
記住我









The present study is a parallel two-phase randomized controlled clinical trial that will be conducted at Shariati Hospital in Tehran, Iran. All participants must complete and sign an informed written consent form prior to completing their registration (Supplementary file, section A). Ethical approval has been obtained by the Bioethics Committee of Tehran University of Medical Sciences (No. IR.TUMS.MEDICINE.REC.1400.200).
Study populationThe current single-blind randomized controlled trial is a two-phase community-based research project. Participants will be recruited through a popular online advertising program rather than a health care center or hospital. This will be done to better reflect population diversity and produce more generalizable results across populations.
Inclusion criteriaThis study will be conducted on adult women with metabolic syndrome who have body mass index (BMI) greater than or equal to 25 and aged 20–50 years. MetS was defined as having three of the five conditions listed in the Adult Treatment Panel III guidelines from the National Cholesterol Education Program (NCEP-ATP III) [36]: (1) waist circumference of more than 88 cm (35 inches), (2) serum triglyceride (TG) level greater than 150 mg/dL, (3) serum high-density lipoprotein cholesterol (HDL-C) level of less than 50 mg/dL, (4) blood pressure greater than 130/85 mm Hg, and (5) fasting plasma glucose (FPG) levels greater than 100 mg/dL. Patients who reside in Tehran will be included in the study to minimize loss to follow-up. This study will only include women because it has been demonstrated that women are more likely than men to maintain dietary changes and adhere to the prescribed diet regimen after participating in a dietary intervention trial [35, 37].
Exclusion criteriaPatients who meet the following criteria will be excluded from the study: (1) pregnancy, breastfeeding, or planning to become pregnant in the near future; (2) being current smokers or using other tobacco such as hookah; (3) evidence of some pathologic conditions such as liver, kidney, thyroid, and gastrointestinal tract diseases as well as suffering from diabetes, rheumatoid arthritis, lupus, severe infection, and trauma; (4) weight loss history surgery; (5) having a severe allergy to specific foods; (6) have been on a special diet or taken weight loss medication for three months prior to the study; and (7) consumed antibiotics, pre- or probiotic products or supplements 3 months prior to enrollment. We will also exclude postmenopausal women, participants who are unwilling to continue the intervention and have poor adherence to the prescribed (their dietary records show that their intake deviates more than 300 kcal from the prescribed amount, or dietary records show that the recommended macronutrient composition is not followed), and those who become infected with COVID-19 during the intervention. Figure 1 presents a schematic representation of the overall research plan.
Fig. 1
Flow chart of the study process
Sample size calculationUsing a type I error of 5% (α = 0.05) and a type II error of 20% (β = 0.20, power = 80%), and serum HDL-C concentrations as the key variable, the sample size in this study was calculated using the following formula, which has been proposed for parallel clinical trials:
$$n=\frac}_}+}_\right)}^2\times ^2\right]}}^2}$$
n = sample size for each group.
σ = The variance (SD) for mean HDL-C concentrations was as 3.5, which was calculated using the average SDs reported for serum HDL-C in Rajaie et al. study [35].
d = The minimal clinically important difference for HDL-C was set at 2.5, based on previous research [38].
Overall, using this formula and assuming a 10% drop-out rate in each group, we will require a sample size of 35 subjects in each group.
Study designA total of 100 women with metabolic syndrome will be screened according to the aforementioned inclusion criteria in the initial phase. After recruiting participants from online advertisements and social media, seventy women who meet the inclusion criteria will be included in the entire project. Patients will be enrolled using a stratified block randomization procedure with a block size of 4. Participants will be randomly assigned to the intervention or control groups based on stratification by age (20–30, 30–40, and 40–50 years) and BMI (25–29.9, 30–34.9, and > 35 kg/m2). First, we will enroll a woman in a stratum that meets the inclusion criteria. Following that, the second person matched based on these variables with the first one will be placed in the same stratum. Consequently, two participants with similar characteristics (for the aforementioned variables) would be in the same stratum (Supplementary file, section B). Finally, using a random allocation software, two subjects from the same strata will be randomly assigned to either moderately restricted carbohydrate diet (MRC) or normal weight loss (NWL) diet groups. The principal investigator (SMM) will enroll eligible women. All participants will sign a consent form before inclusion in the study, in which information about the prescribed diets, duration of the study, and contact information for the research team are provided. Study participants will be informed that the services given to them will be free of charge and that they can withdraw from the study at any time throughout the study. Each person will receive a booklet, including a pre-designed dietary plan containing a series of menus and recipes for breakfast, lunch, dinner, and snacks according to the prescribed diet. In the current trial, outcome assessors will be blinded to the intervention allocation. The study protocol for this clinical trial was registered with the Iranian Registry of Clinical Trials in advance (IRCT20210307050621N1). The flow diagram of the research process is presented in Fig. 2.
