
記住我
Psoriasis is a chronic immune-mediated multisystem disease arising from dysregulation of interleukin (IL)-23 and IL-17 signaling pathways.1 The two categories of skin manifestations both occur on the vulva: classic plaque type seen as red to purple well-demarcated lesions with silvery scale, and flexural or inverse psoriasis seen as erythema and fissures at skin folds.2–4 The incidence of vulvar psoriasis is unknown; up to 40% of psoriasis patients report genital involvement and 1%–7% attending specialist vulvar clinics receive a diagnosis of psoriasis.2 Vulvar inverse psoriasis has similar symptoms and examination to erosive or hypertrophic lichen planus (LP), dermatitis, and candidiasis.2,5 Exposure to irritants and frictional trauma exacerbates psoriasis and may provoke the Koebner phenomenon of new lesions appearing in previously unaffected skin.2,6
The clinical presentation of vulvovaginal candidiasis (VVC) differs depending on location and estrogen status. Reproductive-age women primarily have vaginal involvement with variable extension to vulvar skin, with chronic or recurrent VVC common in a healthy cohort.7–9 Postmenopausal women predominantly have cutaneous or intracrural candidiasis, usually associated with obesity, diabetes mellitus (DM), systemic or local immunosuppression, antibiotic exposure, and skin occlusion.10,11 Cutaneous candidiasis occurs across sexes, ages, and sites, accounting for 1%–7% of dermatology clinical encounters.10 In both cohorts, symptoms include itching, burning, dyspareunia, edema, rash, fissures, adherent debris, and abnormal discharge.7 Skin abnormalities range from subtle erythema to violaceous or macerated rash, sometimes with peripheral scale and/or satellite lesions.1,12 False-negative culture of vaginal swab or vulvar scrapings may occur if organism numbers are low, with recent exposure to antifungal medications, or if an uninvolved site is sampled.13
Histopathology of psoriasis and candidiasis both demonstrate corneal or subcorneal neutrophils, acanthosis, and dermal lymphocytic infiltrate.14,15 Budding cells and pseudohyphae of candidal organisms in the stratum corneum (SC) may be seen in candidiasis but not psoriasis.16 Organism detection is easier on periodic acid-Schiff (PAS) than hematoxylin and eosin (H&E) stains, but they may be sparse or absent even with obvious clinical and microbiologic disease.14
This common clinicopathologic presentation and a growing body of literature suggest an overlap in immunologic pathogenesis. The study’s aim is to explore the relationship of vulvar psoriasis and candidiasis to determine if these entities are distinguishable or intertwined.
METHODSThe NSW Health Pathology North, John Hunter Hospital database was searched for vulvar biopsies with 1) corneal and/or subcorneal neutrophils, 2) acanthosis, and 3) dermal lymphocytic infiltrate. The Hunter New England Research Ethics and Governance Unit approved this retrospective histopathologic series (2020/ETH01880), and signed written consent was obtained for use of clinical photographs. Inclusion criteria were biopsies from hair-bearing or hairless skin with all layers of epidermis and upper dermis for review. Exclusion criteria included age younger than 18 and unavailable or uninterpretable slides.
Review of H&E-stained slides yielded data on biopsy location, site, appearance of SC and granular cell layer, rete ridge regularity and morphology, and spongiosis. Hyperproliferation of the basal and suprabasal layers was deemed “basal proliferative zone” and noted as present or absent. Measurements were recorded of stratum corneum, suprapapillary, and epidermal thickness. Frequency of neutrophils in the SC was described as scattered, unifocal, or multifocal, and their presence in epidermis and papillary dermis was noted. Infiltrate was semiquantitatively characterized as scant, moderate, or marked, with cell types recorded in descending frequency and location assessed as band-like, perivascular, or diffuse. Dermal assessment included edema, fibrosis, and ectatic vessels. Review of PAS-stained slides checked for fungal organisms in or under the stratum corneum. When multiple biopsies from a single patient and site showed similar histology, data were collected from the most representative specimen.
