
記住我
The 2019 ASCCP Risk-Based Management Consensus Guidelines (abbreviated hereafter as 2019 guidelines) are the current national consensus guidelines used to manage the results of cervical cancer screening tests in the United States.1 In the 2019 guidelines, clinical management decisions are based on risks of an individual having or developing cervical intraepithelial neoplasia lesion grade 3 (CIN 3), adenocarcinoma in situ, or cancer, collectively defined as CIN 3+. The 2019 guidelines are based on the principle of equal management for equal risks, defined as recommending the same management for patients with the same risk of CIN 3+. For the 2019 guidelines, a patient's immediate and 5-year risk of having CIN 3+ are used to determine clinical management. Colposcopy is recommended for patients with an immediate CIN 3+ risk of 4%–24%, colposcopy and expedited treatment (i.e., proceeding directly from screening test results to an excisional procedure without the need for an additional visit for colposcopic biopsies) is both recommended options for patients with immediate CIN 3+ risk of 25%–59%, and expedited treatment is preferred, with colposcopy an acceptable option, for patients with immediate CIN 3+ risk of 60%–100%.1–3 For patients with immediate CIN 3+ risks lower than the colposcopy threshold (4% immediate CIN 3+ risk), repeat testing is recommended at either 1-, 3-, or 5-year intervals, with the interval determined by the patient's risk of developing CIN 3+ over the next 5 years (i.e., 5-year risk). These risk estimates were generated using long-term observational screening and management data from Kaiser Permanente of Northern California (KPNC). Risk estimates were based on data from more than 1.5 million KPNC patients who received cotesting with cytology and human papillomavirus (HPV) testing between 2003 and 2017.2,3 This large, longitudinal data set allowed precise risk estimation over long follow-up periods.
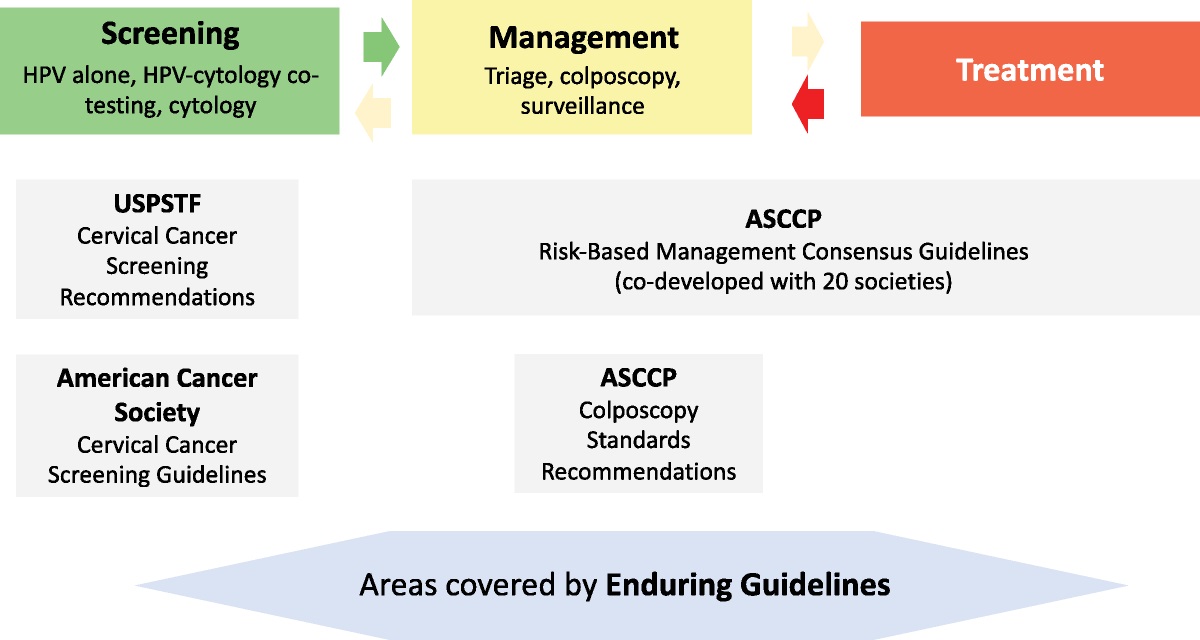
Because of the rapid progress in the cervical cancer prevention field,4–6 the Enduring Consensus Cervical Cancer Screening and Management Guidelines (Enduring Guidelines Committee) effort was established to integrate new technologies and approaches into the existing guidelines framework (https://dceg.cancer.gov/research/cancer-types/cervix/enduring-guidelines). Most data for technologies other than HPV testing and cytology are limited to observational studies and clinical trials with fewer than 5 years of follow-up. As 5-year data may be lacking, additional approaches are needed to incorporate new technologies into existing risk-based guidelines. This report describes a methodological addendum to the 2019 guidelines by generating 3-year equivalents for 5-year risk estimates and details of the consensus voting process and adoption of the new approach to evaluate new technologies when 5-year data are not available.