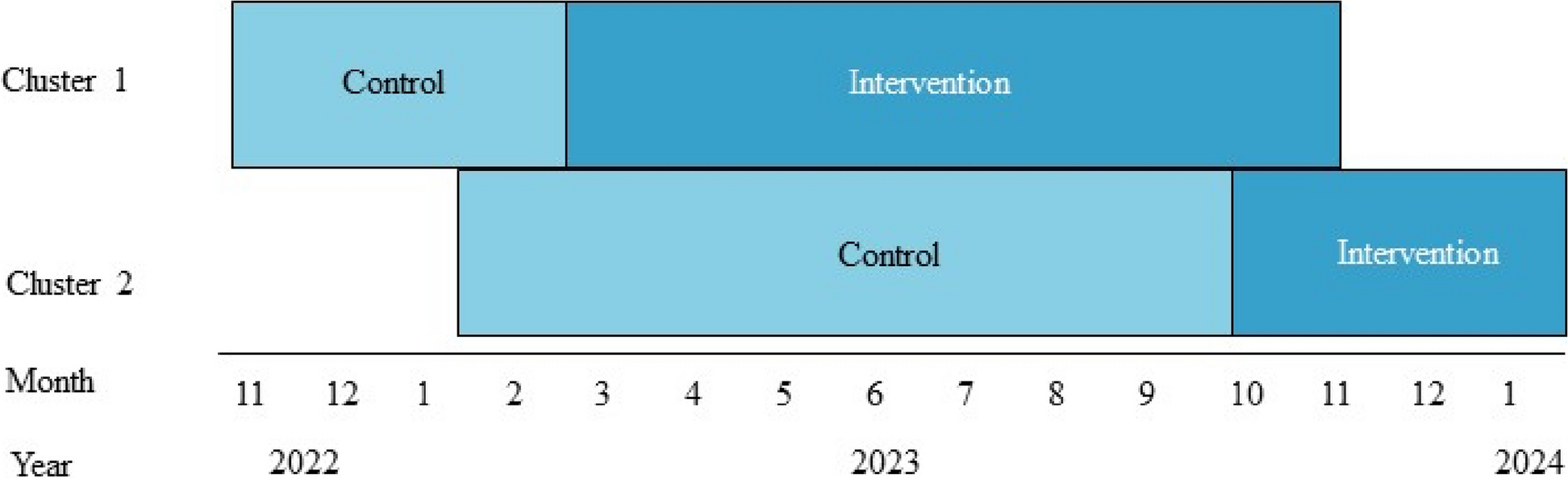
Fig. 2
Enrollment, interventions, and assessments at various points in time. The “X” denotes what has been accomplished during a specified time period. Mth, month
InterventionParticipants will be randomly assigned into one of the two above-mentioned groups. During an hour-long discussion, each participant will be instructed on either the MRC diet or NWL diet. All participants will receive a calorie restricted diet based on their status of weight and BMI (300–500 kcal less than participant’s energy requirement). We will compute calorie requirements based on resting energy expenditure (using the Harris-Benedict equation) and physical activity levels. The main distinction between these two diets will be the proportion of calories derived from fats and carbohydrates. The MRC diet will be defined as 42–45% of energy from carbohydrates and 35–40% from fats, while the NWL diet will be defined as 52–55% of total calories from carbohydrates and 25–30% from fats. In fact, 10% of energy from carbohydrates in the MRC diet will be substituted with non-hydrogenated vegetable oils. Dietary protein intakes will be accounted for 15–17% of total energy across both dietary groups. The first phase of the study in which subjects will receive the aforementioned diets will last for 3 months. Then participants will enter the second phase, in which all participants will be followed for another 6 months on a weight-maintenance (WM) diet containing a normal proportion of macronutrients, including 52–55% carbohydrates, 27–30% fat, and 15–17% protein. The main objective of this phase is to determine whether the changes caused by the intervention will be maintained after six months. In addition, it will be determined if changes in gut microbiota persist after 6 months of a weight-maintenance diet and to what extent these changes might contribute to weight maintenance and the stabilization of metabolic variables after 6 months.
