
記住我



This study screened patients with MN who were hospitalized and received RTX treatment at the First Medical Center of the PLA General Hospital from January 1, 2019, to December 30, 2022. Patients with a follow-up period of no less than 12 months were selected. After 7 patients with incomplete data and 3 patients with comorbid tumors were excluded, a total of 126 eligible patients with MN were ultimately included in the study. The follow-up time for these patients was 13.0 (12.0, 20.0) months, and the remission rate reached 73% (n = 126). The details of patient enrollment are shown in Table 1.
Table 1 Comparison of baseline parameters, comorbidities, treatments, adverse reactions, clinical characteristics at admission, and differences between patients who achieved remission and those who did not, in the final study populationThe average age of the study population was 49.0 ± 13.4 years, with male patients accounting for 77.8% of the sample. The mean BMI was 26.7 ± 4.0. Among these patients, 80 (63.5%) had comorbid hypertension, 39 (31%) had diabetes, 7 (5.6%) had coronary heart disease, and 52 (41.3%) were diagnosed with refractory nephrotic syndrome.
Fifty-two (34.9%) patients chose RTX as their initial treatment during the course of the disease, and 75 (59.5%) RTX-treated patients were also treated with GCs and/or IMS. Among them, 19 (15.1%) patients were given tacrolimus, 50 (39.7%) patients were given GCs, and 11 (8.8%) patients were given CsA. Additionally, 50 (39.7%) patients were treated with the standard RTX regimen. The time from the diagnosis of kidney disease to the initiation of RTX treatment was 13.0 (6.0–37.3) months. The standard RTX dose is 2.0 (2.0, 2.0) g, whereas the non-standard RTX treatment dose is 1.1 (1.0, 1.1) g, with the non-standard group primarily receiving low-dose treatment.
Twenty-two (17.5%) patients experienced adverse reactions during the follow-up period. The main adverse reaction was pulmonary infection in 13 patients (10.3%), followed by upper respiratory infection in 5 patients (4.0%), gastrointestinal infection in 2 patients (1.6%), urinary and reproductive tract infection in 1 patient (0.8%), and other reactions in 1 patient (0.8%).
