According to the 2023 ISPD revised guidelines [5], the initial treatment of catheter-related infections involves adequate antibiotic administration. However, if the infection persists, particularly in cases of refractory ESI or TI, salvage methods such as cuff saving and exit site relocation could be prioritized over the simultaneous removal and reinsertion technique. These approaches preserve the peritoneum, unlike the latter technique which entails peritoneal manipulation.
In cases of intractable infection where both the catheter and cuff are invaded by pathogenic organisms, complete catheter removal is often necessary to ensure eradication, as failure to eliminate the pathogens may result in persistent bacterial colonization. If the infection does not involve the inner cuff, considering partial replantation as a salvage method is feasible [5]. This approach requires several conditions, including a still-functioning inner conduit, a negative culture of dialysate, no signs of infection over the internal cuff area, and specifically, the presence of a near-cuff perforation.
Particularly, eschewing peritoneal manipulation offers numerous benefits. A study in the United States reported that up to 15.5% of PD-naïve patients required a follow-up procedure within 90 days post-initial PD catheter insertion due to complications such as bleeding, catheter obstruction, malposition, kinking, and peritoneal leakage [6]. Notably, the replantation method allows for the prompt resumption of PD without requiring a hemodialysis catheter (0 day vs. 16.6 days, p < 0.001). The use of a hemodialysis catheter, even in short-term, can potentially induce vessel damage, and prolonged dwelling can exacerbate this damage [7,8,9]. Additionally, partial replantation can be executed in an outpatient setting, which obviates the need for hospitalization thus potentially offering greater convenience and cost effectiveness. At our hospital, patients undergoing simultaneous catheter replacement typically required at least three nights and four days of hospitalization to monitor procedure-related complications.
Previous studies have shown that partial replantation is comparable to complete catheter replacement [10,11,12,13]. Our study corroborates earlier research, revealing that partial replantation was not inferior. In contrast to other studies, we opted for a control group comprising patients who had a de novo catheter insertion for initiating PD. Given the lengthy average PD vintage of 66 months in the intervention group, comparing these patients to those newly starting PD could potentially influence the clinical outcomes adversely. Nonetheless, despite this disparity in groups, which includes control patients who had never previously undergone peritoneal manipulation, there was no significant difference in clinical outcomes. This finding emphasizes the non-inferiority of the salvage method compared to de novo catheter insertion. Despite the potential for more complications and reduced durability from retaining the previous catheter below the connector, especially given their average 66-month duration of PD, our study found no inferiority in clinical outcomes. Furthermore, there was no significant difference in the infection rates between the catheter replantation and de novo groups.
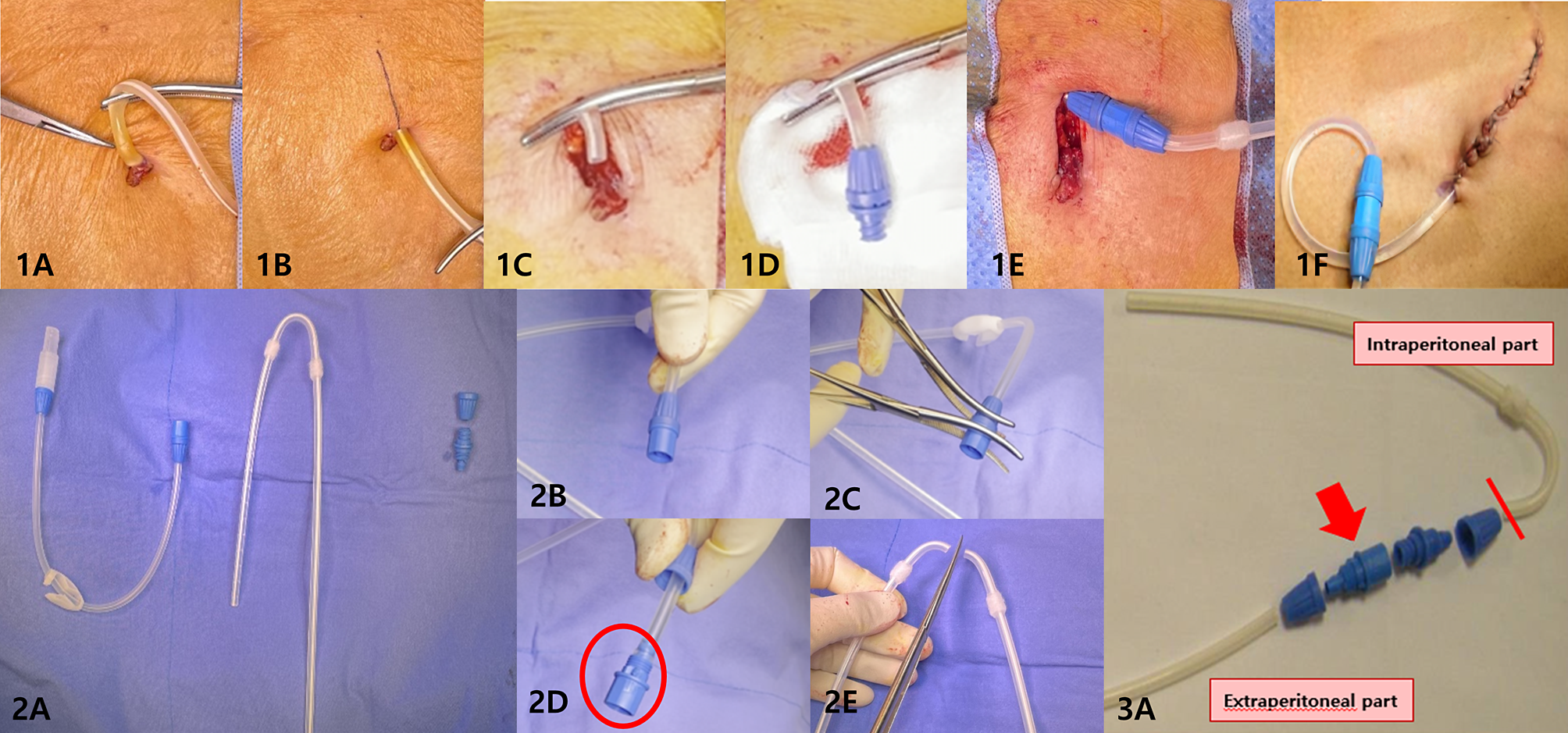
