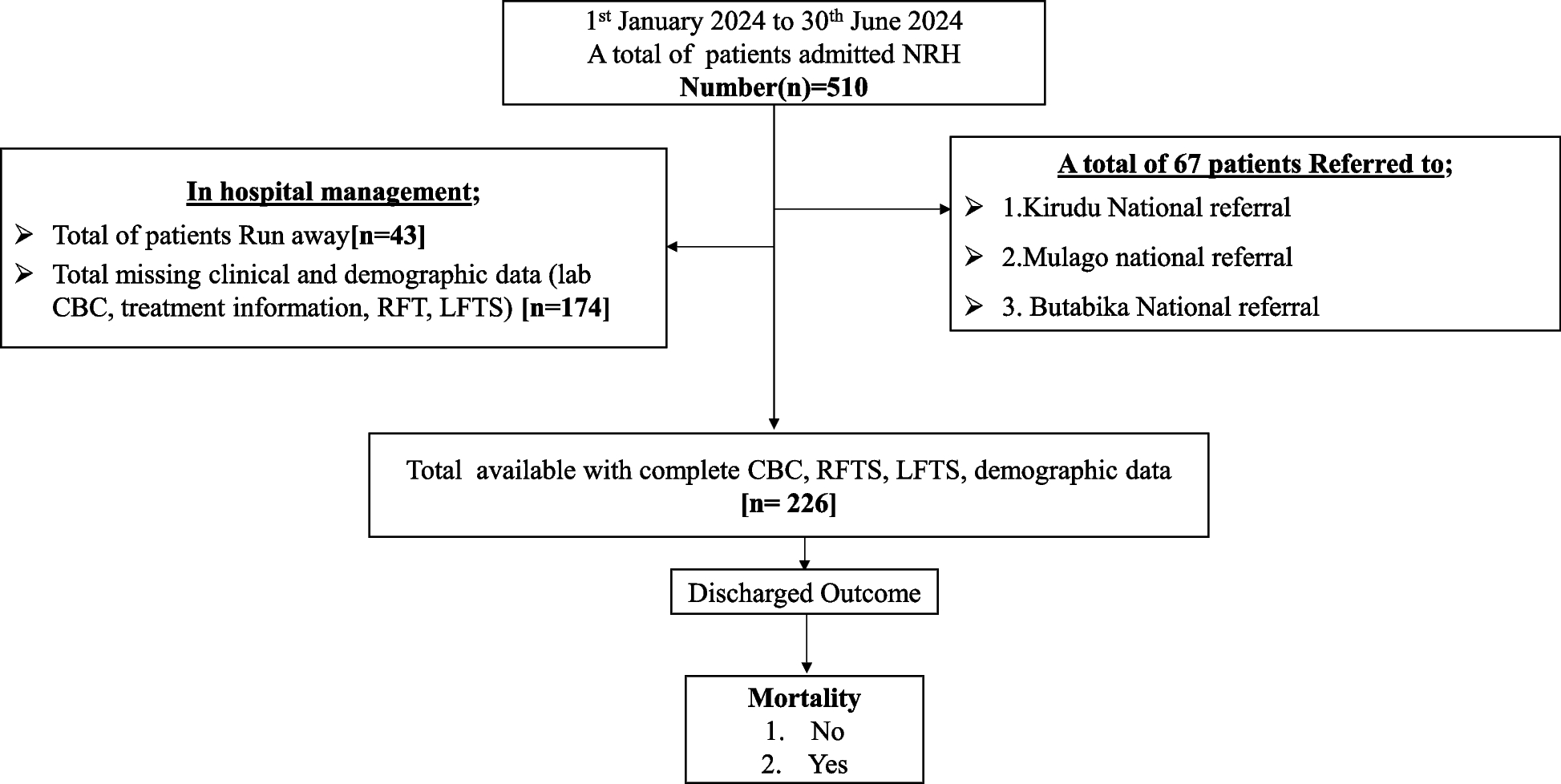
The present study reports several key findings. First, lower eGFR levels were associated with a significantly higher risk of IHM, while higher eGFR levels were linked to a reduced risk. Second, a significant interaction between eGFR and both age and HIV status was observed in relation to IHM in this cohort. Specifically, IHM was notably higher among patients with lower eGFR, particularly in younger patients who were HIV-negative and in HIV-positive individuals aged ≥ 60yrs. Finally, the association remained significant after full adjustment for potential confounders. To our knowledge, this is the first study to examine the relationship between eGFR and IHM in a low-income setting. The study, conducted at NRH, included 226 patients admitted to the internal medicine ward during the first half of 2024 in Uganda.
Patients with lower eGFR levels had a significantly higher risk of IHM, whereas those with higher eGFR levels demonstrated a reduced risk. This finding supports the established association between impaired renal function and adverse outcomes, including mortality [19,20,21]. Low eGFR, which indicates decreased kidney function [22], was associated with physiological disturbances such as fluid overload, electrolyte imbalances [23], and toxin accumulation, all of which may contribute to worse clinical outcomes [24]. IHM was notably higher among patients with lower eGFR who were younger or HIV-positive((≥ 60yrs). The interaction between age and HIV status suggests that young individuals and those with HIV are disproportionately affected by reduced eGFR and comorbidities. This is consistent with literature highlighting the compounding effects of renal dysfunction on morbidity and mortality, particularly in vulnerable populations [19, 22, 25]. A significant negative correlation was observed between low eGFR and specific subgroups. Younger, HIV-negative patients (< 40 years) showed a modest correlation (p = 0.016, r = −0.275), which was stronger in middle-aged HIV-positive patients (40–60yrs; p = 0.020, r = −0.397) and most pronounced in older HIV-positive individuals (≥ 60yrs; p = 0.003, r = −0.997). These results suggest that these subgroups are particularly vulnerable to renal impairment, underscoring the need for targeted monitoring and management.
