
記住我
Vaginitis is a frequent condition in women of childbearing age and is responsible for approximately 50% of outpatient consultations in gynecological offices.1 Typical symptoms include vulvovaginal itching, discharge, irritation, dyspareunia, and unpleasant odor. These symptoms can be traced back to one of the following 4 entities: vulvovaginal candidiasis (VVC), bacterial vaginosis (BV), desquamative inflammatory vaginitis/aerobic vaginitis (DIV/AV), and trichomoniasis.2 Nevertheless, there are other and less common causes for these symptoms, such as cytolytic vaginosis, although the existence of this condition is rather controversial.3
Vulvovaginal candidiasis, or less often referred to as candidosis, is a common vaginal infection, with 75% of all patients reporting at least 1 episode of VVC in their life.4 In 80%–95% of all symptomatic cases, VVC is caused by Candida albicans.5 Vulvovaginal candidiasis can often be suspected clinically, although clinical diagnoses are associated with high error rates. Hence, it is recommended to verify the diagnosis of VVC by the identification of pseudohyphae on phase-contrast microscopy; further diagnostic measures include cultural diagnosis and the use of multiplex polymerase chain reaction, which are both of highest importance in complex and recurrent cases. Fungal culture, however, is still considered the criterion standard for VVC diagnosis.6–9
Bacterial vaginosis is widely considered a form of vaginal dysbiosis and the most common bacterial syndrome of the vagina.4 Pathogens most frequently associated with BV are Gram-negative Gardnerella species, Fannyhessea vaginae, and other BV-associated bacteria.10,11 In most cases, BV can be suspected using the Amsel criteria: homogeneous, grayish-white discharge, vaginal pH of 4.5 or higher, positive amine whiff test, and the presence of clue cells on microscopy.12 Microscopic evaluation of Gram-stained smears and determination of the Nugent score is widely considered the criterion standard method for BV diagnosis. The Hay-Ison criteria represent another simplified and effective method for BV diagnosis.13 Bacterial vaginosis treatment is recommended for symptomatic patients, apart from an ongoing discussion on the screening and treatment of asymptomatic BV in pregnant women due to their increased risk of preterm birth; currently, recommendations on this topic are inconsistent.14–16
Inflammatory states of the vagina that occur less frequently include DIV/AV, which is characterized by an increased vaginal pH, vaginal leucocytosis, and a highly disturbed vaginal microbiota caused by aerobic bacteria such as Staphylococcus spp. or Escherichia coli. To date, no standard treatment has been implemented for this special entity.17 Trichomoniasis, an infection by the protozoan Trichomonas vaginalis, should be treated with metronidazole for both the affected patient and his/her sexual partner/s.18
From a clinical perspective, the exact diagnosis of the specific etiology that causes symptoms of vulvovaginal infection demands special equipment and skilled personnel, which might result in a financial burden because these resources are frequently not available at the primary point of care.19 Indeed, standard treatment with antimycotic and/or antibiotic agents requires exact diagnosis of the underlying etiology, which might pose a challenge during difficulties in differentiating between colonization, contamination, and infection.7,14,20 The required effort and expense might also significantly delay the treatment.19 Therefore, not only easy and affordable diagnostic measures, such as wet mount microscopy, but also rapidly available point-of-care tests might be important in clinical routine.8,19,21
The antiseptic agent dequalinium chloride (DQC), which is a quaternary ammonium salt, possesses a broad spectrum of antimicrobial efficacy, as well as anti-inflammatory effects through the inhibition of protein kinase C.22,23 The antimicrobial effect of DQC results from multiple modes of action. It has mitochondriotropic properties, leading to DNA depletion and inhibition of energy production in cells; it can lead to protein denaturation, thereby affecting ribosomal protein synthesis; and it increases cell permeability, which results in a loss of enzyme activity and microbial membrane lysis depending on the concentration.23–26 In addition, in vitro studies show that DQC can effectively disrupt biofilms that play a vital role in the pathophysiology of vaginal infections associated with pathogens such as Gardnerella species.27 The efficacy against other leading pathogens such as T. vaginalis or Candida albicans has also been shown in in vitro studies.23 The clinical efficacy of DQC as a treatment option for different vaginal infections has been evaluated in several studies in recent years.2,28–31 We conducted this systematic review and meta-analysis to evaluate whether DQC is comparable with the reference treatment of various vaginal infections.
