Preoperative risk stratification is an essential tool for identifying high-risk patients. A 2020 review found 26 preoperative predictive scores of postoperative mortality, such as the Preoperative Score to Predict Postoperative Mortality, the American Society of Anesthesiologists classification system (ASA), or the Charlson comorbidity index (Charlson et al. 1987; Le Manach et al. 2016; Saklad 1941).
In 2021, the IESG developed a new risk score to predict 90-day mortality after esophagectomy (D’Journo et al. 2021). Before introducing a risk prediction model to clinical use, it should be validated on patient populations. To our knowledge, this is the first study to validate the IESG score in a single-center high-volume center which has not contributed toIESG data.
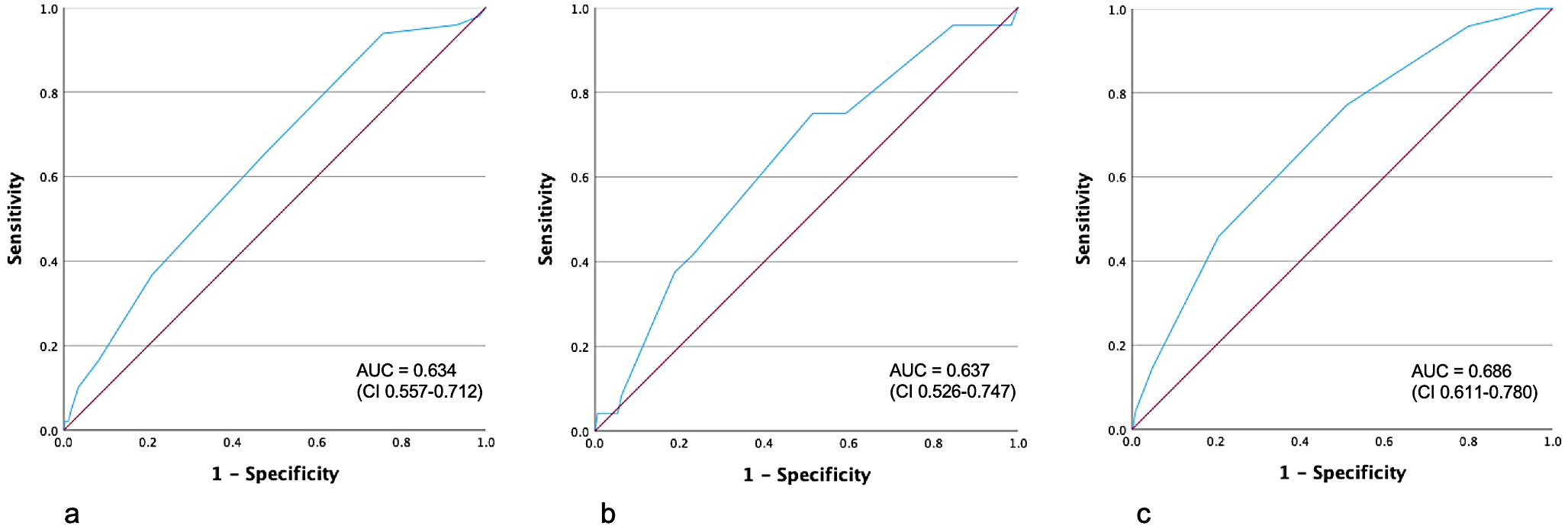
Steyerberg et al. reported in 2006 a predictive score including eight characteristics related to the outcome after esophagectomy (Steyerberg et al. 2006). A key limitation of this score is that it relies on patient data from the 1990s. As morbidity and mortality of esophagectomy have dramatically changed over the past three decades, the prognostic value of the Steyerberg score might be limited. However, the AUC of the Steyerberg score in our cohort was 0.637, confirming the initial study’s results (AUC 0.56–0.70). Compared to the original publication of the Steyerberg score, our 30-day mortality was lower (3.0% compared to 4%,7%,10%, and 11%). The most likely explanation for this difference is the abovementioned improvement in perioperative treatment. Furthermore, Steyerberg’s score is based upon SEERs (Surveillance, Epidemiology, and End Result) data, which included lacks granularity of institutional databases and therefore may have missed some relevant predictive factors including ASA (American Society of Anesthesiologists) classification.
The in-hospital mortality score by Fuchs used six patient factors (age, cardiovascular, pulmonary, renal and hepatic comorbidity and tumor pathology) and two hospital factors (operation volume/year, abdominal approach) to calculate the mortality (Fuchs et al. 2017). The AUC for the Fuchs score was 0.686, which also agrees well with the score. The in-hospital mortality rate in our hospital was 6.7% compared to 7.7%, as calculated by the Fuchs score.
The Fuchs score’s main limitation is the reliance on a nationwide database, including data on discharge records. These databases rely on accurate data but may lack details on complex cases, like preoperative functional or nutritional status or neoadjuvant treatment.
Even though considerable differences between the cohorts of the original publication of the IESG score and our cohort exist, predictive values were similar with 0.634 compated to 0.68 in development and 0.64 in the validation group. Almost 60% of the patients in the IESG cohort had a minimally invasive operation, whereas in our cohort over 20 years starting in 2002, a majority received an open operation (87.4%). In the IESG cohort on the other hand the investigation period was relatively short with just four years. Although the operation technique is not part of the risk stratification for IESG, this finding shows similar performance in different settings. A limitation pertinent to the IESG score is its derivation from the Esodata database, which was not designed for this specific research questions and lacks the capacity for in-depth analysis or the consideration of additional variables.