METHODSIn the 2019 guidelines, repeat testing in 5 years was recommended for a 5-year risk of CIN 3+ of less than 0.15%, repeat testing in 3 years was recommended for a 5-year risk of 0.15% or greater and less than 0.55%, and repeat testing in 1 year was recommended for all patients with a 5-year risk of 0.55% or greater and an immediate risk less than 4%. To determine the equivalent clinical action thresholds for 3-year CIN 3+ risk, we considered all screening test scenarios in which we previously estimated risks for the 2019 guidelines.2 These risk estimates are based on the KPNC cohort of which details have previously been described.3 The use of KPNC data for this research was approved by institutional review boards at KPNC and the National Cancer Institute.
We identified all screening test result scenarios from the 2019 guidelines that had 5-year CIN 3+ risks close to 0.15% (0.15% ± 0.03%) and 0.55% (0.55% ± 0.25%). These risk ranges were chosen according to the natural clustering in the distribution of estimated risks. We then calculated the average percent CIN 3+ risk increase from 3 to 5 years, weighting each scenario by the frequency of occurrence. We derived equivalent 3-year risk thresholds by subtracting this difference from the 0.15% and 0.55% risk thresholds. We then assessed whether use of the 3-year thresholds in place of the 5-year thresholds would have changed the 2019 risk-based management recommendations for any of these scenarios. While we evaluated this approach over the whole range of risk estimates as a proof of principle, we did not attempt to extrapolate less than 5-year risk estimates to support decisions about 5-year screening intervals.
Consensus VoteThese data and the proposed methodological addendum to the 2019 guidelines were presented to the Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee, which includes representatives from 20 national organizations, on July 12, 2021 (https://dceg.cancer.gov/research/cancer-types/cervix/enduring-guidelines#participating-organizations). After the discussion and clarifications of questions related to the proposed strategy, a vote was held. A yes vote from two thirds of the present voting members was required to pass the recommendation.
RESULTS Identification of 3-Year Risk Equivalents for 5-Year Risk ThresholdsTo identify correlates of 5-year thresholds, we evaluated the current risk estimates around the 5-year thresholds of 0.15% (corresponding to the 5-year retesting threshold) and 0.55% (corresponding to the 3-year retesting threshold). We identified 4 HPV- or cotest-negative test result scenarios with 5-year CIN 3+ risk around the 0.15% risk threshold (see Table 1, Figure 1). The weighted mean difference between 3- and 5-year risks for these test scenarios was 0.06%. Hence, an equivalent to the 0.15% CIN 3+ 5-year risk threshold is 0.09% CIN 3+ 3-year risk.
TABLE 1 - List of Screening Test Results in the 2019 ASCCP Risk-Based Management Consensus Guidelines With a 5-Year CIN 3+ Risk Around 0.15% Past history (previous 2) Past history (most recent) Current HPV result Current PAP result n CIN 3+ cases CIN 3+ 3-y risk, % CIN 3+ 5-year risk, % Recommended management in guidelines Management confidence probability % No history HPV-negative NILM 1,388,153 1,246 0.07 0.12 5-y follow-up 100 No history HPV-negative ALL 1,420,033 1,472 0.08 0.14 5-y follow-up 95 HPV-negative/ASC-US HPV-negative NILM 13,918 14 0.07 0.14 5-y follow-up 58 Low grade - > Colpo < CIN 2 Cotest-negative HPV-negative NILM 13,431 10 0.14 0.18 3-y follow-up 66 High grade - > Colpo < CIN 2 Cotest-negative HPV-negative NILM 2,686 2 0.15 0.18 3-y follow-up 56This table lists clinical scenarios in 2019 guidelines, which have 5-year risk in a close interval around 0.15% (0.15% ± 0.03%).