METHODS Search Strategy and Data SourcesThis systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.32 The databases PubMed/MEDLINE, EMBASE, CENTRAL (Cochrane Library), and clinicaltrials.gov were searched for studies on DQC, local anti-infective agents, vaginal antiseptics, BV, VVC, and other vaginal infections. The search was conducted until October 2022. Table S1, https://links.lww.com/LGT/A330, presents the defined search terms. The references of all retrieved reviews were evaluated for additional studies.
Eligibility Criteria and Study SelectionThis systematic review included cohort and randomized controlled studies exclusively. All retrieved results were independently reviewed by 2 researchers for eligibility (F.E. and K.K.F.). In cases of disagreement between the 2 researchers, eligibility was determined by senior researchers (P.F. and A.F.). To be considered eligible, a study had to (i) examine the efficacy of DQC vaginal tablets in one of the following vaginal infections: VVC, BV, DIV/AV, or trichomoniasis; (ii) include a control group (only applicable for inclusion in the meta-analysis); and (iii) provide exact data to extract efficacy. Exclusion criteria were (i) a high risk of bias according to the Newcastle-Ottawa Scale (NOS) and (ii) unsuitable study design, such as case reports or systematic reviews. Titles and abstracts were screened for eligibility during the first round according to the PRISMA guidelines. The final selection was determined in the second round after a full-text assessment.
Risk-of-Bias Assessment and Data CollectionWe used a standardized extraction form for data collection. The data obtained included the first author's name, period during which the study was conducted, country in which the study was conducted, study design, number of treated patients (DQC vs reference treatment), adverse events, and study outcome measures. Two researchers (F.E. and K.K.F.) independently collected the data, and discrepancies were resolved by the senior researchers (P.F. and A.F.). We used the NOS for randomized controlled trials and observational studies to assess the possible risk of bias.33,34 We then evaluated the quality of study using criteria ranging from 0 (high risk of bias) to 9 points (low risk of bias). Studies with 7 points or higher were considered high quality and had a low risk of bias. The risk of bias was independently assessed by 2 researchers (F.E. and K.K.F.), and discrepancies were resolved by the senior researchers (P.F. and A.F.).
Aims and Working HypothesisOur primary aim was to evaluate the efficacy of vaginally applied DQC as a treatment option compared with standard treatment for vaginal infections of 1 of the following 4 etiologies: VVC, BV, DIV/AV, and trichomoniasis. Standard treatment was defined as antibiotics, antifungal medication, or another local antiseptic agent. The secondary aim was to evaluate the safety and tolerability of this agent. As a hypothesis, we assume that DQC is noninferior to the standard treatment option.
Data Synthesis and Meta-analysisNarrative synthesis was the primary reporting method used in this review. For meta-analysis, we calculated forest plots using Review Manager 5.4.1 (The Cochrane Collaboration, London, UK). We applied the Mantel-Haenszel method to calculate the odds ratio (OR). The chi-square test was used to evaluate the heterogeneity of intervention effects to assess whether the results of included studies were consistent, and the summary effect was calculated using a z test.
