assigned to nine different periods according to the time that passed between the first vaccination and the sampling for diagnostic purposes. Following one year after vaccination, we divided the observation period into nine time frames and accordingly assigned them to nine descriptive time points (Table 1).At the end of the observation period, all serum samples were tested at the Chair of Bacteriology and Mycology of LMU Munich. Serum samples were therefore thawed at room temperature. For quantitative analysis, total antibody levels specific for LB organisms were evaluated using a KELA as described elsewhere [12,17,38]. Representative samples for every time point from each study group, of which a sufficient volume was available after the first round of serological testing, were assessed for the presence of species-specific rOspA antibodies using a KELA. As the lowest number of serum samples available for one observation timepoint was seven serum samples, we used this number of samples in all KELAs to allow compatibility. Therefore, 96-well-plates were prepared with 1.0 µg of purified recombinant OspA from the strains Bbss ZS7, B. garinii ZQ1, or B. afzelii PKo kindly provided by Prof. Dr. Kraiczy (Institute for Medical Microbiology and Infection Control, Frankfurt, Germany). To confirm positive results and differentiate infected from vaccinated dogs, a line immunoassay (LIA) was performed. Here, the Borrelia Veterinär plus OspA LINE (VIROTECH Diagnostics GmbH, Dietzenbach, Germany) was used to analyze and evaluate the presence of B. burgdorferi sensu lato-specific antibodies according to the manufacturer’s instructions. Statistical AnalysisAntibody levels for each dog were recorded, summarized according to the experimental groups, and compared statistically. KELA curves were visualized using OriginPro, Version 2022 (OriginLab Corporation, Northampton, MA, USA). To compare the KELA levels (i.e., IgG and species-specific) from both groups, we calculated the area under the curve (AUC) between the time points t0 and t30, t30 and t60, t60 and t120, t120 and t180, t180 and t230, t230 and t300, t300 and t350, and t350 and t390. The AUC was then tested for standard deviation using the Shapiro–Wilk test. Besides the AUC between t0 and t30, all AUCs were normally distributed. Significance for the AUC between t0 and t30 was then calculated using the Mann–Whitney test, while all other time frames were tested with the t-test. All analyses were conducted with OriginPro, Version 2022 (OriginLab Corporation). Significance was assumed when the p value was p ≤ 0.05.
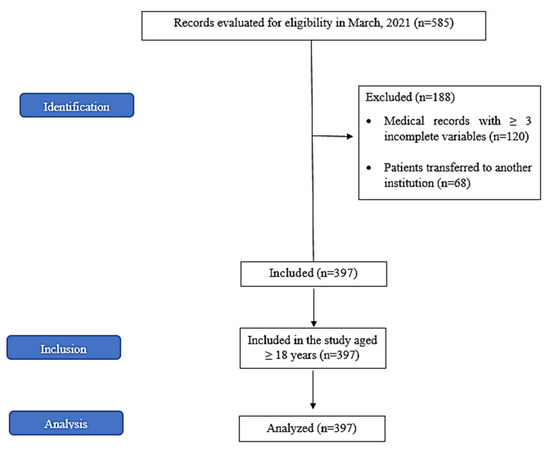
3. ResultsIn total, 183 vaccinations against LB were performed during the project. Of these vaccinations for V-basic, 222 serum samples were analyzed for the classified time points, while for V-plus 223 serum samples were collected and examined for their antibody contents. Of these serum samples, 41% originated from female dogs, while the remaining 59% were from male dogs, 39% of the experimentees were spayed or neutered. The age of the dogs ranged between four months and eleven years. Irrespective of the vaccination group, only moderate side effects were reported. In the test population, 4% of the dogs seemed to be tired one or two days after the immunization, 2% showed signs of moderate pain, and in 0.6% moderate swelling at the injection site was reported. Serum samples displayed negative results in the SNAP 4Dx Plus before the vaccination on t0. However, when analyzing these sera from t0 with a KELA, some of these sera showed antibody levels higher than 100 (n = 10), which is thought to be a threshold that non-infected dogs rarely pass. When analyzing these serum samples on a LIA, a color reaction specific to infection was observed in four serum samples. Sera, which tested negative on the SNAP-test and showed antibody levels below 100 KELA units, displayed a slight color- reaction for the VlsE antigen (VlsE AG line) fainter than the cut-off control (COC) or no reaction at all on the LIA strip (Figure 1B). This is considered negative for LB infection.The first vaccination with the vaccine was performed on t0. All samples available on t30 showed increasing antibody levels in the KELA (Figure 1A) and specific reactions to the OspA antigen on the LIA (Figure 1B). Dogs were then vaccinated a second time on t30, finalizing the basic immunization. After the second immunization, antibody levels measured with the KELA increased further until t60. At this time point, LIA strips displayed color reactions to the OspA antigen that were stronger than the COC in both groups. Color reactions of antigens beside the VlsE and stronger than the COC that occurred on the LIA strips of vaccinated