The main clinical characteristics of the remaining laboratory tests, renal pathology, and other baselines are shown in Table 1.
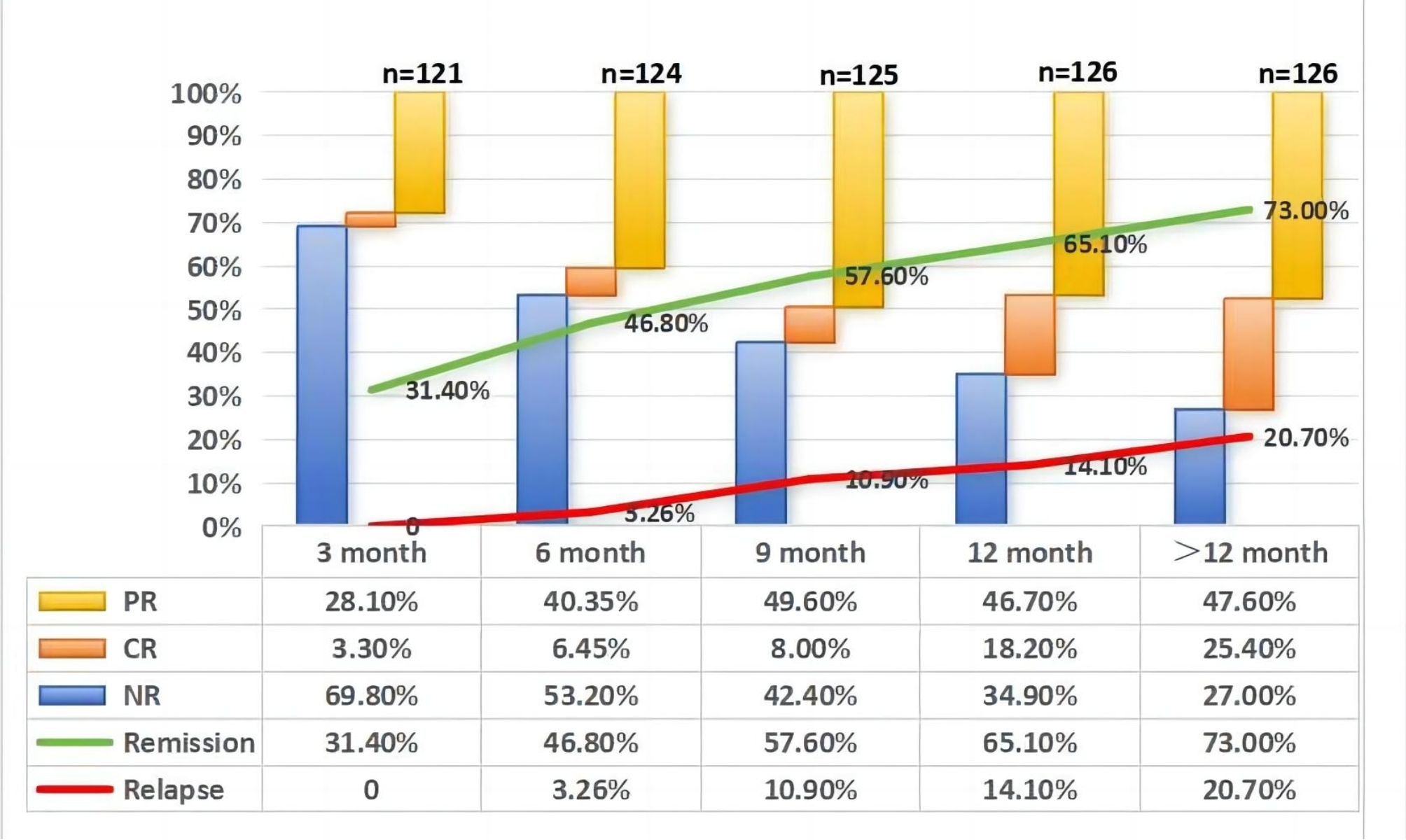
Patient remission and relapse at different follow-up pointsFigure 1 shows that during the 13.0 (12.0, 20.0) months of follow-up in this study, the cumulative remission rate was 73%, and the cumulative relapse rate was 20.7%. Detailed information about patient remission and relapse at different follow-up time points is also presented.
Fig. 1
Patient remission and relapse at different follow-up points
Abbreviations: PR, partial remission; CR, complete remission; NR, non-remission
Third Month Follow-Up: PR was observed in 34 patients (28.1%, n = 121). CR was achieved in 4 patients (3.3%, n = 121). Sixth Month Follow-Up: The number of patients with a PR increased to 50 (40.3%, n = 124). CR was achieved in 8 patients (6.45%, n = 124). Relapse was observed in 3 patients (3.2%, n = 92). Ninth Month Follow-Up: PR continued to increase in 62 patients (49.6%, n = 125). CR increased in 10 patients (8.00%, n = 125). The number of patients who experienced relapse increased to 10 (10.9%, n = 92). Twelfth Month Follow-Up: Fifty-nine patients (46.7%, n = 126) achieved a PR. Twenty-three patients (18.2%, n = 126) achieved CR. The cumulative remission rate was 65.1%. The number of patients who experienced relapse increased to 12 (13, n = 92). Follow-Up Period Over 12 Months: The number of patients with a PR further increased to 60 (47.6; n = 126). CR was achieved in 32 patients (25.4%, n = 126). The number of patients who experienced relapse also increased to 19 (20.7, n = 92).
The impact of different treatment regimens on patient remission and remission speedAmong the different treatment regimens, there was no significant difference in remission rates between the combined GCs and/or IMS therapy group and the RTX monotherapy group (P = 0.439). However, the median remission time in the combined therapy group was 3 (3, 9) months, which was faster than that in the RTX monotherapy group, with a median remission time of 6 (3, 12) months (P = 0.010). Figure 2 shows the differences in remission and relapse rates between the different treatment groups, whereas Fig. 3 shows the differences in the speed of remission between the various treatment groups.