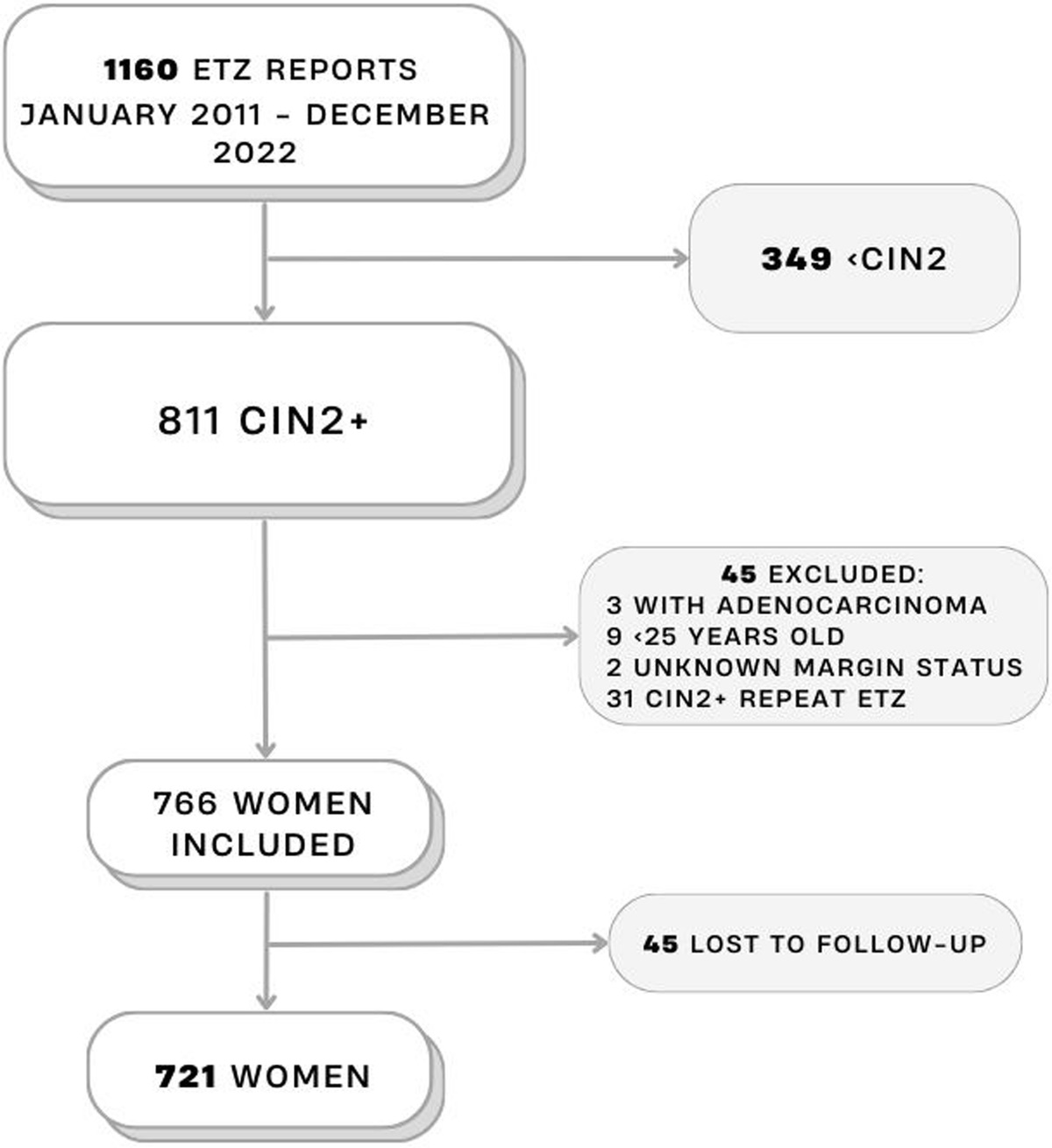
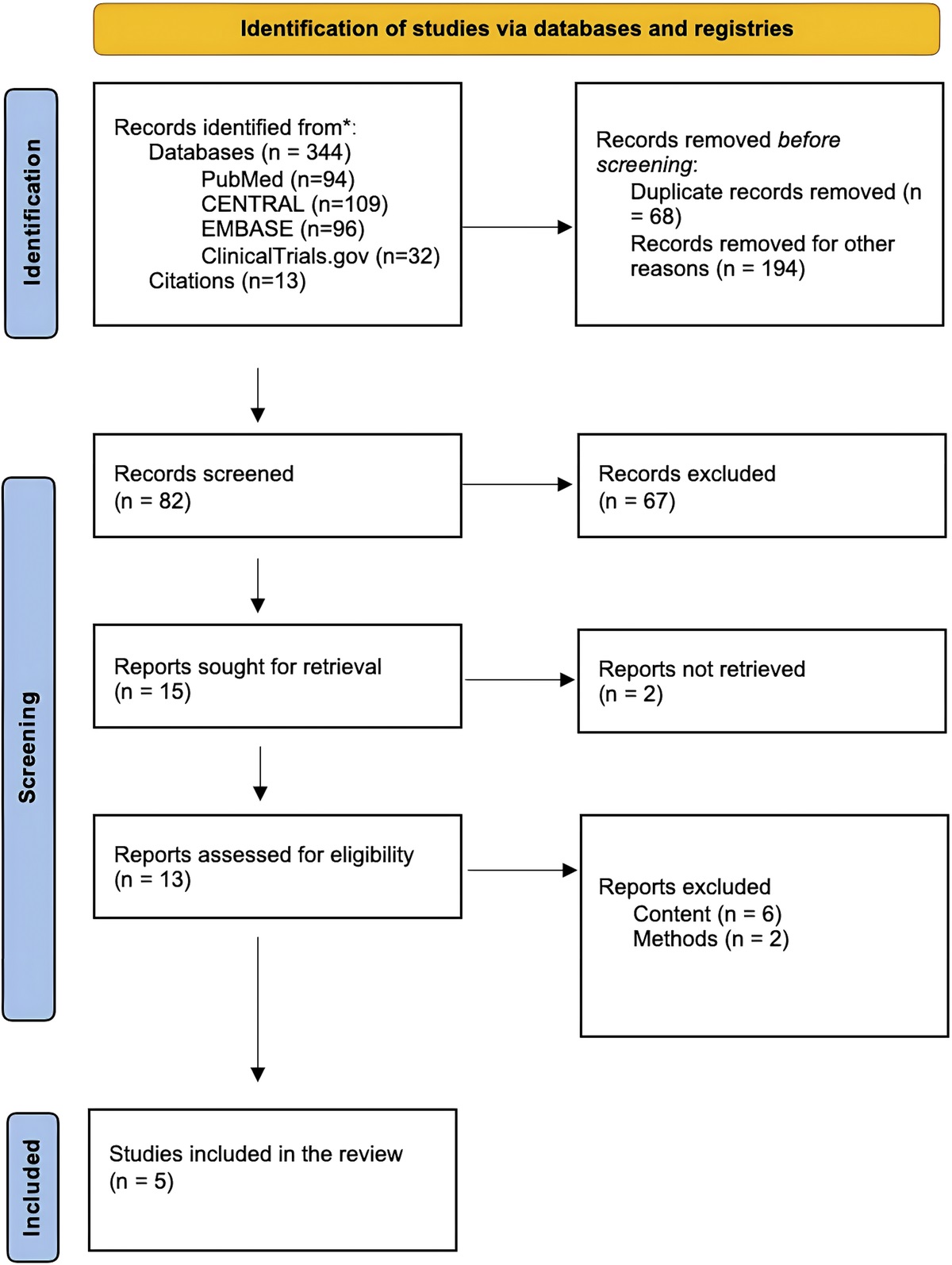
RESULTS Search ResultsA total of 344 records were identified by initial literature research. References of identified reviews were also evaluated, not resulting in any additional records of relevance. After removing duplicates and conducting thorough screening of titles and abstracts, 329 records were removed and 15 records were sought for retrieval, 10 records had to be excluded after full-text evaluation. The remaining 16 articles were sought for retrieval and full-text evaluation. After evaluating the full texts, 11 records had to be excluded due to either wrong article types or irrelevant content. Finally, 5 studies (4 randomized controlled trials and 1 observational study) were included in the review for further evaluation.2,28–31 Three of these qualified for inclusion in the meta-analysis.2,30,31 The other 2 studies were excluded from the meta-analysis owing to the lack of a control group and insufficient efficacy data.28,29 The study selection process is shown in Figure 1. All included trials were conducted between 1993 and 2016. In total, 1,416 patients with vaginitis of different etiologies were included in these studies, of which 1,115 had BV, 185 had VVC, 144 had DIV/AV, and 7 had trichomoniasis. A total of 1,005 patients were treated with DQC, whereas others received a reference treatment or placebo. The characteristics of included trials are shown in Tables 1, 2, and 3 according to their entity. Because some of the included studies examined multiple vaginal infections, the patient numbers for each etiology were extracted and sorted into individual tables: 1 for BV (Table 1), 1 for VVC (Table 2), and 1 for less common conditions (Table 3). Because the results for each etiology will be discussed separately, articles including several etiologies will be discussed multiple times, regarding their results for each etiology individually.