canines are considered reactions to the various antigens provided with the lysate vaccine. After t60, both groups displayed a steady and clear decrease in antibody levels observable until t180 (Figure 1A); on matching LIA strips this can be observed as well as decreasing color intensity of the OspA antigen lines (Figure 1B). Dogs in V-plus, which had received an additional booster vaccination on t180, developed significantly higher antibody levels on t230 compared to dogs in V-basic (Figure 1A). The antibodies reached an average of around 600 KELA units in V-plus, compared to an average of around 300 KELA units in V-basic (Figure 1A). On the LIA strips at time point t230, a stronger color reaction to OspA in V-plus was observed compared to V-basic (Figure 1B). While the antibody levels from the KELA decreased further in V-basic until the booster vaccination around t350 was applied, antibodies in dogs of V-plus increased after the additional booster on t180 and stayed at a significantly higher level until the yearly booster vaccination on t350 (Figure 1A). On t350, V-plus reached KELA units over 500, while in V-basic KELA units stayed below 300. The LIA results support the observations made with the KELA. The color reaction for OspA in V-basic was fainter than in V-plus and similar to the COC and was directly proportional to the decreasing antibody levels (Figure 1B). At the last observation time point (t390), antibodies of both groups displayed similar levels in the KELA (V-basic 588 KELA units on average; V-plus 610 KELA units on average; Figure 1A). LIA strips display a very strong signal for OspA in both groups on t390 after the last booster vaccination (Figure 1B).Reactions to species-specific recombinant OspA (rOspA) originating from the three Bbsl-complex species used in the lysate vaccine were subsequently analyzed by applying species-specific rOspA KELA assays (Figure 2). The antibody levels against Bbss, B. garinii, and B. afzelii from both vaccination groups corresponded to the IgG KELA described above (Figure 1A). However, the measured levels for rOspA-specific antibodies for the three different borrelial species were lower than the IgG KELA levels (Figure 1A) for V-basic between t180 and t350. Further, rOspA KELA levels seem to be highly variable between different canine sera used in these assays. Bbss-specific rOspA antibody levels in V-basic drop until t180 to a mean KELA level of 166 units and drop further until t350 to a mean KELA level of 86. On t180 mean KELA levels of 140 units were observed for B. garinii, that drop to 86 units on t350. Mean KELA levels for B. afzelii are at around 179 KELA units on t180 and declined to a mean of 115 KELA units on t350. When applying a booster vaccination on day 180 (i.e., V-plus), a drop in antibody levels until t180 was observed in this group as well. However, the booster vaccination on t180 lead to an increase in antibody levels on t230 (Figure 1). This increase led to higher antibody levels until the last booster vaccination on t350. 4. DiscussionDue to climate change and an increase in global temperature, we must expect an increase in tick population and a year-round activity of ticks [10,11,42]. This leads to the conclusion that there is a perennial risk of tick exposure and infection with TBD such as infections with Bbsl causing LB. As described above there are three columns of protection against LB: tick removal, use of repellents and acaricides, and vaccination. Tick removal only protects against LB when dogs are scanned for ticks after every walk and all ticks are found and removed promptly. Acaricides and repellents should be applied individually to the owner’s preferences and the dogs’ tolerance. All-year-around protection must be provided by reapplying the protective agent routinely. Further, ticks can develop resistance to these repellents and acaricides [27]. The vaccination against LB, based on inactivated Bbsl-complex species expressing the OspA provides the most reliable protection against LB, as the vaccination not only protects against the development of disease but further protects against the transmission of Bbsl-complex species to the canine host [43]. However, it is crucial to vaccinate against the genospecies that lead to infections in the dogs’ geographical environment and to provide perennial protection by keeping antibody levels high enough [44].In this study, we hypothesized that the vaccination schedule of Merilym 3 (Boehringer Ingelheim Vetmedica GmbH, Ingelheim am Rhein, Germany) as provided by the manufacturer is not sufficient to protect dogs against LB, especially in autumn when a dog is immunized during the spring season. The basic vaccination is recommended to be applied at the