
記住我


The study included 20 HCPs with different professional backgrounds (physicians, psychologists, [specialist] nursing staff, and pastoral care; see Table 1). Participants’ ages ranged from 28 to 60 years (M = 41.45; SD = 9.7) and their professional experience from 5 months to 20 years. The category system for the initial three questions is available in Supplementary Tables 1 and is described below.
Table 1 Sample characteristics and reported professional experiencesQuestion 1: Experiences with suicidality in cancer patientsIn the questionnaire, six HCPs indicated having no contact with suicidal cancer patients, while ten HCPs attended to one to three, and four HCPs attended to more than three suicidal patients annually (Table 1). Moreover, eleven HCPs had private experiences with suicidality in family or friends (N = 4) or relatives (N = 1). Three each reported their own experiences with suicidality (N = 3) or did not provide more information (N = 3), while nine reported no private experiences with suicidality.
Despite initial claims of limited experience (e.g., due to lacking experience in the field), all HCPs reported direct or indirect experiences with different manifestations of suicidality (e.g., in own patients or colleagues’ patients, reading about it in the documentation, or hearing about a patient’s suicide from the patient’s relatives). These described experiences can be differentiated into four categories: (1) passive death wishes/suicidal thoughts, (2) death and dying, (3) stopping life-sustaining actions/suicidal actions and suicide deaths and (4) positive experiences.
All professional groups reported encounters with (1); e.g., “One in ten patients, maybe even a little more (…) expresses at least passive death wishes.” (EI12_psychologist). While some of the HCPs cited somatic symptoms (e.g., pain) as contributing factors for developing suicidal thoughts, paradoxically, improvements in physical symptoms were mentioned triggering suicidal thoughts as well. The common mention of (2) highlights the difficulty in distinguishing between suicidal crises and conversations around assisted suicide/end-of-life care (e.g., “(…) people who are in a hospice [are] very different [from non-palliative patients and how] (…) they deal with impending death.” (EI20_pastoral care)). One psychologist said: “[The patients] want to live and are afraid of dying” (EI17). However, they also reported that one of their patients first expressed thoughts of weariness of life and two weeks later acute suicide risk had to be reassessed. Psychologists, (specialist) nursing staff and pastoral carers shared experiences with (3) of their own patients (e.g., “From time to time it happens; this year it has already happened once (…). She couldn’t cope psychologically and took her own life.” (EI3_specialist nursing staff)). Stopping life-sustaining actions included food refusal or avoidance of treatment. HCPs in the intensive care unit were most likely to encounter patients who attempted suicide.
Some patients had been referred to psychiatric wards, and their suicide deaths occurred post-discharge from these. But this was not always the case. The impact of these deaths was significant, affecting both patients and staff (e.g., “It made waves when a patient witnessed someone jumping off the roof (…) that’s something you don’t need in a situation that’s already burdensome” (EI13_psychologist)). In addition, twelve of the interviewees reported witnessing or hearing about suicide deaths (in their own ward, other wards, or patients unknown to them). Some of the reports concerned certain patients who died by suicide in the oncological ward. Despite the noted challenges, some psychologists reported (4) discussing suicidality with their patients, describing patients’ relief and improved mood after conversations.
Question 2: Asking about suicidalityTwelve HCPs reported discussing suicidality with patients, and 14 reported asking about it under certain conditions (e.g., patient expression, screening results, or intuition) (Supplementary Table 2). However, most (N = 19) did not routinely explore suicidality, of whom five did not explore suicidality at all. Although the HCPs had a concept of potential protective/risk factors or particularly vulnerable groups (e.g., according to the level of social support, financial resources or gender (with men less likely to disclose suicidality) and age), naming specific criteria was difficult for the HCPs, as well as reporting the questions they used. Standard questions included explicit (“Do you have thoughts/plans of taking your own life?” (EI13_psychologist) or “Are you acutely suicidal? Is there an acute danger?” (EI4_physician)) to non-explicit questions (“What kind of images come to mind when you think of peace?” (EI19_pastoral care)). Suicide exploration was understood as a conversation, using “several phases of exploration” to “get an understand what is behind it [meaning patients’ initial reports]” (EI12_psychologist), reflecting concern for patient dignity and context.
Question 3: Managing suicidalityNineteen HCPs had reliable referrals (colleagues, supervisors, psycho-oncology, psychiatry, pastoral care) for patients expressing suicidality (e.g., “I consult with my psycho-oncological team - that would be my first point of contact, alongside the physicians” (EI13_psychologist), “We have the psycho-oncology [as support for the team]. But pastoral care is also always requested, as we have a 24-hour emergency call service.” (EI19_pastoral care) and “[My contact persons are] my colleagues. We have exchange” (EI16_specialist nursing staff)). A mere 10 HCPS mentioned own strategies, e.g. specific interventions such as a no-suicide contract (N = 4) and withdrawal of lethal medication (N = 2), or more general approaches such as perspective-talking (N = 1), involving persons of trust or the patients’ social network (N = 1), administration of medication (N = 3), regular checking and conversation (N = 6), normalization/psychoeducation (informing patients that experiencing thoughts of weariness of life is not uncommon after receiving a life-altering diagnosis) (N = 2), and resource activation with imagination (N = 1). Reactions to suicide deaths varied widely from team discussions to avoidance of the topic, with a focus on future prevention or guilt over perceived mistakes, including difficult feelings like shock, sadness, surprise, and emotional blunting (“I was a bit shocked, and then thought, should I have seen that somehow? [after learning about a patients’ suicide]” (EI7_nursing staff)).