Fig. 2
The impact of different treatment regimens on patient remission and relapse
Abbreviations: Blue P represents the remission difference between different treatment groups
P [1]: After correcting for hypertension, the differences between patient groups treated with or without a combination of GCs and/or IMS were compared; P [2]: After correcting for hemoglobin, CD20, UN, and PLA2R; time to use; glomerular arteriosclerosis; standard treatment; and RNS; the differences between the initial treatment and non-initial treatment patient groups were compared; P [3]: After correcting for RNS; time to use; and initial treatment. compared the differences between the standard treatment and non-standard treatment patient groups
Yellow P represents the difference in relapse between the different treatment groups
Pa: After hypertension was corrected, the differences between patient groups treated with or without a combination of GCs and/or the IMS were compared. Pb: After the hemoglobin, UN, PLA2R, time to use, standard treatment, and RNS were corrected, the differences between the initial treatment and non-initia treatment patient groups were compared. Pc: After UN, RNS, the time to use, and initial treatment were corrected. compared the differences between the standard treatment and non-standard treatment patient groups
GCs, glucocorticoid; IMS, immunosuppressant; UN, urea nitrogen; PLA2R, phospholipase A2 receptor; RNS, refractory nephrotic syndrome
Fig. 3
The impact of different treatment regimens on patient remission speed
Abbreviations: P [1]: After hypertension was corrected, the differences between patient groups treated with or without a combination of GCs and/or the IMS were compared
P [2]: After the hemoglobin, CD20, UN, and PLA2R levels, time to use, initial dose, degree of glomerular arteriosclerosis, standard treatment, and RNS were corrected, the differences between the initial treatment and non-initial treatment patient groups were compared
P [3]: After correcting for RNS, the time to use is the initial treatment. compared the differences between the standard treatment and non-standard treatment patient groups
GCs, glucocorticoid; IMS, immunosuppressant; UN, urea nitrogen; PLA2R, phospholipase A2 receptor; RNS, refractory nephrotic syndrome
The remission rate in the initial RTX treatment group was 84.1%, which was higher than the 67.1% reported in the non-initiall treatment group. However, after adjusting for confounding factors, there was no significant difference between the two groups (P = 0.835). The median remission time was 3 (2, 9) months, and there was no difference in remission speed compared with non-initial treatment patients after adjusting for confounding factors (P = 0.095).
The remission rate in the standard treatment group was 78%, which was higher than the 69.7% reported in the non-standard treatment group. After adjusting for confounding factors, there was a significant difference in remission rates between the two groups (P < 0.001). This result indicates that the standard treatment group had a significant advantage in terms of the treatment effect. In terms of remission time, there was also a significant difference between the standard treatment group and the non-standard treatment group (P = 0.027).
After adjusting for confounding factors, there were no significant differences in relapse rates across all treatment regimens (all P > 0.05).
Differences in baseline parameters, comorbidities, treatment, adverse reactions, and clinical characteristics at admission between remission patients and non-remission patientsCompared with the non-remission group, our study revealed that the remission group had significantly lower cholesterol (P = 0.027), triglyceride (P = 0.001), and PLA2R values (P = 0.029). Additionally, the proportions of diabetic patients (P = 0.017) and patients with refractory nephrotic syndrome (P = 0.001) were significantly lower in the remission group.
Further analysis revealed that more patients in the remission group chose to use RTX as their initial treatment (P = 0.040). Moreover, during the longer follow-up period (P = 0.011), the remission group experienced significantly fewer adverse reactions (P = 0.028).
Apart from the aforementioned significant differences, no other parameters were notably different between the two groups. For detailed information, please refer to Table 1.
Cox regression analysis of risk factors affecting patient remissionUnivariate Cox regression analysis revealed that a lower BMI, the absence of diabetes, the adoption of standard RTX, the combined use of tacrolimus improved the remission rate. The detailed data are presented in Table 2.
Table 2 Cox regression analysis of risk factors affecting remission of patientsIndicators with P < 0.05 (BMI, diabetes, standard treatment, combined use of tacrolimus) were included in the multivariate Cox regression analysis. The results revealed that the standard RTX (HR = 2.262, 95% CI [1.434 ~ 3.568], P < 0.001) improved the remission rate, whereas comorbidity with diabetes (HR = 0.585, 95% CI [0.362 ~ 0.947], P = 0.029) reduced the remission rate.
Cox regression analysis of risk factors affecting patient relapseUnivariate Cox regression analysis revealed that advanced age, higher white blood cell count, and urea can increase the relapse rate of patients. See Table 3 for details.
Table 3 Cox regression analysis of risk factors affecting relapse of patientsIndicators with P < 0.05 (age, white blood cell count, urea) were included in the multivariate Cox regression analysis. Advanced age (HR = 1.082, 95% CI [1.034 ~ 1.132], P < 0.001) and higher white blood cell count (HR = 1.285, 95% CI [1.104 ~ 1.496], P = 0.001) can lead to a higher relapse rate.
留言 (0)