 FIGURE 1:
FIGURE 1: Study selection process.
TABLE 1 - Characteristics of the 4 Included Studies on Bacterial Vaginosis Donders et al.29 Petersen et al.2 Vives et al.28 Weissenbacher et al.31 Country Uganda Germany/Switzerland Spain Multinational (Europe) Study design Randomized, controlled trial Randomized, controlled trial Observational study Randomized, controlled trial Duration n/a September 1993 until July 1995 October 2015 until May 2016 January 2007 until July 2008 Sample Size 148 73 573 321 Stratification Change in BV score after treatment with DQC vs rifaximin vs placebo Change in total symptom score 5–7 d and 3–4 wk after treatment with DQC vs povidone iodine 1) Characterization of BV in Spanish women; 2) symptom relief of patients with BV after treatment with DQC; 3) patient satisfaction after treatment with DQC Comparison of effectiveness of DQC and clindamycin as topical treatment for BV Dequalinium exposure 49 48 573 164 Duration of treatment with DQC in days 6 6 6 6 Control treatment exposure 48 (rifaximin) 25 (povidone iodine) — 157 (clindamycin) Duration of reference treatment in days 6 6 — 7 Definition of cure Predefined BV score Global efficacy score Absence of symptoms Absence of clue cells and no more than 1 positive Amsel criterium Adverse events n/a 7 (mild) 25 (mild) 66 (mild/related)BV indicates bacterial vaginosis; DQC, dequalinium chloride; n/a, non-applicable.
VVC indicates vulvovaginal candidiasis.
DIV/AV indicates desquamative inflammatory vaginitis/aerobic vaginitis.
The NOS that determined the risk of bias in the included trials revealed that one of the randomized controlled trials was scored with the highest possible result of 9 points.2,29 The other randomized studies and the observational study28,30,31 were scored with 7 or 8 points, resulting in a low risk of bias in all 5 studies that were evaluated. The scores are reported in Tables 4 and 5.
TABLE 4 - Risk-of-Bias Assessment of the 4 Included Randomized Controlled Trials Using the Newcastle-Ottawa Scale Risk-of-Bias Assessment – Randomized Trials Donders et al.29 Petersen et al.2 Thamkantho et al.30 Weissenbacher et al.31 Case definition 0 1 1 1 Representativeness 1 1 1 1 Selection of controls 1 1 1 1 Definition of controls 1 1 1 1 Comparability 2 2 1 1 Ascertainment of exposure 1 1 1 1 Same method case and control 1 1 1 1 Nonresponse rate 1 1 1 1 Total score 8 9 8 8Four of the included studies examined the efficacy of DQC as BV treatment, whereof 3 were randomized controlled trials2,29,31 and 1 was an observational study.28 The characteristics of included studies are summarized in Table 1.
Vives et al.28 retrospectively analyzed the data of 573 Spanish BV patients who were treated with DQC (one 10-mg vaginal tablet per day for 6 d). The main end points were BV-associated symptoms defined as vaginal discharge, odor, pruritus, itching, leucorrhoea, erythema, pain, and edema after treatment. Almost 85% of the patients who were treated reported to be symptom-free 4–6 weeks after the diagnosis. Only 4.3% reported adverse effects, most of which were mild, such as vaginal discharge. Serious adverse events were not observed.