NILM indicates negative for intraepithelial lesion or malignancy.
 FIGURE 1: Increase in CIN 3+ risk from year 3 to year 5 among test results with 5-year CIN 3+ risk around 0.15%. Cumulative risk curve for scenarios with 5-year CIN 3+ risk around 0.15% with each color corresponding to a different scenario from Table 1. For these scenarios, we obtained the weighted average increase from years 3 to 5, weighted by frequency of occurrence as indicated by N in Table 1. The average percentage increase from 3- to 5-year CIN 3+ risk is calculated as 0.06%. The red line in the figure represents 0.06% increase from 3- to 5-year risk, and hence, the equivalent clinical action management threshold for a 3-year follow-up is obtained as 0.09% CIN 3+ 3-year risk, which is equivalent to 0.15% CIN 3+ 5-year risk. Only scenarios with large numbers (10 or more) of observed CIN 3+ cases are plotted.
FIGURE 1: Increase in CIN 3+ risk from year 3 to year 5 among test results with 5-year CIN 3+ risk around 0.15%. Cumulative risk curve for scenarios with 5-year CIN 3+ risk around 0.15% with each color corresponding to a different scenario from Table 1. For these scenarios, we obtained the weighted average increase from years 3 to 5, weighted by frequency of occurrence as indicated by N in Table 1. The average percentage increase from 3- to 5-year CIN 3+ risk is calculated as 0.06%. The red line in the figure represents 0.06% increase from 3- to 5-year risk, and hence, the equivalent clinical action management threshold for a 3-year follow-up is obtained as 0.09% CIN 3+ 3-year risk, which is equivalent to 0.15% CIN 3+ 5-year risk. Only scenarios with large numbers (10 or more) of observed CIN 3+ cases are plotted.There were 7 screening test result scenarios with 5-year CIN 3+ risk close to the 0.55% risk threshold (between 0.40% and 0.80%; see Table 2, Figure 2). These results include HPV-negative atypical squamous cells of undetermined significance (ASC-US) and low-grade squamous intraepithelial lesion (LSIL) results from routine screening and surveillance, postcolposcopy, and posttreatment scenarios. The weighted mean difference between 3- and 5-year risks for these test result scenarios was 0.16%; therefore, we estimated 0.39% to be the equivalent CIN 3+ 3-year risk threshold.
TABLE 2 - List of Screening Test Results in the 2019 ASCCP Risk-Based Management Consensus Guidelines With a 5-Year CIN3+ Risk Around 0.55% Past history (previous 2) History (most recent) Current HPV result Current PAP result n CIN 3+ cases CIN 3+ 3-y risk, % CIN 3+ 5-y risk, % Recommended management in guidelines Management confidence probability % Low grade - >Colpo < CIN 2 HPV-negative/ASC-US or LSIL HPV-negative NILM 1,308 2 0.28 0.31 3-y follow-up 63 CIN 3—>treatment Cotest-negative ×3 1,099 2 0.35 0.35 3-y follow-up 58 High grade - >Colpo < CIN2 HPV-negative HPV-negative ALL 3,137 6 0.25 0.36 3-y follow-up 79 HPV-negative HPV-negative ASC-US 14,372 43 0.20 0.36 3-y follow-up 100 Low grade - >Colpo < CIN 2 Cotest-negative HPV-negative ASC-US/LSIL 549 1 0.26 0.39 3-y follow-up 39 No history HPV-negative ASC-US 25,331 83 0.24 0.40 3-y follow-up 100 HPV-negative/LSIL HPV-negative NILM 1,547 3 0.35 0.40 3-y follow-up 57 Low grade - > HPV-negative NILM 32,361 56 0.32 0.42 3-y follow-up 99 Colpo < CIN 2 CIN 3—>treatment HPV-negative ×3 1,314 4 0.44 0.44 3-y follow-up 59 Low grade - >Colpo < CIN 2 HPV-negative ALL 35,603 74 0.29 0.51 3-y follow-up 73 CIN 3—>treatment Cotest-negative ×2 2,087 7 0.58 0.68 1-y follow-up 68 HPV-negative/ASC-US HPV-negative ASC-US 1,701 11 0.42 0.78 1-y follow-up 82 HPV-negative HPV-negative LSIL 1,553 9 0.63 0.79 1-y follow-up 82 High grade - >Colpo < CIN 2 HPV-negative ALL 5,161 24 0.61 0.80 1-y follow-up 93This table lists clinical scenarios in 2019 guidelines, which have 5-year risk in a close interval around 0.55% (0.55% ± 0.25%).