Demographic data included specialist type, age, postmenopausal status, body mass index, DM, tobacco use, and immune dysfunction defined as autoimmune disease or immunosuppressive medications. Clinical information included symptoms and their duration, prereferral treatments, examination, comorbid vulvar dermatoses, impression, treatments, response, outcome, and duration of follow-up. Results of vulvovaginal swabs or vulvar skin scrapings performed prereferral or during specialist assessment were categorized as positive or negative for Candida albicans or not done. Descriptive statistics were performed and categorical data were compared with Fischer exact test.
RESULTSThere were 62 biopsies from women with a median age of 60 years (range 25–82); 5 (8%) patients were aged younger than 40. Vulvovaginal culture yielded C. albicans in 28 (45%), 26 (42%) were negative for C. albicans, and 8 (13%) lacked microbiologic assessment (Table 1). Two patients had vulvar scrapings; 1 resulted negative and 1 positive, both aligning with concurrent vaginal swab results. Two patients had Candida glabrata on vaginal microbiology; in both the specialist impression was psoriasis, and clinical improvement occurred without exposure to an antifungal. Specialist type, postmenopausal status, body mass index, duration of symptoms, and known extragenital psoriasis were similar across microbiologic groups. Culture-positive patients were more likely to have DM [16/28 (57%) vs 7/34 (21%); p = .004]. Tobacco use occurred in 1 patient with unknown status and was undocumented in 14. Four women identified as First Nations, 1 culture-positive and 3 negative. Seven had an immunosuppressive condition to include rheumatoid arthritis in 2 and 1 each with sarcoidosis, CREST, Sjogrens, multiple sclerosis, and myopathy; 4 were culture-positive, 2 negative, and 1 unknown.
TABLE 1 - Clinical Characteristics of Patients With Biopsies Showing Psoriasis or Mycosis, Stratified by Microbiology Results All = 62; n (%) C. albicans = 28; n (%) Negative = 26; n (%) Not available = 8; n (%) Specialist type Gynecology 47 (76) 23 (82) 20 (77) 4 (50) Gynecologic oncology 6 (10) 3 (11) 3 (11.5) 0 Dermatology 9 (14) 2 (7) 3 (11.5) 4 (50) Age, median y (range) 60 (25–82) 63 (31–82) 58 (25–76) 60 (47–71) Duration of symptoms, median mo (range) 12 (0–288) 12 (3–288) 18 (0–144) 12 (12–120) Postmenopausal status 45 (73) 22 (79) 16 (62) 7 (88) DM* Yes 23 (37) 16 (57) 6 (23) 1 (12.5) Unknown 6 (10) 1 (4) 2 (7) 3 (37.5) Body mass index <30 26 (42) 12 (43) 11 (42) 3 (37.5) 30–39 8 (13) 3 (11) 3 (12) 2 (25) ≥40 14 (23) 8 (29) 6 (23) 0 Unknown 14 (23) 5 (18) 6 (23) 3 (37.5) Extragenital psoriasis 6 (10) 1 (4) 5 (19) 0 Prereferral treatment a Topical corticosteroids 33 (53) 18 (64) 15 (58) 0 Topical antifungal 16 (26) 8 (29) 8 (31) 0 Systemic antifungal 7 (11) 3 (11) 4 (15) 0 Topical estrogen* 13 (21) 10 (36) 3 (12) 0 Antibiotic 4 (6) 2 (7) 2 (7) 0 None/unknown/other 