ComplianceTo assess how well participants adhere to their diets, their dietary intakes will be recorded once every 2 weeks in the first phase and every 4 weeks in the second phase by telephone interview. A sample of dietary recall format is provided in Supplementary file, section C. In total, participants are going to complete 12 dietary records (six in the first phase and six in the second phase). Participants will be asked to report their dietary intakes using household measures in order to complete the dietary recalls. Then, we will convert household measures to grams using the booklets provided. Participants’ total dietary intakes will be assessed using the average of all dietary recalls taken over the duration of the intervention. Total energy intake, macronutrients, and micronutrients will be computed from the dietary recalls using Nutritionist-IV software (First Databank, San Bruno, CA, USA) modified for Iranian dishes. We will also send text messages and make phone calls to participants throughout the study to increase compliance and prevent forgetfulness of diet principles.
Intervention safetyThere have been no serious side effects associated with moderate carbohydrate restriction diets. To investigate any potential side effects, we will ask participants to report any changes during the study period concurrent with their dietary assessment via phone interview.
Assessment of variablesA standard questionnaire will be used to collect data on participants’ age, ethnic origin, marital status, educational level, disease history, family history of disease, medication use, and history of COVID-19 and type of vaccination. We will also measure primary outcomes including serum lipid profile concentrations, fecal bacterial load, and glucose levels, as well as secondary outcomes including anthropometric measurements and blood pressure at the beginning of the study, end of the phase I (3 months), and end of the phase II (6 months).
Biochemical assessmentsA blood sample will be taken from each patient’s venous blood at the study baseline, end of the first phase (after 3 months), and end of the second phase of the study (after 9 months) following 12 h of fasting. We will use a portion of the blood sample to evaluate glucose levels and lipid profile. The remaining serum will be kept at – 80 °C until it is further analyzed for insulin levels. Plasma glucose and lipid profile concentrations (TC, HDL, LDL, and TG) will be determined via an enzymatic colorimetric method using commercial kits. Finally, the serum insulin concentrations will be examined using electrochemiluminescence (ECL) method. We also will determine insulin resistance (HOMA-IR) and quantitative insulin-sensitivity check index (QUICKI) formulas.
Stool samples and gut microbiota assessmentA 10-g stool sample will be collected from each participant at study baseline, 3 months after intervention, and 6 months after the end of intervention using a stool specimen collection kit that will be brought to the clinic in ice packs within 4 h. Until fecal microbial analysis, stool samples will be frozen at – 80 °C in the laboratory. To minimize changes in the quantity of fecal bacteria, we will collect stool samples in one of three ways: first, we will invite patients to visit the laboratory on the day of fecal sampling. The lab will be equipped with all of the necessary equipment to collect fecal samples. The second method requires the patient to transport the sample to the laboratory within 4 h of their sampling. Finally, if the patient is unable to complete any of the prior approaches, they should contact the study researchers, who will collect their sample at their home and transfer it within 4 h to the lab.
DNA extraction from 200 mg of frozen stool samples will be done using a FavorPrep Stool DNA Isolation Mini Kit (Favorgen Biotech Corp., Taiwan) according to the manufacturer’s instructions. The extracted bacterial DNA purity and concentration will be determined by Nanodrop spectrophotometer (Thermo Scientific NanoDrop, USA). All the extracted DNAs will be stored at − 20 °C freezer until further analysis. Additionally, the quantity of fecal bacteria, including Firmicutes, Bacteroidetes, Bifidobacteria, Lactobacillus, Clostridium, Prevotella, Bacteroidetes, and Akkermansia muciniphila, will be determined using a quantitative real-time polymerase chain reaction (qRT-PCR) in duplicate. We selected the taxa based on their association with metabolic syndrome and their ability to balance the gut microbiota [39, 40]. Specific primers targeting the bacterial 16S rRNA genes blasted in NCBI will be used in the current study. Each reaction mixture is composed of SYBR Premix Ex Taq II (Takara, China), the specific forward and reverse primers, and a DNA template. The thermal cycling conditions will be as follows: an initial DNA denaturation step at 95 °C for 1 min, 40 cycles of denaturation at 95 °C for 5 s, primer annealing at 55 °C for 30 s, and extension at 72 °C for 30 s. Finally, in order to confirm the specificity of the amplification products, melting curve analysis will be performed by slowly cooling the PCRs from 95 °C to 60 °C.