Donders et al.29 conducted a double-blinded randomized control study comparing the efficacy of DQC and rifaximin in asymptomatic women with BV. A total of 49 patients treated with DQC were compared with 48 patients treated with rifaximin as a reference treatment and another 51 patients who received placebo. All 3 treatment regimens were designed as a 6-day intravaginal treatment. Bacterial vaginosis was classified as the presence of either Gardnerella or Mobinculus species or clue cells with an additional lack of lactobacilli, equating to a Nugent score higher than 6. Taking into consideration the amount of clue cells present, a specific BV score was defined and used as a primary end point for efficacy measures. Both the treatments eliminated BV, with a significant difference compared with the placebo group, where BV was hardly eliminated. In addition, a positive effect of DQC on concomitant VVC compared with rifaximin was demonstrated.29
Petersen et al.2 conducted a double-blinded randomized controlled trial, evaluating the efficacy of DQC as a treatment for different vaginal infections. Regarding BV, the study compared the treatment efficacy on 48 patients treated with DQC to 25 treated with povidone iodine as reference treatment. The medication regimen was identical for both substances, with 1 vaginal tablet per day for 6 days. The dosage was 10 mg for DQC and 200 mg for povidone iodine. Bacterial vaginosis was diagnosed when at least 3 of the 4 Amsel criteria were fulfilled and Gardnerella spp. or other anaerobes were present in bacterial culture. In this study, multiple factors were assessed, including the degree of purity of the vaginal microbiota, a predefined 12-point symptom score, vaginal pH, bacterial cultures, and lactobacilli levels. Summarizing these factors and adding adverse events, efficacy and tolerability were globally assessed at 2 control visits (after 5–7 d and 3–4 wk). Noninferiority of DQC was shown for each of these outcomes, and in both groups, a 75% full or partial remission rate was noticed after 3–4 weeks. In addition, the study reported a higher remission rate at the first control visit, so a faster improvement in patients who received DQC than those in the control group.
The efficacy of vaginal clindamycin and DQC was compared in a multinational single-blinded randomized controlled study in 164 and 157 patients treated with DQC and clindamycin, respectively.31 Bacterial vaginosis was diagnosed when all 4 Amsel criteria were positive. The study group received a vaginal tablet of 10 mg DQC daily for 6 days, the control group received an application of 2% clindamycin vaginal cream once per day for 7 days. A clinical cure was defined as the absence of clue cells and no more than 1 positive Amsel criterium. The reported cure rates 3–4 weeks after treatment were 79.5% and 77.6% in the DQC and clindamycin groups, respectively. Several other factors, including the Amsel criteria, recurrence rate, and lactobacillary grade, were evaluated. The authors demonstrated noninferiority of DQC for each of the evaluated categories. A reduction in concomitant VVC was observed in the DQC group compared with a 2-fold increase in the clindamycin group, although this difference was not statistically significant. No serious adverse event occurred in those groups, with a rather good tolerability rate of “good” or “very good” in more than 90% for both agents. Notably, these numbers included the entire heterogeneous patient collective of this study, not only those with BV. In conclusion, our evaluated studies confirmed that DQC was noninferior to the examined reference treatments of BV, without the evidence of any serious adverse events.31
When performing the meta-analysis for BV, we found that only 2 studies were considered eligible.2,31 The studies by Vives et al. and Donders et al. were excluded owing to the lack of a control group and insufficient efficacy data.28,29 The study data are shown in Table S2.1, https://links.lww.com/LGT/A330. Both studies reported similar cure rates between 75% and 80% for DQC.2,31 We could not determine parameters for adverse events because Petersen et al. evaluated a very heterogeneous patient collective and did not provide numbers, particularly for BV patients. Statistical evaluation using a meta-analysis confirmed the noninferiority of DQC when being compared with the examined reference treatments for BV, with an OR of 1.01 and a 95% CI of 0.59–1.73, as shown in Figure 2.
 FIGURE 2:
FIGURE 2: Efficacy of dequalinium chloride for treating bacterial vaginosis compared to that of the standard treatment: results of the meta-analysis.
Vulvovaginal CandidiasisOf the randomized controlled trials that we included for further analyses, 2 examined the efficacy of DQC for treating VVC and compared it to the results of reference treatments.2,30 Their characteristics are presented in Table 2. Petersen et al.2 enrolled 35 women diagnosed with VVC in their study, out of which 23 were treated with DQC and compared the data to 12 patients treated with povidone iodine. Vulvovaginal candidiasis was diagnosed through the presence of yeasts in the wet mount or positive culture results for Candida spp. Medication regimens and efficacy assessment are described previously. Full or partial remission was observed in 84.2% of the DQC group, compared with 88.9% in the control group. A negative result for Candida in microbiological culture was achieved in 84.2% and 81.8% of patients in the DQC and control groups, respectively. Subanalysis of 2 control visits (5–7 d and 4–5 wk after the end of treatment) revealed noninferiority of the DQC group, showing that patients were more likely to experience early clinical improvement in the DQC group, compared with those in the control group.