 FIGURE 2: Increase in CIN 3+ risk from 3-year to 5-year among the test results which have 5-year CIN 3+ risk around 0.55%. Cumulative risk curve for scenarios with 5-year CIN 3+ risk around 0.55% with each color corresponding to a different scenario from Table 2. For these scenarios, we obtained the weighted average increase from years 3 to 5, weighted by frequency of occurrence as indicated by N in Table 2. The red line in the above figure is the estimated trend line showing the 0.16% increase from 3- to 5-year CIN 3+ risk, so the equivalent clinical action threshold for a 1-year follow-up is determined as 0.39% CIN 3+ 3-year risk (which is equivalent to 0.55% CIN 3+ 5-year risk threshold). Only scenarios with large numbers (10 or more) of observed CIN 3+ cases are plotted.Comparison of Clinical Recommendations Between 5- and 3-Year Risk Estimates
FIGURE 2: Increase in CIN 3+ risk from 3-year to 5-year among the test results which have 5-year CIN 3+ risk around 0.55%. Cumulative risk curve for scenarios with 5-year CIN 3+ risk around 0.55% with each color corresponding to a different scenario from Table 2. For these scenarios, we obtained the weighted average increase from years 3 to 5, weighted by frequency of occurrence as indicated by N in Table 2. The red line in the above figure is the estimated trend line showing the 0.16% increase from 3- to 5-year CIN 3+ risk, so the equivalent clinical action threshold for a 1-year follow-up is determined as 0.39% CIN 3+ 3-year risk (which is equivalent to 0.55% CIN 3+ 5-year risk threshold). Only scenarios with large numbers (10 or more) of observed CIN 3+ cases are plotted.Comparison of Clinical Recommendations Between 5- and 3-Year Risk Estimates
We examined whether any of the 2019 management recommendations would change when applying 3-year versus 5-year CIN 3+ risk thresholds. The scenarios in Table 3 serve as internal validation of the 3-year risk thresholds using the KPNC data set. We examined all clinical scenarios in the 2019 guidelines for which 1- and 3-year follow-up intervals are recommended using the following standards: a 3-year CIN 3+ risk of 0.09% was considered equivalent to a 5-year risk of 0.15% and a 3-year risk of 0.39% was considered equivalent to a 5-year risk of 0.55%. In 66 of the 67 follow-up scenarios (98.5%), the management recommendations using the 3-year risk thresholds were the same (see Table 3). The only scenario for which we observed different recommendations based on 5- versus 3-year risk thresholds was for individuals who are posttreatment and had 3 consecutive negative HPV tests. Based on the 2019 guidelines, 3-year follow-up is recommended for this scenario; however, according to the 3-year risk threshold, 1-year follow-up is recommended. This difference is likely due to the small number of outcomes in this group (4 CIN 3+ cases), resulting in imprecise risk estimates.
 TABLE 3:
TABLE 3: List of All Screening Test Results in the 2019 ASCCP Risk-Based Management Consensus Guidelines for Which 1-, 3-, and 5-Year Follow-up Is Recommended
Recommendation for Use of 3-Year Risk Estimates in the Enduring Guidelines ProcessThe following recommendations were accepted unanimously by the Enduring Guidelines Committee (Figure 3):
 FIGURE 3:
FIGURE 3: Updated risk-based management algorithm. The figure presented in the 2019 ASCCP Risk-Based Management Consensus Guidelines is updated according to this approved method presented in this report. If 5-year risk is not available for any screening test, the algorithm extends below, first checking whether 3-year CIN 3+ risk is available. If it is, the length of follow-up interval is determined by the new threshold at 3-year risk (0.39%). The recommendation is either 1- or 3-year return according to the 3-year risk of the patient. If 3-year risk is not also available, then the recommended management is to return in 1 year.