beginning of tick season (i.e., spring) followed by a yearly booster vaccination. Other vaccines available in Germany (i.e., Virbagen canis B, Virbac Tierarzneimittel GmbH, Bad Oldesloe, Germany, and Rivac Borrelia, Ecuphar N.V., Oostkamp, Belgium) recommend a further booster vaccination four to six months after the basic immunization [45]. Therefore, we applied the vaccine Merilym 3 according to the vaccination scheme provided by the manufacturer and compared canine antibody levels of dogs receiving the standard vaccination scheme to antibody levels induced by a vaccination scheme with a booster vaccination on t180. Antibody levels were measured with a KELA system and vaccination-specific antibodies were further confirmed with a LIA. As Figure 1 depicts clearly, the standard vaccination scheme (i.e., V-basic) leads to a drop in antibody levels between t180 and t350. This can also be observed by the intensity of the signals on the LIA. When considering the antibody levels observed in the species-specific rOspA KELAs, it becomes very clear, that antibody levels induced with the standard vaccination scheme might not protect against borrelial transmission in autumn. Therefore, we conclude, that the standard vaccination scheme initiated in spring produces a gap in protection against LB in autumn (Figure 3).Furthermore, the vaccination scheme with an additional booster on t180 is already recommended for the two other vaccines used in Germany [45]. Considering the decrease in antibody levels between t60 and t180, it might even be too late to apply the booster vaccination on t180 and as described for the other two German vaccines (i.e., Rivac Borrelia and Virbagen canis B) an earlier booster vaccination between days 100 and 150 might even be more adequate. Future research on this issue is urgently needed as well as the characterization of an antibody level protective against infection with borrelial organisms.The authors would further like to address some general considerations regarding the LB vaccination in dogs. It has recently been discussed that the LB vaccine should still be considered a non-core vaccine in the vaccination guidelines [46] and applied according to the risk assessment of individual patients [45,47]. Therefore, veterinarians and veterinary clinics must be aware of the LB risk and apply individual recommendations regarding the dog’s exposure (i.e., working dogs, hunting dogs, traveling). Furthermore, the owners must be made aware of the risks of LB infection and thus must be informed about the importance of rigorous tick scanning after walks and the application of repellents and acaricides. Due to client failure in detecting and removing ticks and continuous application of repellents, adequate protection of canines might not be given and thus LB can occur. A safer method would be the continuous vaccination against LB in endemic regions. However, even when dogs are vaccinated against LB, owners need to keep in mind, that ticks transmit additional infectious agents like Anaplasma spp., Ehrlichia spp., which can only be avoided by removing ticks [23] and applying repellents or ectoparasitic agents. As tick-borne encephalitis virus is transmitted within an hour [48], avoiding an infection is only possible by applying repellents. Further, working and hunting dogs that due to their assignments are especially exposed to ticks and tick bites and thus endangered to infection with Bbsl-complex species should be protected against LB using every available option especially as their training is expensive and time-consuming and downtime due to LB can easily be avoided. The endemic regions are shifting due to climate change and the ability of ticks to reside in regions that have up to date not been habitable [1]. A further point that must be considered is the increase in tick population due to fewer population losses when winters are milder. Increased temperatures in winter, autumn, and spring further lead to increased activity of ticks in these seasons, which some owners might not be aware of. Additionally, rising global temperature and urban sprawl will increase the population of rodents and small mammals that will, in turn, contribute to the increase of tick populations in these areas [49]. In sum, veterinarians must be informed about such changes and the endemic regions of TBD and inform owners professionally and transparently of the best options for TBD prevention and LB protection, not only in the best interest of the dogs’ but also in the interest of the owners’ health.Lately, the opinion has been expressed that the “rationale for canine LB vaccination is unpersuasive” [50] and the experts of the American College of Veterinary Internal Medicine could not agree