21 (34) 6 (21) 7 (27) 8 (100) Symptom a Itch 42 (68) 17 (61) 21 (80) 4 (50) Pain* 21 (34) 17 (61) 3 (12) 1 (12.5) Abnormal discharge 7 (11) 2 (7) 4 (15) 1 (12.5) Nil/unknown 3 (5) 0 1 (4) 2 (25) Examination - color Red 52 (84) 26 (93) 20 (77) 6 (75) Gray-pink 3 (5) 0 3 (11.5) 0 Pallor 3 (5) 1 (3.5) 0 2 (25) Normal/unknown 4 (6) 1 (3.5) 3 (11.5) 0 Examination - additional feature a Plaque 14 (23) 5 (18) 7 (27) 2 (25) Edema 14 (23) 7 (25) 6 (23) 1 (12.5) Erosion or fissure 11 (18) 4 (14) 5 (19) 2 (25) Satellite lesions 6 (10) 4 (14) 2 (8) 0 None/atrophy/unknown 17 (28) 8 (29) 6 (23) 3 (37.5) Clinical impression, n (%) VVC* 33 (53) 24 (86) 7 (27) 2 (25) VVC and psoriasis 7 (11) 3 (11) 3 (12) 1 (12.5) Psoriasis* 11 (18) 1 (4) 7 (27) 3 (37.5) Dermatitis or lichen simplex* 10 (16) 0 7 (27) 3 (37.5) Nil/unknown 2 (3) 0 2 (8) 0 Biopsy location Labium majus 28 (45) 14 (50) 11 (42) 3 (37.5) Interlabial fold/labium minus 20 (31) 6 (21) 10 (39) 4 (50) Perineum/perianus 8 (13) 6 (21) 2 (8) 0 Mons/groin 6 (10) 2 (7) 3 (11.5) 1 (12.5) Treatment a Topical corticosteroids 39 (63) 19 (68) 17 (65) 3 (37.5) Systemic antifungal* 32 (52) 21 (75) 10 (38) 1 (12.5) Topical antifungal* 13 (21) 10 (36) 2 (8) 1 (12.5) Barrier ointment 17 (27) 4 (14) 7 (27) 1 (12.5) Topical estrogen 4 (6) 1 (4) 2 (8) 1 (12.5) None/unknown/other 12 (19) 3 (11) 9 (35) 5 (62.5) Treatment with combination of steroid and antifungal* 23 (37) 16 (57) 6 (23) 1 (12.5) Outcome Improved, treatment ceased 25 (40) 12 (43) 8 (31) 5 (62.5) Improved, maintenance therapy 25 (40) 11 (39) 14 (54) 0 Not improved 3 (5) 2 (3) 1 (4) 0 Unknown or no follow-up 9 (15) 3 (5) 3 (12) 3 (37.5) Follow-up, median mo (range) 6 (0–82) 7 (0–82) 6 (0–36) 12 (2–24)*p < .05.
aCases may have more than 1 symptom, examination feature, or treatment.
VVC indicates vulvovaginal candidiasis.
Preexisting vulvovaginal conditions occurred in 14 (23%). In those with C. albicans, 5/28 (18%) had lichen sclerosus (LS) or LP and 1 (4%) had vulvodynia. In the culture-negative group, 3/26 (11.5%) had LS or LP and 3 (12%) had desquamative inflammatory vaginitis. Of those with no microbiologic result, 1/8 (12.5%) each had LP, desquamative inflammatory vaginitis, and high-grade squamous epithelial lesion.
Before specialist referral, 6 (21%) culture-positive women received a combination of topical corticosteroids and topical or systemic antifungals. Of these, 3 used betamethasone dipropionate and clotrimazole, 2 applied low- to medium-potency steroid with clotrimazole, 1 used betamethasone dipropionate and fluconazole, and 1 had hydrocortisone plus oral terbinafine. Among culture-negative women, 5 received combination regimens; 4 had a low- to medium-potency corticosteroid with clotrimazole, and 1 used betamethasone dipropionate and oral terbinafine. Referrers were more likely to provide topical estrogen to those who subsequently grew C. albicans [10/28 (36%) vs 3/34 (9%); p = .013].