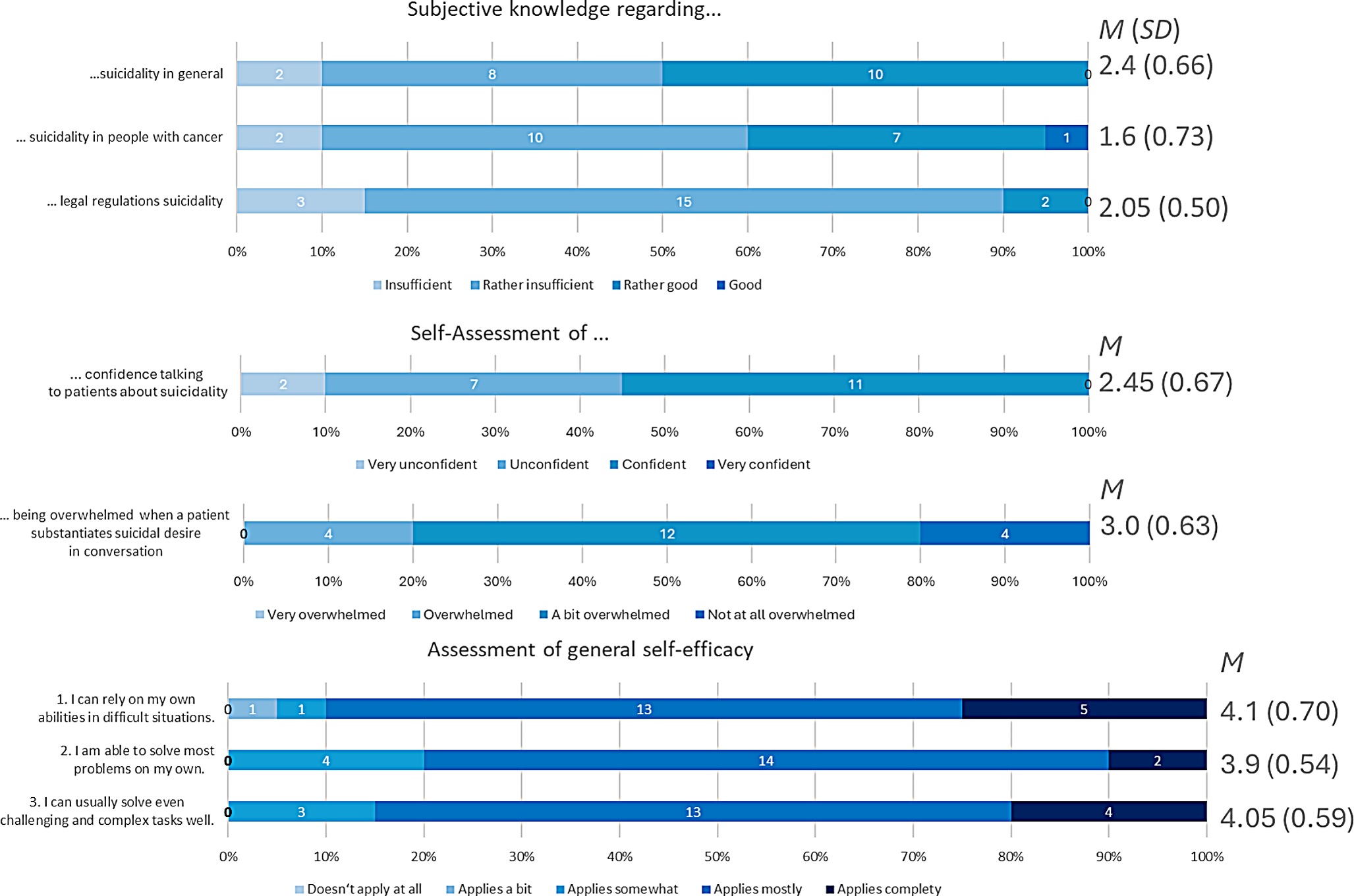
Question 4: Differences in relation to sociodemographicsSubjective knowledge. The interviews revealed the lack of a consistent approach to assessing suicidality. Figure 1 indicates a decline in subjective knowledge the more specifically HCPs were asked about suicidality. For instance, Fig. 2 shows differences across professional groups: psychologists rated their general knowledge the highest, yet it declined with increasing focus on suicidality, while nursing staff perceived themselves the lowest in legal knowledge. A Kruskal-Wallis test revealed no significant differences between professional groups or genders. Age was not associated with knowledge.