on a recommendation for a LB vaccine [20]. This matter has further been reasoned with a statement of the American Animal Hospital Association regarding not recommended vaccines [51]. However, this reference refers to not recommended vaccines in pet cats and discusses the use of a vaccination against feline infectious peritonitis. Nevertheless, it is stated, that vaccines are not generally recommended for diseases with a low clinical significance, that display a good response to treatment, and where evidence of vaccination in the field is minimal and adverse events occur frequently [50]. Therefore, the authors feel obligated to address these issues as it affects the reputation of this important vaccine and harms the willingness of veterinarians to recommend and owners to make use of this vaccination. Regarding the low clinical significance, it has been discussed, that 95% of dogs display no clinical signs [50]. This statement first occurred in a study from 1992 by Levy et al. [19]. In this study, 234 dogs were analyzed for Bbsl-specific antibodies and according to their reaction divided into a seronegative (n = 109) and a seropositive (n = 125) group of dogs that were further monitored for 20 months. In both groups, the incidence of limb/joint disorder, lethargy, fever, and inappetence was nearly 5%. Retesting was possible in 202 canines (105 dogs from the seropositive group and 97 dogs from the seronegative group). Some of the examined canines from both groups were treated with antibiotics during the observation period. The observation of seropositive dogs seems incomprehensible, as we do not know when the infection occurred and how long it has been persisting. Regarding the seronegative group that seems sensible to observe, 88 from 97 dogs remained seronegative. Thus, nine dogs have seroconverted, of which two had received antibiotics. The clinical signs these nine dogs displayed are not clear. Further, the diagnosis of LB was based on the occurrence of limb/joint disorder accompanied by fever, lethargy, and inappetence [19]. As fever has been reported to only peak on single days [52] a co-occurrence would be observed rarely. Returning to the study by Levy et al. (1992) [19], a further sign of LB was the prompt response to antibiotic treatment. However, other bacteria might react to this antibiotic treatment as well, making the exclusion of differential diagnoses crucial. Regardless, differential diagnoses have not been ruled out. Serologic results have not been reported as the actual time of infection was unknown to the author. For animals diagnosed with LB due to clinical signs and prompt reaction to antibiotic treatment neither serologic results nor evidence of borrelial organisms have been reported (i.e., PCR, pathology, or serology) [19]. Therefore, the results from this study must be considered with caution. Nevertheless, this number of dogs displaying no clinical signs has first been cited by Appel et al. (1993) [12] and has in the following years been cited and used various times. However, this number of 5% clinically LB conspicuous dogs in the field is highly questionable and other researchers have provided numbers from clinical studies on dogs that are more reliable. Straubinger et al. (1997) [52] observed severe clinical lameness in 65% of canines experimentally infected and confirmed seropositivity, 10% of seropositive dogs displayed mild lameness, and 25% showed no clinical signs. Of canines that displayed clinical signs, 55% displayed an increase in temperature > 39.4 °C for a single day. In another study, 77% of dogs developed lameness, accompanied in 80% of lame dogs by concurrent fever (≥38.0 °C). In 92% of dogs, Bbss organisms were recovered from skin and joint tissues samples [22]. In another trial, 69% of dogs developed clinically apparent arthritis after tick exposure [53]. Furthermore, described clinical signs of LB can vary strongly and canines displaying stiffness, lameness, arthritis, and joint swelling [52] are often not recognized and tested for LB. Additionally, further maladies like cardiac signs [54,55,56], nephritis [57,58,59], neurologic disorders [15,60], rheumatoid arthritis [61], and myositis [62] have been described to occur in canine patients with LB. It is questionable whether owners can connect these disorders with a tick bite that probably has occurred months before the onset of clinical signs [12,52] and if veterinarians then test dogs with these unspecific clinical signs for LB. Many dogs have been reported displaying no clinical signs [12,22,52], however, the authors wonder if we can recognize mild clinical signs and minimal to moderate pain in canines. In humans it is known that mild to moderate chronic pain affects