Although rates of itch and abnormal discharge were similar across microbiologic groups, pain occurred more often in culture-positive women [17/28 (61%) vs 4/34 (12%); p = .0001]. Erythema was the most frequent examination finding, with variable documentation of additional descriptors like edema, erosion, fissure, and satellite lesions (Figures 1–3). Clinicians noted groin involvement in 4 each of culture-positive and negative groups.
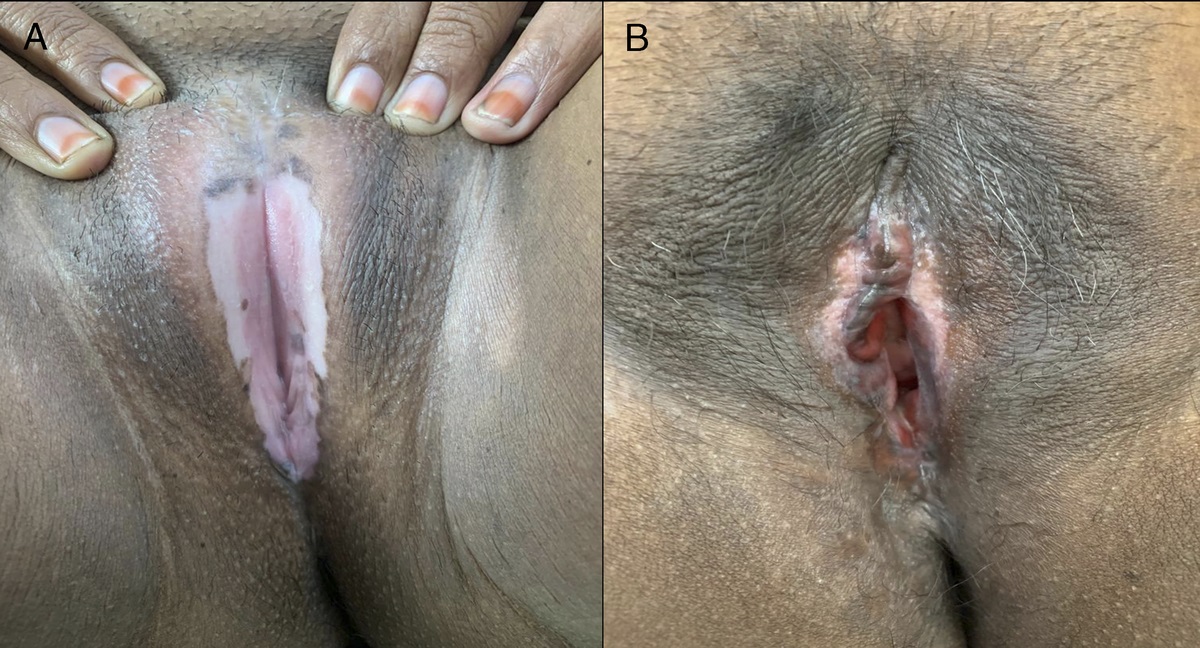
 FIGURE 1:
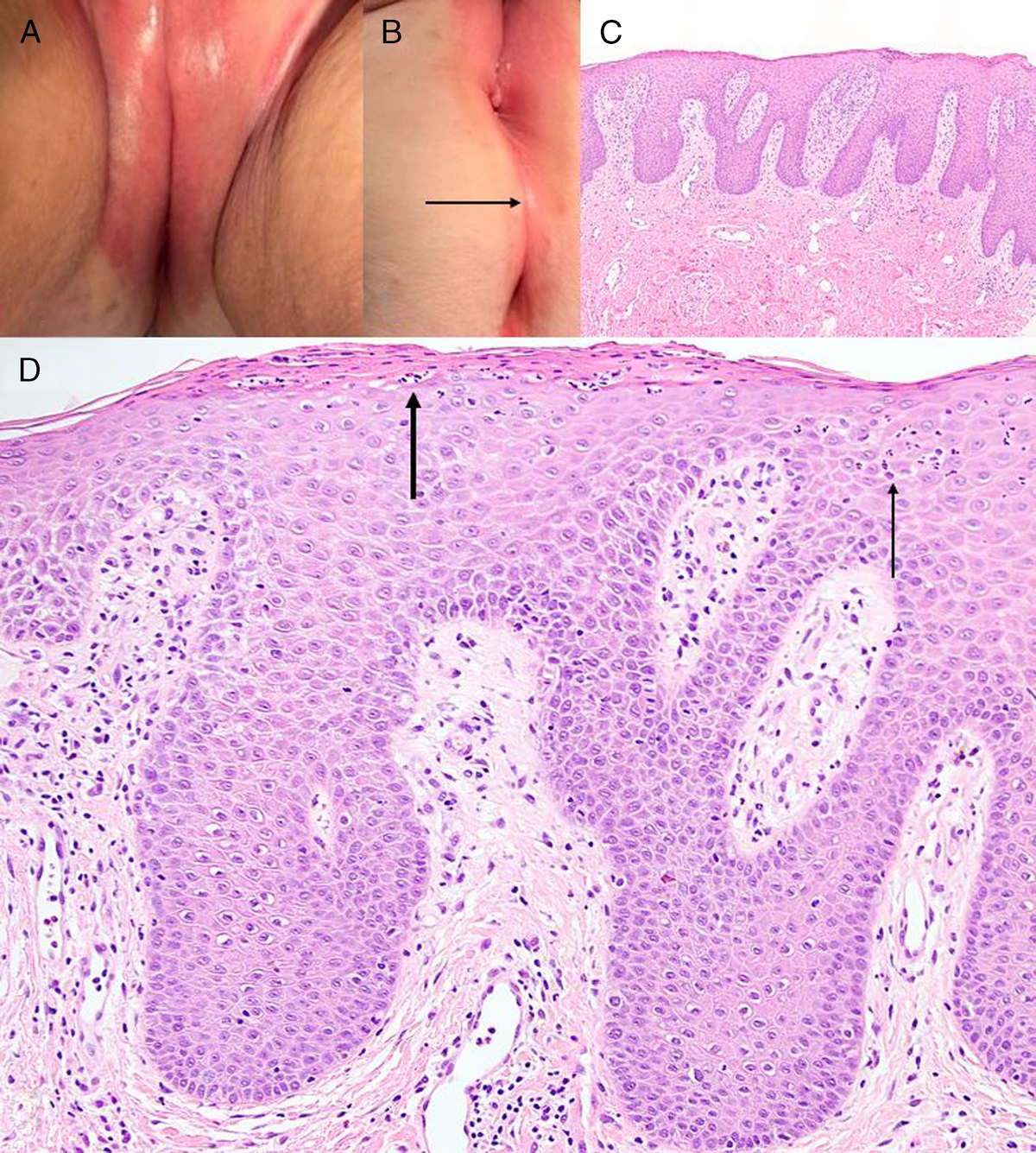
FIGURE 1: A 69-year-old with obesity and scalp psoriasis presented with 2 years of vulvar itch and pain; vulvovaginal culture was negative, clinical impression was comorbid psoriasis and candidiasis that improved with fluconazole and methylprednisolone aceponate ointment treatment then maintenance. A, vulvar erythema and edema extending to groins. B, moderately demarcated symmetric erythema over perianal skin and natal cleft (arrow). C, biopsy of labium majus shows hair-bearing skin with thin confluent parakeratosis (PK), hypogranulosis, acanthosis with elongated rete ridges, and papillary perivascular lymphocytic infiltrate; hematoxylin and eosin (H&E) ×40. D, subcorneal neutrophils (thick arrow), spongiosis, and epidermal neutrophils (thin arrow), periodic acid-Schiff (PAS) negative for organisms; H&E ×100.