Here, the integration of interview and questionnaire data yielded further insights, with one HCP rating their knowledge as “good” within the questionnaire, but casting doubt on the feasibility of assessing suicide risk.
Fig. 1
Piled bar charts of subjective knowledge, confidence, being emotionally overwhelmed and self-efficacy. This figure shows the frequency of each answer of the 20 HCPs as well as mean and standard deviations of responses to each question. The different professional groups rated their subjective knowledge as lower for the more specific kinds of knowledge. Most HCPs rated themselves as “a bit overwhelmed” in encountering suicidal desire. The HCPs rated their self-efficacy as high
Fig. 2
Boxplots of subjective knowledge by professional groups. The boxplots show differences in three levels of subjective knowledge regarding the professional groups. The more specific the questioned topic, the lower the mean value of subjective knowledge
Confidence. Most participants felt “unsure” and “certain” (Fig. 1). The Kruskal-Wallis test showed a difference between professional groups (χ2(4) = 10.09, p =.039), but post-hoc tests found no significant differences. No significant difference was shown in age or gender.
Being emotionally overwhelmed. Most HCPs felt “a little overwhelmed” (Fig. 3). There were no significant differences between professional groups, age or gender.
Self-efficacy. Self-efficacy was rated at M(SD) = 4.02(0.51) (Fig. 1), with physicians scoring the highest. No differences were found between professional groups, age or gender.
Suicide myths. Suicide myths were frequently mentioned in the interviews, either to contradict or reinforce them. High agreement with suicide myths was observed in the questionnaire, especially for the statements “Most patients who die by suicide suffer from depression" (myth 1) and “(…) some kind of psychiatric disease” (myth 2). Many HCPs identified mental disorders such as depression as a key risk factor for suicidality in the interviews. Myth 9 was supported by four HCPs in the interviews. In the case of myth 7, statements from interviews showed that HCPs supported it. At the same time, there were also divergences between the statements made in the interviews and the level of agreement with these myths in the questionnaire (Table 2), for instance, in the sense that one HCP disagreed with the myth (that patients who announce their suicide do not follow through) when it was presented within the questionnaire, but still narrated it in the interview (stating “barking dogs don’t bite”). Endorsing myth 7 correlated negatively with age (r = -.55, p = .013). The agreement to other myths did not differ between age or gender.
Table 2 Suicide myths – comparison of questionnaire responses and interviewFor myth 8, interview responses were mixed, with discrepancies between interviews and questionnaires within HCPs (Table 2). Some HCPs raised knowing about the concern that asking about suicidality might trigger it, but also stated that they disagreed, while others agreed with it. The Kruskal-Wallis test revealed significant differences between professional groups (χ²(4) = 13.66, p =.008), but post-hoc analysis showed no significant differences.
Stigmatization. Stigmatization of suicidality was evident in interviews, with many HCPs avoiding the topic due to preconceived notions, such as patients being too old to be asked about suicidality, the topic not relevant, or suicide exploration is not preventive. The questionnaire showed comparatively higher stigmatization scores in depression/isolation and glorification/normalization subscales (Fig. 3). The Kruskal-Wallis test showed significant differences between professional groups (χ2(4) = 10.12, p =.039), though no post-hoc differences emerged.
Fig. 3
Boxplots of the estimation of people who die by suicide (the German version of the Suicide of Suicide Scale (SOSS-SF-D)). This boxplot shows the results of the German version of the Suicide of Suicide Scale (SOSS-SF-D). It shows higher agreement with the Depression/Isolation scale (M(SD) = 3.43(1.17)) and the Glorification/Normalisation (M(SD) = 3.45(1.13)) scale. There was less agreement with the items of the Stigma Scale (M(SD) = 1.34(0.68)
Relations. There was no significant difference between HCPs who explore and those who do not explore suicidality regarding self-efficacy or stigmatization, but there was a difference regarding the statement that in oncological patients, suicidal thoughts were a means for regaining control (interview: W = 15.5, p =.046 (d = -0.98); questionnaire: W = 14.5, p =.010 (d = 1.44)) and the statement that it was a sign for suicidality if an oncological patient aborts/ceases therapy (questionnaire: W = 17.5, p =.010 (d = -1.48)).
There were differences in confidence (interview: W = 10.5, p =.009 (d = -1.48); questionnaire: W = 18.5, p =.018 (d = -1.13)), being emotionally overwhelmed (interview: W = 13.5, p =.018 (d = -1.43), and subjective knowledge about suicidality (interview: W = 12.5, p =.018 (d = -1.34)) between those exploring and not exploring suicidality; with the former reporting greater confidence, being less emotionally overwhelmed, and knowing more.
In general, confidence (r =.59, p =.006), self-efficacy (r =.53, p =.017), and stigmatization (r =.53, p =.017) were associated with being (less) emotionally overwhelmed.
留言 (0)