Objective
Our aim was to evaluate the performance of different follow-up strategies after treatment for cervical intraepithelial neoplasia (CIN) 2 or 3, including human papillomavirus (HPV) detection, cytology, or colposcopy, as well as their combinations. Additionally, we compared the influence of the persistence of HPV 16/18 versus that of other high-risk HPV genotypes (HR-HPV) in the recurrence risk.
Methods
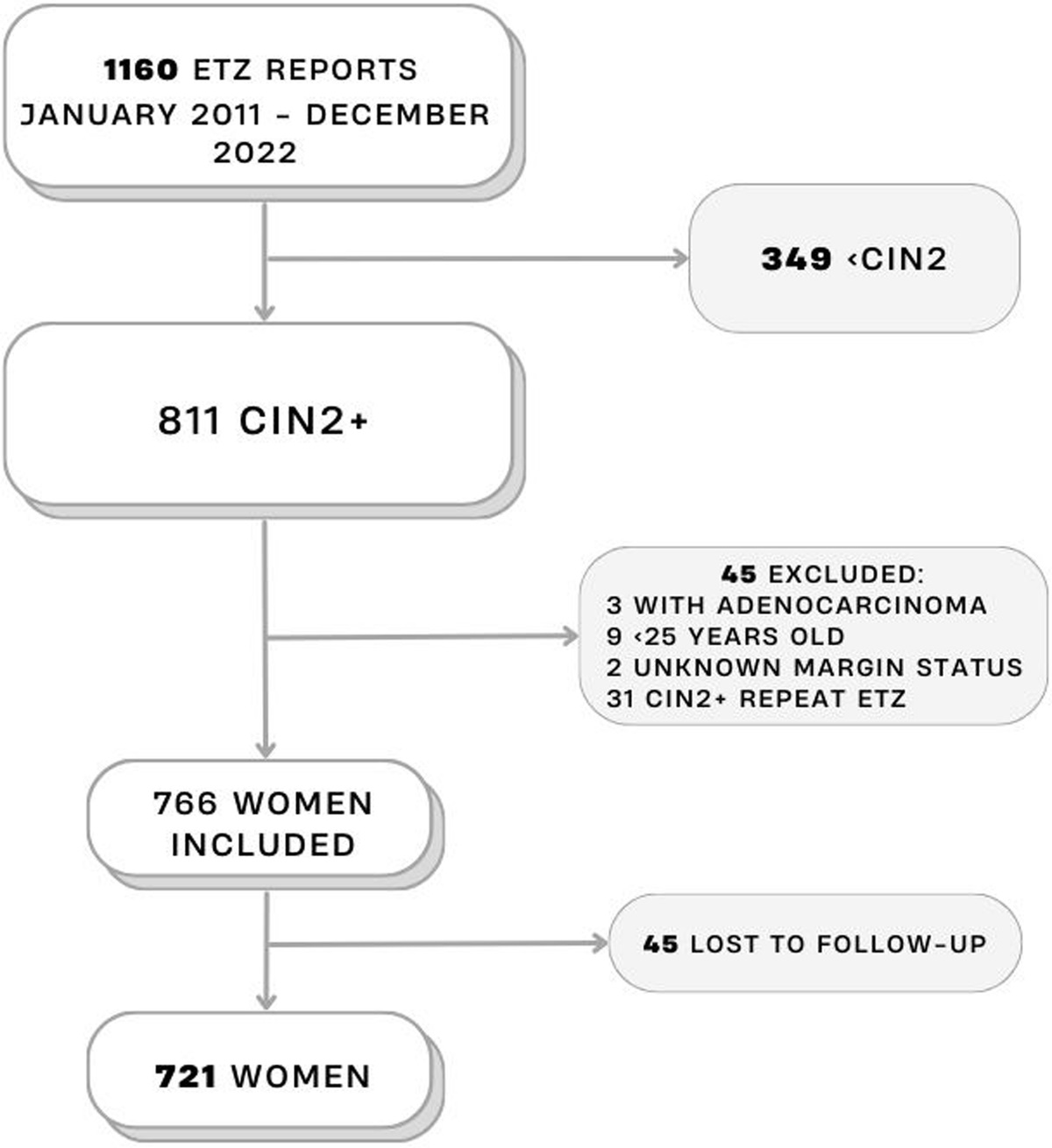
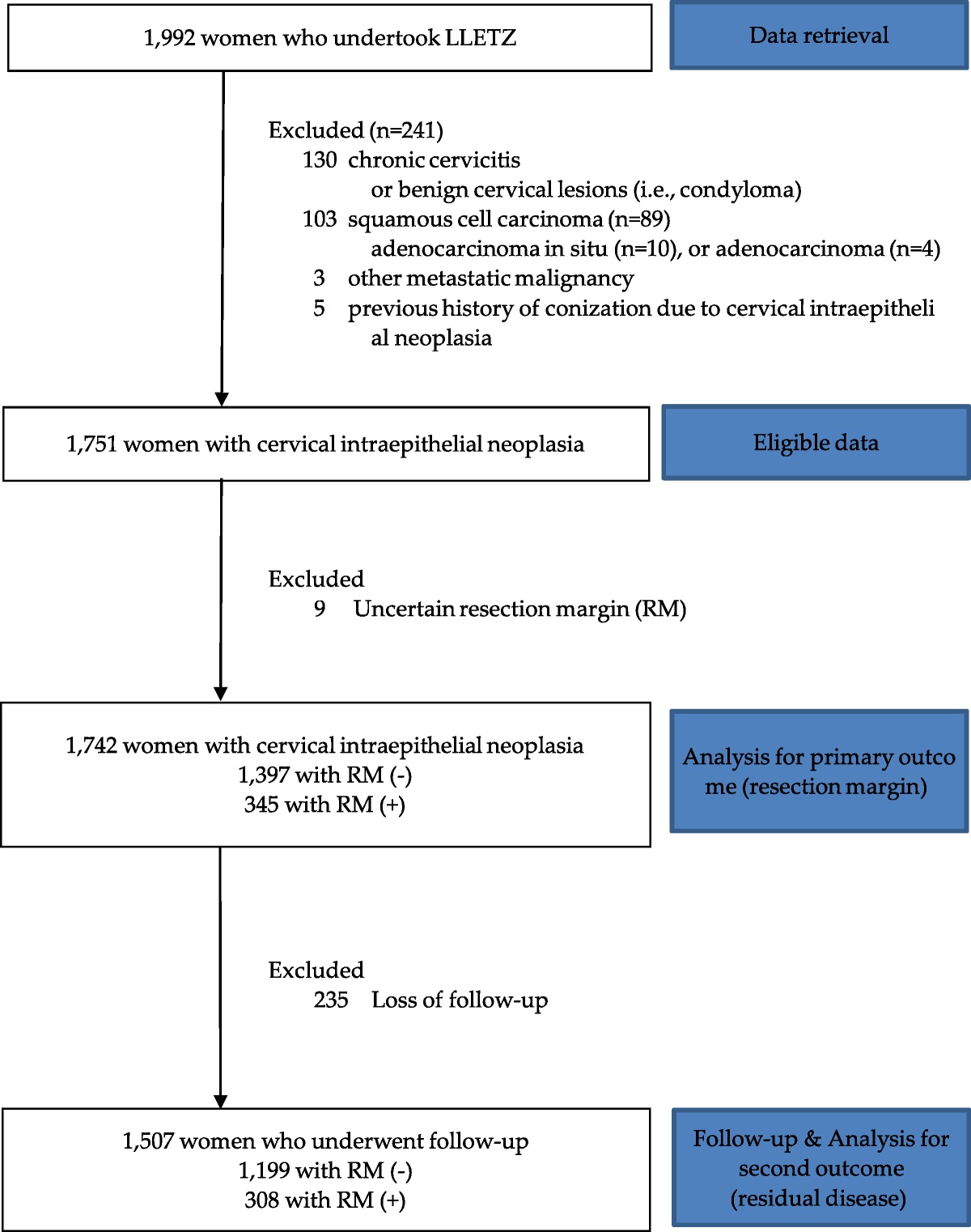
Retrospective register-based study, including women who had an excision of the transformation zone for CIN2 or CIN3 at our institution, between January 2011 and December 2022. The outcome assessed was histopathological recurrence/persistence of CIN2 or worse.
Results
Of the 721 women included, 6.8% (49/721) had recurrence/persistence. The sensitivity, specificity, and positive and negative predictive values of the HPV test were 97.4%, 80%, 22.3%, and 99.8%, respectively, whereas for cotesting (HR-HPV and cytology), 86.8%, 90.1%, 34.4%, and 99.1%, respectively. The referral rates for colposcopy were 24.3% and 14.2%, respectively. The sensitivity of colposcopy was low (40.0%).
Women who were initially positive for non-16/18 genotypes at baseline who became HPV16/18 positive during follow-up, had a statistically significant increased risk of CIN2 or worse, compared with those who tested positive only for other HR-HPV genotypes during both stages (hazard ratio = 4.98; 95% CI = 1.66–14.91).
Conclusions
Human papillomavirus testing is the best strategy for follow-up after treatment of cervical HSIL. The addition of cytology triage decreases by more than 40% the referrals for colposcopy, without significantly missing cases of recurrence/persistence. Human papillomavirus 16/18 in the follow-up, regardless of being previously positive, is associated with higher risk of recurrence/persistence of HSIL.

留言 (0)