 FIGURE 2:
FIGURE 2: A 55-year-old postmenopausal woman with obesity and diabetes mellitus (DM) presented with 1 year of vulvar itch and pain; vulvovaginal culture grew Candida albicans, clinical impression was candidiasis that resolved with fluconazole and hydrocortisone ointment. A, confluent vulvar erythema and edema over hairless and hair-bearing skin extending to medial labia majora. B, biopsy of perineum diagnostic of mycosis shows hair-bearing skin, PK, subcorneal pustules (thick arrows), acanthosis, spongiosis, and dermal lymphocytic infiltrate; H&E ×100. C, PAS ×200 shows fungal elements in stratum corneum (thin arrow).
 FIGURE 3:
FIGURE 3: A 41-year-old premenopausal woman with obesity, autoimmune disease on a biologic, and recent antibiotic use presented with 1 year of pain and abnormal discharge; vulvovaginal culture was negative, clinical impression was candidiasis that resolved with fluconazole and betamethasone dipropionate ointment. A, extensive nonconfluent erythema, edema, scale, and satellite lesions over vulva, groins, and inner thigh. B, biopsy of interlabial fold shows hair-bearing skin, acanthosis with regular rete ridges, and perivascular lymphocytic infiltrate; H&E ×40. C, thin confluent PK, hypogranulosis, corneal pustule (thick arrow), suprapapillary neutrophils (thin arrow), PAS negative for organisms; H&E ×100.
After history, examination, and investigations, clinical impression of cutaneous candidiasis was more likely with C. albicans identified [24/28 (86%) vs 9/34 (26%), p = .0001], whereas diagnoses of psoriasis [1/28 (4%) vs 10/34 (29%); p = .009] or dermatitis [0% vs 10/34 (29%) p = .0013] were more common in culture-negative women. There were 7 diagnoses of comorbid psoriasis and candidiasis (Figure 1). Among 6 with history of psoriasis, 1 (17%) had organisms on histology and 1 was culture-positive for C. albicans.
Specialist provision of systemic antifungals was more likely in Candida-positive women [21/28 (75%) vs 11/33 (33%); p = .001]; prescription of topical antifungals occurred less than half as often as oral therapy but was likewise more frequent in the culture-positive group [10/28 (36%) vs 3/34 (9%); p = .013]. Common fluconazole regimens were 50–100 mg daily for 2–6 weeks. Specialists provided antifungals to all but 1 in the C. albicans group, of whom 11 also received a topical corticosteroid and 5 had ongoing potent steroid treatment of lichenoid dermatosis. Combination regimens were more common in the culture-positive group [11/28 (39%) vs 5/34 (15%); p = .04] and included a potent steroid with fluconazole in 5/11 (24%), a low- to medium-potency steroid with fluconazole in 4 (36%), and 1 each (9%) received clotrimazole with a medium- or high-potency steroid. In the culture-negative and unknown groups, 2 had fluconazole plus ongoing potent steroid treatment of lichenoid dermatosis and 5 had combination regimens comprised of fluconazole paired with potent steroid in 3 or medium potency in 2. Additional treatments in 3 Candida-positive patients were intramuscular medroxyprogesterone, tricyclic antidepressant, and antiviral. Adjunctive management in culture-negative and unknown groups included menopause replacement therapy in 2; topical clindamycin in 2; and 1 each of antiviral, antihistamine, methotrexate for LP, tricyclic antidepressant, pelvic floor physiotherapy, and laser for high-grade squamous epithelial lesion. Women were equally likely to use maintenance therapy as to cease treatment, regardless of culture result.
Fungal organisms were seen on H&E and PAS in 9/16 (56%) cases, PAS in 6 (11%) cases, and H&E in 1 (6%) with PAS failure (Figure 2). Diabetes [10/16 (62.5%) vs 13/46 (28%) p = .02] and satellite lesions [6/16 (37.5%) vs 2/46 (4%); p = .03] were more common in organism-positive cases. Microbiologic presence of C. albicans [12/16 (75%) vs 16/46 (35%); p = .08] and prereferral exposure to topical corticosteroids [13/16 (81%) vs 22/46 (48%); p = .04] were associated with organisms on histology. Clinicians more often provided systemic antifungals to those with microscopic organisms than without [13/16 (81%) vs 20/46 (43%); p = .01]. The remaining positive cases received clotrimazole; all responded to antifungal therapy and 7/16 (44%) continued maintenance regimens.