Thamkantho et al.30 conducted a double-blinded randomized controlled study comparing the efficacy of DQC with clotrimazole in women with VVC. The diagnosis was confirmed by the detection of pseudohyphae in microscopic examination. Both medication regimens included 1 vaginal tablet (10 mg DQC, 100 mg clotrimazole) daily for a duration of 6 days. A total of 74 patients in the DQC group were compared with 76 patients in the clotrimazole group. Clinical cure was defined as a symptom score lower than 5 (maximum score, 12 points), including itching, soreness, discharge, and edema. Clinical cure was achieved in 84.9% and 85.1% of patients in the DQC and control groups (p = .985), respectively. This again indicated noninferiority of DQC in VVC patients compared with the reference treatment. However, patients treated with DQC were more likely to show positive Candida cultures than those who were treated with the standard (69.7% vs 36.6%, p < .001). No adverse events were described in both groups, and patient satisfaction was comparably high for both groups.30
Both of these studies by Petersen et al. and Thamkantho et al. were eligible for meta-analysis (Table S3, https://links.lww.com/LGT/A330).2,30 Vulvovaginal candidiasis cure rates were comparable in both studies, ranging from 75% to 85% in the DQC group. However, we were unable to perform calculations for adverse events because Petersen et al. did not offer the numbers, particularly for patients with VVC. Compared with the examined reference treatment, meta-analysis revealed an OR of 1.07 (95% CI = 0.33–3.47) as shown in Figure 3.
 FIGURE 3:
FIGURE 3: Efficacy of dequalinium chloride for treating vulvovaginal candidiasis compared to that of the standard treatment: results of the meta-analysis.
Other Vaginal ConditionsIn addition to BV and VVC, we reviewed 2 other etiologies of vaginal conditions: DIV/AV and trichomoniasis. Because these infections do not occur as frequently as BV and VVC, the number of cases included in the analyses was rather low. Therefore, we could not perform a meta-analysis, but the characteristics of the 2 studies that have been included are shown in Table 3.2,29 Donders et al.29 evaluated data of 79 patients diagnosed with DIV/AV. Desquamative inflammatory vaginitis/aerobic vaginitis was diagnosed via microscopic examination according to a specific predefined DIV/AV score including lactobacillary grades and other factors such as relative frequency of leucocytes compared with epitheliocytes. Twenty-four women were treated with DQC, 30 received the reference treatment with rifaximin, and the residual received placebo. The treatment regimen is described previously. Both treatments significantly improved DIV/AV symptoms compared with placebo. Petersen et al.2 enrolled 65 patients with DIV/AV and 7 with trichomoniasis. Trichomoniasis was diagnosed when Trichomonas vaginalis was detected in vaginal smears. Desquamative inflammatory vaginitis/aerobic vaginitis was defined as an abnormal vaginal microbiota without the necessary diagnostic criteria for BV, VVC, or trichomoniasis. Patients of both groups received DQC and povidone iodine in a 2:1 ratio, according to the treatment pattern that is described previously. In a global assessment, a complete or considerable improvement was observed in 77.1% and 64.3% patients in the DQC and control groups, respectively. For trichomoniasis, insufficient data were available to draw any conclusion regarding DQC as an effective treatment option. However, it was demonstrated that Trichomonas was eradicated in approximately 50% of the women in both treatment groups, which suggests an effect of DQC against trichomoniasis. Summarizing, DQC was demonstrated to be noninferior to the reference treatment in patients with DIV/AV, whereas the data were inconclusive for the treatment of trichomoniasis.
DISCUSSIONThis systematic review and meta-analysis assessed the efficacy of DQC in treating vaginal infections. Our review focused on acute vaginal infections because the literature on DQC as a maintenance therapy for chronic or recurrent infections is sparse. In this meta-analysis, we demonstrated noninferiority of DQC to the examined reference treatments for BV and VVC, although available data for VVC are limited. In addition, we found that DQC treatment was equivalent to the compared reference treatments for DIV/AV, although a meta-analysis could not be conducted in this subgroup owing to insufficient data.