Immediate risks will be used to determine whether colposcopy or expedited treatment are recommended as outlined in the 2019 guidelines. This will apply to all new technologies. When immediate risks are less than 4% and fewer than 5 years of adequate follow-up data are available, 3-year equivalents of 5-year risk estimates may be used. o Repeat testing is recommended in 3 years for patients whose 3-year CIN 3+ risk is less than 0.39%. o Repeat testing is recommended in 1 year for patients whose 3-year CIN 3+ risk is 0.39% or greater and less than 4.0%. Return in 5 years will only be recommended when an adequate amount of 5 years of data are available for accurate risk estimation. Five-year risk estimates will be used preferentially over 3-year estimates when equivalent 5-year data are available. When insufficient data exist to estimate a 3-year CIN 3+ risk for a new technology that has been recommended, intervals for repeat testing cannot extend 1 year until additional follow-up data become available. DISCUSSIONRisk estimates underlying the 2019 ASCCP Risk-Based Management Consensus Guidelines were based on a large longitudinal data set, which consists of long-term observational screening and management data using cytology and HPV testing. However, most new technologies for cervical cancer screening and management will have fewer than 5 years of follow-up data at the time they are initially Food and Drug Administration approved. Only long-term clinical use will provide large-scale, long-term risk estimates. However, more widespread clinical adoption of new technologies will typically only happen after consensus guidelines for new technologies become available. Therefore, to facilitate the evaluation of new technologies for cervical screening and management, we developed a 3-year equivalent of 5-year CIN 3+ risk estimates adhering to the principle of equal management of equal risk. This new risk threshold based on 3-year data can determine whether a 1- or 3-year return is appropriate.
The Enduring Guidelines process is designed to incorporate new data and flexibly adapt guidelines at shorter intervals when new assays are approved and sufficient evidence is available. As additional data accrue for these new technologies, clinical recommendations based on 3- and 5-year risk thresholds can be evaluated and updated as needed. The risk thresholds outlined in the 2019 guidelines remain intact and will be used when adequate 5-year follow-up data are available. The 3-year risk estimates may also be preferable in situations when 5-year data are available, but scarce and underpowered, in which case 3-year risks can reduce uncertainty allowing for more robust recommendations. This is an extension of the methodology underlying the 2019 guidelines, not a new recommendation or a new risk threshold. The new approach allows determination of a 1- or 3-year follow-up interval when 3 years of data are available and recommend a follow-up interval of 1 year when fewer than 3 years of data are available.
The new 3-year risk thresholds were internally validated in the KPNC population and showed high agreement with the established 5-year thresholds. While external validation would be desirable, this is not possible currently because of a lack of comparable long-term risk data from other populations. While regulatory trials and observational studies may be limited to 3-year data, real-world clinical use of new technologies will ultimately provide more long-term risk estimates that can inform 5-year screening intervals. The Enduring Guidelines Committee will refine estimates when additional relevant data become available.
CONCLUSIONSWhen 5 years of follow-up data are not available, 3-year CIN 3+ risk estimates can be used to determine whether repeat testing in 1 or 3 years is appropriate.
REFERENCES 1. Perkins RB, Guido RS, Castle PE, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J Low Genit Tract Dis 2020;24:102–31. Erratum in: J Low Genit Tract Dis. 2020;24(4):427. 2. Egemen D, Cheung LC, Chen X, et al. Risk estimates supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines. J Low Genit Tract Dis 2020;24:132–43. 3. Cheung LC, Egemen D, Chen X, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines: methods for risk estimation, recommended management, and validation. J Low Genit Tract Dis 2020;24:90–101. 4. Wentzensen N, Schiffman M, Palmer T, et al. Triage of HPV positive women in cervical cancer screening. J Clin Virol 2016;76 suppl 1(suppl 1):S49–55. 5. Wentzensen N, Arbyn M, Berkhof J, et al. Eurogin 2016 roadmap: how HPV knowledge is changing screening practice. Int J Cancer 2017;140:2192–200. 6. Cuschieri K, Ronco G, Lorincz A, et al. Eurogin roadmap 2017: triage strategies for the management of HPV-positive women in cervical screening programs. Int J Cancer 2018;143:735–45.
留言 (0)