We constructed the connector using two PD adaptors and a segment of a transfer set, which were cost-effective and easily obtainable since they are routinely stocked in the PD unit. Previous studies typically employed medical adhesive glue or a specific endoluminal connector to join the remaining portion of the old catheter with a new one [10, 12,13,14]. The endoluminal tube, either silicone-based or a titanium extender, was integrated into the inner lumen of both catheters, and the interfaces were sealed using type A glue or sutures. However, it is crucial to acknowledge that adhesive materials may trigger chemical reactions with certain types of catheters or surrounding tissues, and the tied method used to connect the catheters can result in dialysate leakage [14, 15]. The biological safety of using adaptors and transfer segments as connectors need further validation. Our long-term follow-up results suggest the relative biocompatibility of the connector device and propose that our approach may offer advantages in terms of reducing complications, enhancing availability, and improving cost-effectiveness.
Our study has some limitations, primarily its small sample size. The reasons for partial replantation were divided into two main categories: refractory catheter-related infection and mechanical catheter damage, encompassing a total of nine patients. Ideally, the clinical outcomes for each group would be compared separately using other techniques, such as simultaneous removal and reinsertion. However, this technique is less commonly performed compared to simultaneous removal and reinsertion and requires specific conditions, which limited the number of eligible cases. Therefore, we chose to combine these two groups into a single cohort for comparison with the de novo insertion group, rather than analyzing infection and mechanical damage cases separately or comparing each subgroup with other methods. Regardless of the reason for performing partial replantation, our findings suggest that its efficacy is comparable to de novo insertion, supporting partial replantation as a viable alternative.
Although the clinical outcomes, specifically infection rates, showed no significant difference between de novo catheter insertion and partial replantation, the proportion of infections appeared relatively high. This may, however, be attributed to our study’s small sample size. Notably, the peritonitis rate at our hospital was 0.242 episodes per patient-year, reflecting effective infection control and education measures. Therefore, the observed higher infection rate is more likely related to the limited sample size rather than an actual deficiency in infection control practices.
In our study, two patients eventually required their PD catheters removed. One patient underwent partial replantation due to catheter perforation, but developed refractory peritonitis with Candida parapsilosis cultured in the peritoneal fluid, leading to the cessation of PD and catheter removal 10 days after the procedure. While it is plausible that the infection was surgery-related, the patient’s history of multiple catheter-related infections and a diabetic foot ulcer suggest that hygiene issues may also have played a role. The other patient underwent partial replantation for refractory ESI with Corynebacterium species, but developed TI with Corynebacterium four months later. Despite two months of antibiotic treatment, the PD catheter was ultimately removed to eradicate the infection. Remarkably, this patient had a history of a fourth ESI and one episode of peritonitis with Corynebacterium species before the replantation. Although there were no signs of peritonitis with an identified pathogen at the time of replantation, colonization by Corynebacteria cannot be excluded.
Despite these limitations, our study provides valuable insights into the management of catheter-related complications using partial replantation. This minimally invasive method may offer a feasible alternative to conventional techniques, potentially reducing hospitalization time and preserving peritoneal integrity. Further large-scale studies are needed to validate these findings and explore the full potential of partial replantation in clinical practice.




留言 (0)