The local antiseptic agent DQC shows antimicrobial and potentially antifungal effects to treat pathogens that cause vaginal infections.22 It is widely known as a locally applied treatment option with a generally well tolerance; only few mild adverse events have been described, such as itching, discharge, or light vaginal bleeding.2,28–31 Several studies regarding its efficacy have been conducted; however, to the best of our knowledge, no recent systematic review and meta-analysis have yet been conducted to assess the efficacy of DQC treatment for vaginal infections.
We found several advantages of treatment with DQC, for example, it seems to have a positive effect on the course and development of concomitant VVC in treating patients who are experiencing BV, compared with that of antibiotic treatment.29,31 Incorrect self-diagnosis and self-treatment of vaginal infections, particularly with over-the-counter antifungal medication, is currently a widespread issue.35 Diagnostic workup for vaginal infections is crucial; however, it might be complicated owing to the need for trained staff and specialized equipment. Furthermore, because standard diagnostics usually require transport to a laboratory and Gram staining, the diagnosis and treatment might be significantly delayed.8,19 Dequalinium chloride has the advantage of having a broader antimicrobial spectrum than standard treatments, regardless of the fact that treatment should always follow proper diagnostic workup.22 Of note, self-treatment is not widely recommended, and treatment should always follow evaluation by medical personnel.20
Interestingly, we found contradictory results regarding the abundance of Candida species in fungal cultures after treatment. Thamkantho et al.30 reported significantly more positive fungal cultures after DQC treatment than after standard treatment, although clinical cure rates were equivalent. However, the clinical implications of this finding are questionable because asymptomatic colonization with Candida should not be considered as an indication for treatment.7
The standard treatment for vaginal infections depends on the underlying etiology. The guidelines of the Centers for Disease Control and Prevention (CDC), the Working Group of Scientific Medical Societies (AWMF), as well as the International Society for the Study of Vulvovaginal Disease (ISSVD) recommend that the first-line treatment for BV should be oral or topical metronidazole or clindamycin.15,36,37 In uncomplicated VVC, oral or topical azoles, such as clotrimazole or fluconazole, are recommended as standard treatment.6,20,37
A rapid increase in resistances to antibiotic or antifungal agents has been discovered over the last decades. This problem is especially severe in low- and middle-income countries, where the rate of multiresistant infections is expected to grow 4–7 times faster than in other regions. It has been estimated that in some countries up to 40%–60% of all infections are caused by resistant pathogens.38 Furthermore, over the last decades, the development of new antibiotic agents has increasingly slowed down.39 Owing to the increase in multiresistant pathogens and the burden of resistance to antibiotic and antifungal treatment options, a broader variety of treatment options would generally be desirable.2,17,31 Although the etiology of recurrent vaginal infections is not fully understood yet, resistance to antibiotics and antifungal agents is definitely a contributing factor. In addition, women with recurrent infections often need to be treated with high doses of antimycotic or antibiotic medication over long periods.40,41 Antiseptic agents could offer a possible treatment alternative, thereby controlling the increasing rates of antimicrobial resistance.
Our systematic review and meta-analysis has several strengths. First, it has been conducted following the PRISMA guidelines, including trials with a low risk of bias only, according to the NOS. Second, in addition to 1 observational study, all the included studies were randomized controlled trials, suggesting the highest level of scientific evidence. Limitations of our study include the small number of available studies examining the efficacy of DQC, as well as the lack of data and unclear definition of adverse events in the included studies. Moreover, data to conduct a meta-analysis on the efficacy of DQC in treating DIV/AV or trichomoniasis were insufficient, which would have, however, also been of interest. This is probably owing to the comparatively low prevalence of DIV/AV and trichomoniasis.42,43 Another limitation was that some of the reference treatments used for the control groups in the included studies, such as rifaximin and povidone iodine, are not considered first-line treatment options in these cases.15
We are aware that the available studies investigating the efficacy of DQC for vaginal infections are very heterogenous. A possible factor explaining this issue is that DQC is available as a treatment for different vaginal infections. Many studies therefore do not address a single etiology rather than
留言 (0)