However, preoperative risk stratification should be practical and reliable. Complex scores with too many parameters are less suitable for clinical use. Parameters that need to be calculated or analyzed may need to be more practical for the clinical routine. The IESG score includes ten parameters compared to eight factors included in the Steyerberg and eight factors in the Fuchs score. Inclusion of more parameters should naturally result in a more sophisticated model yielding a more accurate risk prediction. However, in our collective all scores revealed rather low predictive power irrespective of the number of parameters included. The parameters used in the IESG score all seem reasonable and are simple to collect. Yet inclusion of ten parameters each with various numerical values results in a cumbersome calculation process which seemed slightly too complex for the clinical implementation of this score in the past. Yet, rapid advancements in artificial intelligence (AI) and related technologies have significantly expanded the possibilities for complex risk prediction models. While modern tools could manage a larger number of parameters more efficiently, practical challenges currently faced in routine clinical workflows, such as time constraints, user training, and accessibility in resource-limited settings still have to be considered. Future risk prediction models should aim to leverage the transformative potential of these innovations.
The three models differed in the included comorbidities for calculating the score. Whereas Fuchs and Steyerberg found that cardiovascular, pulmonary, renal, and hepatic comorbidities had an impact, the grade of the impact differed. For example, Steyerberg gave every comorbidity one point, whereas Fuchs’s score shows more severity for renal and especially hepatic comorbidities. The IESG score, on the other hand, just gave a higher score for people with moderate or severe liver disease and did not include pulmonary or renal comorbidities but connective tissue disease and peripheral vascular disease. All investigated scores carry the risk that comorbidities are underestimated and not entirely diagnosed at the time of the risk assessment. Combining all published studies on this topic, a meta-analysis showed that an age ≥ 70 and cardiac and renal comorbidities significantly impacted the 30-day- and in-hospital mortality. In contrast, the meta-analysis did not show a significant impact of a BMI < 18.5 and pulmonary comorbidities on the 30-day- and in-hospital mortality. The alcohol intake that was also a significant prognostic factor for a 30-day- and in-hospital mortality (OR 3.1 (95%CI 2.26–4.25) was not included in any of the three predictive scores (van Kooten et al. 2022).
Another important parameter in all three scores is hospital volume. High-risk procedures such as esophagectomy should be performed in high-volume centers to reduce morbidity and mortality (Markar et al. 2012; Metzger et al. 2004).
Our study has some limitations. It is a retrospective single-center evaluation with a smaller sample size than the original publications (IESG 8403, Fuchs 23751, Steyerberg 3592 patients). Another limitation of this study is the long study period from 2002 till 2021. As noted in the introduction, substantial changes have occurred in surgical techniques, intensive care, and complication management. These advancements have likely contributed to improved outcomes in recent years. The long study period could also explain the higher mortality rates observed in our cohort’s low- and very low-risk groups compared to the IESG cohort. When analyzing only patients treated from 2015 to 2021, the mortality rates decrease to 3.2% for the low-risk group and 1.3% for the very low-risk group, which are consistent with the results reported by the IESG.
Even when postoperative mortality could be reduced over the years, complication rates of up to 22–70% are mainly caused by respiratory complications like pneumonia with respiratory failure, arrhythmia, anastomotic leakage, and wound infection (Atkins et al. 2004; McLoughlin et al. 2013; Raymond et al. 2016). Results of the IESG score showed that this kind of complications occur more often in very high and high-risk patients (D’Journo et al. 2021).
How can we apply high-risk patient identification in practice? First, surgery indications for high-risk patients should be critically reconsidered, especially if definitive radiochemotherapy is a viable alternative. If neoadjuvant radiochemotherapy shows a good response, surgery with its risks might be postponed in favor of regular follow-up in selected cases. However, with an AUC of < 0.7 in all scores, prediction is unreliable and therefore the scores show insufficient performance to guide these important treatment decisions.
Second, procedures such as prophylactic endoluminal vacuum therapy should be considered in patients with increased risk profile. Studies in this regard currently need to be improved. A systematic review of prophylactic vacuum therapy identified four case series for patients undergoing esophagectomy for cancer treatment (Adamenko et al. 2022). The biggest case study with 67 patients, whereas 57 patients were identified as high-risk patients (ASA > 2, BMI > 29, WHO/ECOG score > 1, age > 65 years), was done after minimal invasive Ivor-Lewis procedure. The morbidity rate was 40% for minor and 15% for major morbidity. 73% of the patients showed an uneventful healing of anastomosis. The anastomosis leakage rate was 7.5% (Müller et al. 2021). Thus, prophylactic endoluminal vacuum therapy could reduce the rate of anastomosis leakage and therefore, may also reduce morbidity and mortality rates, but high-evidence is lacking. As it might be a potential option for high-risk patients the potential drawbacks of prophylactic endosponge therapy must be considered. One notable concern is its possible interference with established enhanced recovery after surgery (ERAS) or fast-track programs, which have been consistently shown to improve postoperative outcomes (Huang et al. 2024). This conflict underlines the need for a balanced approach carefully evaluating risks and benefits of prophylactic endosponge therapy. Future research should focus on clarifying its efficacy and determining its role in the context of high-risk patients and ERAS protocols.
Last but not least, high-risk patients should be monitored more intensively after surgery to identify and treat complications early, in order to reduce perioperative morbidity and mortality by their timely treatment.
In conclusion, the existing scoring systems provide a possibility for individual preoperative risk stratification, especially to identify high-risk patients. However, strategies for identifying these patients and their application in everyday clinical life currently need to be improved due to their low predictive ability.



留言 (0)