Anthropometric measuresWeight will be determined with the minimum clothing without shoes using a weighing calibrated scale (Seca, Hamburg, Germany) to the nearest 100 g. Standard stadiometer will be used to measure barefoot standing height to the nearest 0.5 cm. Measurement of the waist and hip circumferences will be done to the nearest 0.5 cm using a strip tape measure over light clothing without applying pressure to the body surface. The waist and hip circumferences will be defined as the circumference around the belly button and the diameter of the hip’s largest point. The body mass index (BMI) will be calculated by dividing weight in kilograms by the height in meters squared.
Blood pressure assessmentAfter at least 5-min resting, measurements of systolic and diastolic blood pressure will be done twice with 15-min intervals in the right arm using a mercury barometer calibrated by the National Institute of Standards and Industrial Research. The average of two blood pressure readings will be used to determine an individual’s blood pressure.
Physical activity assessmentWe will determine the level of physical activity of participants based on their once in a month physical activity recording (including working and non-working days) (Supplementary file, section D). Physical activity levels will be classified as low, moderate, or high and expressed in metabolic equivalents per week (MET-min/week).
ConfidentialityThe information about participants will be stored anonymously according to TUMS rules. During laboratory tests and in all records, participants will only be able to be identified by their ID number so as to assure their privacy and confidentiality. In a secure database, we will store participants’ identifying information separately from the research data collected during the study. Moreover, all specimens will be stored in the TUMS biochemistry laboratory. All study data will be kept strictly confidential on password-protected computers in the research team’s office, which will be accessible only by the research team. The corresponding author will provide anonymized data to other researchers in order for them to conduct secondary studies after the trial has been completed on reasonable request.
Data management and monitoringPrincipal study coordinators will be SMM and BL, who have designed the study and will be responsible for project oversight. In fact, the Trial Steering Committee (TSC) is comprised of AE and BL as key members, the study physician (SHR), the study assistant and study advisor (SDS), the statistician and study advisor (HSE), and the principal investigator (SMM). Monthly meetings of this committee will be held to assess performance and progress, overcome technical and financial challenges, and develop plans to meet project deadlines. A separate data monitoring committee is not required due to the low-risk nature of the intervention. The laboratory of the Endocrine and Metabolism Research Institute at Tehran University of Medical Sciences serves as the coordinating canter, where blood sample, serum collection, storage, and all laboratory testing are conducted. Main investigator (SMM) is responsible for coordinating visits for identifying potential participants and obtaining consent. There will be a Data Management Team comprising the principal investigator (SMM) and the project supervisors (AE and BL).
Statistical analysisAll statistical analyses will be carried out using the SPSS software version 25 (SPSS Inc., Chicago, IL, USA). For addressing non-adherence, the intention-to-treat (ITT) analysis will be applied [41]. Moreover, we will apply the last observation carried forward method (LOCF) to handle missing values [42]. In order to determine the normal distribution of variables, we will use the Kolmogorov-Smirnov test, histogram, and Q-Q plot. We will log transform (ln) the data, if necessary, to achieve normal distribution. Data will be presented as mean ± standard deviation (SD) for continuous variables and as percentages for categorical variables. Chi-square test and independent samples t-test will be used for comparing continuous and categorical variables between the two groups, respectively. We also will use the paired-sample t test for within-group comparisons. Repeated measures analysis of variance will be employed to determine the impact of the intervention on the outcome variables. These analyses will examine the effects of the intervention, time, and the interaction between time and intervention. Any potential differences in baseline levels of outcome variables, dietary intakes, and physical activity will be controlled in these analyses. Statistical significance will be defined as P values less than 0.05.
留言 (0)