physical and psychological health [63]. When considering a seroprevalence of around 2 to 20% [16,17], we have to assume that of 10.3 million dogs in Germany in 2021 [64] on average 11% (1,100,000 dogs) are infected with Bbsl-complex species. Considering that in animal trials on average 75% of dogs display clinical signs [52], we calculate that around 50% of dogs in the field might display clinical signs. Of the 1,100,000 infected dogs, at least around 550,000 dogs in Germany assumably might display clinical signs and probably experience a reduction in quality of life. Further, one needs to consider that the clinical signs of canines observed in trials have been conducted with Bbss only [22,52]. However, other genospecies (i.e., B. garinii and B. afzelii) might lead to similar or further unrecognized disorders, therefore, research on clinical signs caused by these genospecies is necessary to evaluate the impact of Bbsl on dogs. In conclusion, in the authors’ opinion LB is no disease with low clinical significance and its well-documented appearance in endemic regions does not support the apprehension against LB vaccination.Regarding the One Health concern, not only the transmission of antibiotic resistances but also the transmission of disease to humans and further animals must be considered. It has been implied that there is no direct transmission of Bbsl-complex species from animal to animal or from animal to human [50]. The authors agree with this statement and the absence of direct transmission has been proven in dogs [52]. However, many indirectly transmitted vector-borne diseases may be further dispersed by our pet animals and increase the risk of vector-exposition for humans. Infected nymphs or uninfected nymphs or larvae that can be infected during the blood meal on a seropositive dog may be carried into human habitats (i.e., urban parks or gardens), where the engorged nymphs then drop off and molt to adult ticks. These adults can then bite humans and thus transmit borrelial species [65]. A further concern is that vaccination of canines does not reduce LB prevalence [50]. In parts, the authors agree with this statement, as the vaccination of dogs does not influence the sylvatic infectious chain. However, considering that most dogs and humans will not go deep into the woods, and most humans living in cities will conduct their free-time activities in urban parks and greens, the carriage of ticks into these regions displays the greatest danger to the largest human population, townsfolk. Therefore, the authors consider an LB vaccination beneficial regarding the One Health concern.Species distribution of borreliae is highly variable between the continents [3]. Therefore, it is not possible to use one single vaccine worldwide [37]. Vaccines used should contain all infective agents responsible for LB infection in the geographical area. For Europe, these agents are B. afzelii, B. garinii, and Bbss [36]. All vaccines available in Germany are at least bivalent, however, the vaccine used in this study is the only trivalent option containing all three borrelial species. The vaccination, in combination with manual tick removal by the owners and the disciplined use of acaricides and repellents, allows the maximum of protection possible, as removal and repellents alone might not disable all tick attachment. In the authors’ opinion, the combination of these options with a vaccine is still the safest method to prevent LB in dogs. However, as ticks not only transmit LB, veterinarians and owners must be aware, that the vaccination is the best protection against LB, tick removal and repellents must still be conducted to protect canines against other TBD.Retrospective observation originating from LB-vaccinated dogs show, that vaccination against LB is most effective when it is applied on days 0, 30, 180, and 360. When a booster vaccination on day 180 is missed, canines display a gap of immunity in autumn, while ticks still display a high questing activity. For the best protection in dogs, a booster vaccination on day 180 is urgently advised, as has been displayed for equines [39]. Further, the use of a canine LB vaccination in endemic regions, in general, seems highly advisable, especially regarding the One Health concern [65]. An infection with LB probably leads to the unnecessary suffering of many animals, that display clinical signs obvious or hidden to their owners, probably reducing the quality of life in these dogs. Infected dogs displaying clinical signs are treated with antibiotics that could have been renounced. Additionally, canines display a risk to their owners by carrying infected ticks in the urban space or by infecting uninfected ticks in the urban space [65].
留言 (0)