Previous investigations have largely focused on eGFR’s role in stratifying mortality in populations from Europe, Asia, and the United States [26]. There was a notable lack of data on this association in low-income countries within sub-Saharan Africa, particularly Uganda. Our study addresses this gap by providing data on this association in a low-income, sub-Saharan African context, contributing valuable insights into the unique healthcare challenges faced by these populations. One key finding was the significant inverse correlation between eGFR and IHM, as demonstrated by hazard ratios(HRs) across different eGFR quartiles. Patients in the Q1 group (eGFR < 66.8 mL/min/1.73 m2) had the highest mortality risk, with a hazard ratio of 4.08 (95% CI: 1.284–12.954, p = 0.037), compared to the reference group (eGFR ≥ 120 mL/min/1.73 m2). Similarly, participants in the Q2 group (eGFR = 66.8–99.0 mL/min/1.73 m2) showed a significantly elevated mortality risk (HR = 4.079, 95% CI: 1.284–12.954, p = 0.017). This highlights the graded relationship between declining renal function and mortality, with even moderate reductions in eGFR contributing to a marked increase in risk. Notably, an increase of 48.60 mL/min/1.73 m2 in eGFR was associated with a 54% reduction in IHM risk (HR = 0.46, 95% CI: 0.282–0.759, p = 0.002), highlighting the protective effect of preserved renal function. These results are consistent with previous studies that have established chronic kidney disease(CKD) as a potent independent risk factor for mortality [26,27,28,29]. Possibles explanation was that impaired renal function could possibly lead to the accumulation of uremic toxins, electrolyte imbalances, and volume overload, which contribute to cardiovascular dysfunction and increased risk of adverse outcomes during acute hospitalization [23].
The present study also analyzed the interaction between eGFR and high-risk subgroups, shedding light on how age and HIV status influence the relationship between renal function and IHM. Significant interactions between age and HIV status were observed, aligning with previous findings [30,31,32]. Notably, participants under 60yrs old had a higher risk of mortality compared to older participants (P for interaction = 0.046), potentially due to aggressive or rapidly progressing conditions, such as severe infections or advanced HIV [30, 33]. HIV status emerged as a key predictor of mortality, with HIV-positive individuals aged 40-60yrs and ≥ 60yrs demonstrating significantly higher mortality compared to their HIV-negative counterparts (P for interaction = 0.021). The CKD progression in HIV-positive individuals has been linked to the virus's nephrotoxic effects, opportunistic infections, and antiretroviral therapy-related nephropathy [34]. Compounded risks like chronic inflammation, immune dysfunction, and cardiovascular comorbidities further contribute to poor outcomes in hospitalized HIV-positive patients [6, 34].
Interestingly, among patients (< 40yrs), HIV-positive status was not significantly associated with IHM. Instead, it was associated with HIV-negative status, and a possible explanation for worsened kidney function in this group, possibly due to lifestyle factors such as alcohol abuse and drug use. This pattern suggests that the impact of HIV on IHM may be mediated through different mechanisms depending on age [30, 34].
These findings highlight the critical need for early risk stratification and proactive management of eGFR levels, particularly in resource-limited settings in sub-Saharan Africa particularly Uganda where optimal care is often challenging. Clinicians should prioritize targeted strategies for high-risk groups, including younger patients and individuals with HIV, to enhance outcomes. Recommendations include regular eGFR monitoring, early intervention for declining levels, and tailored management plans addressing both age and HIV status. Emphasizing preventive care and timely treatment adjustments is essential for improved prognosis [6, 28].
Study limitations
Despite the significant findings, this study has several limitations that must be acknowledged. The retrospective cohort design inherently carries the risk of selection bias, which could affect the internal validity of the findings and limit their applicability to broader populations beyond the specific cohort studied. Furthermore, the small sample size and the short study period reduce the statistical power and may limit the ability to detect subtle or long-term effects, potentially skewing the results. Another significant limitation is that this was a single-center study, which restricts the diversity of the sample and raises concerns about external validity. Multi-center studies with larger and more heterogeneous populations, as well as extended follow-up periods, are necessary to confirm and generalize these findings. Additionally, while eGFR is a widely used and accepted surrogate marker for renal function, it may not comprehensively reflect kidney health in certain patient groups. For instance, in patients experiencing acute kidney injury or fluctuating renal function, eGFR may fail to capture dynamic changes or nuanced aspects of renal impairment. Lastly, potential confounding variables and unmeasured factors, such as some comorbid conditions, medication use, or lifestyle factors, were not fully accounted for, which could further influence the study outcomes. Addressing these limitations in future research is essential to validate and strengthen the findings.




留言 (0)