Histopathologic findings were similar when stratified by microbiologic result (Table 2) and presence of organisms in the stratum corneum. Most biopsies were obtained from hair-bearing skin and showed parakeratosis, hypogranulosis or agranulocytosis, elongated rete ridges with suprapapillary thinning, corneal or subcorneal neutrophils, neutrophils peppered through epidermis and dermis, and dermal lymphocytes (Figures 1–3). Erosion or ulcer was seen in 5 (8%) with 3 in the C. albicans and 2 in the unknown groups. Eosinophils were absent in 39 (63%), sparse in 22 (35%), and frequent in 1 (2%) case with negative PAS and positive culture; there was no difference between groups. The frequency of epidermal neutrophils, morphology of rete ridges, presence of spongiosis, location of infiltrate, and dermal plasma cells was similar across microbiologic groups. Dermal edema occurred in 15 (24%), dermal fibrosis in 18 (29%), pigment incontinence or hemosiderin in 18 (29%), and dilated capillaries in 12 (19%), with no difference between microbiologic groups.
TABLE 2 - Histopathologic Characteristics of Biopsies Showing Psoriasis or Mycosis, Stratified by Microbiology Result All = 62; n (%) C. albicans = 28; n (%) Negative = 26; n (%) Not available = 8; n (%) Site Hair-bearing skin 52 (84) 26 (93) 20 (77) 6 (75) Hairless skin 10 (16) 2 (7) 6 (23) 2 (25) SC PK alone 33 (53) 18 (64) 9 (35) 6 (75) PK and HK 9 (15) 5 (18) 3 (12) 1 (12.5) PK or HK and normal 20 (33) 5 (18) 14 (54) 1 (12.5) Organisms in SC* 16 (26) 12 (43) 3 (12) 1 (12.5) Granular cell layer Agranulocytosis 31 (50) 17 (61) 9 (35) 5 (62.5) Hypogranulosis 27 (44) 11 (39) 14 (54) 2 (25) Hypergranulosis 1 (2) 0 1 (4) 0 Combination 3 (5) 0 2 (8) 1 (12.5) Epithelial thickness, mm; median (range) 0.4 (0.12–2) 0.42 (0.17–0.72) 0.4 (0.12–2) 0.43 (0.12–0.82) Suprapapillary thickness 0.08 (0.01–0.48) 0.08 (0.02–0.4) 0.08 (0.03–0.48) 0.07 (0.01–0.14) SC neutrophils Many or multifocal 35 (56) 18 (64) 13 (50) 4 (50) Scattered foci 5 (8) 2 (7) 2 (8) 1 (12.5) Scant 22 (35) 8 (29) 11 (42) 3 (37.5) Epithelial neutrophils None or rare 13 (21) 4 (14) 6 (23) 3 (37.5) Moderate 33 (53) 14 (50) 14 (54) 5 (62.5) Many 16 (26) 10 (36) 6 (23) 0 Basal layer proliferative zone present 42 (68) 20 (71) 19 (73) 3 (37.5) Rete ridges Regular/psoriasiform 27 (44) 13 (46) 10 (38) 4 (50) Irregular 35 (56) 15 (54) 16 (62) 4 (50) Spongiosis Present 40 (65) 16 (57) 16 (62) 8 (100) Marked 9 (15) 5 (18) 4 (15) 0 Dermal infiltrate Sparse 18 (29) 7 (25) 9 (35) 2 (25) Moderate 28 (45) 13 (46) 12 (46) 3 (37.5) Dense 16 (26) 8 (29) 5 (19) 3 (37.5) Infiltrate pattern Perivascular
留言 (0)