Study population
The study was based on data from a postal follow-up survey (Augsburger Herzinfarkt-Versorgungsstudie 2023) conducted in participants of the Myocardial Infarction Registry Augsburg. This population-based registry was established in 1984 as part of the MONICA project (Monitoring Trends and Determinants in Cardiovascular Disease) as the KORA (Cooperative Health Research in the Region Augsburg) Myocardial Infarction Registry. Since 2021, it runs as Myocardial Infarction Registry Augsburg. It includes patients who have had a clinically confirmed, hospitalized AMI or who had died prehospitally due to ischemic heart disease [7]. The registry covers the city of Augsburg, Germany, and the two adjacent counties of Augsburg and Aichach-Friedberg, with a total population of approximately 680,000.
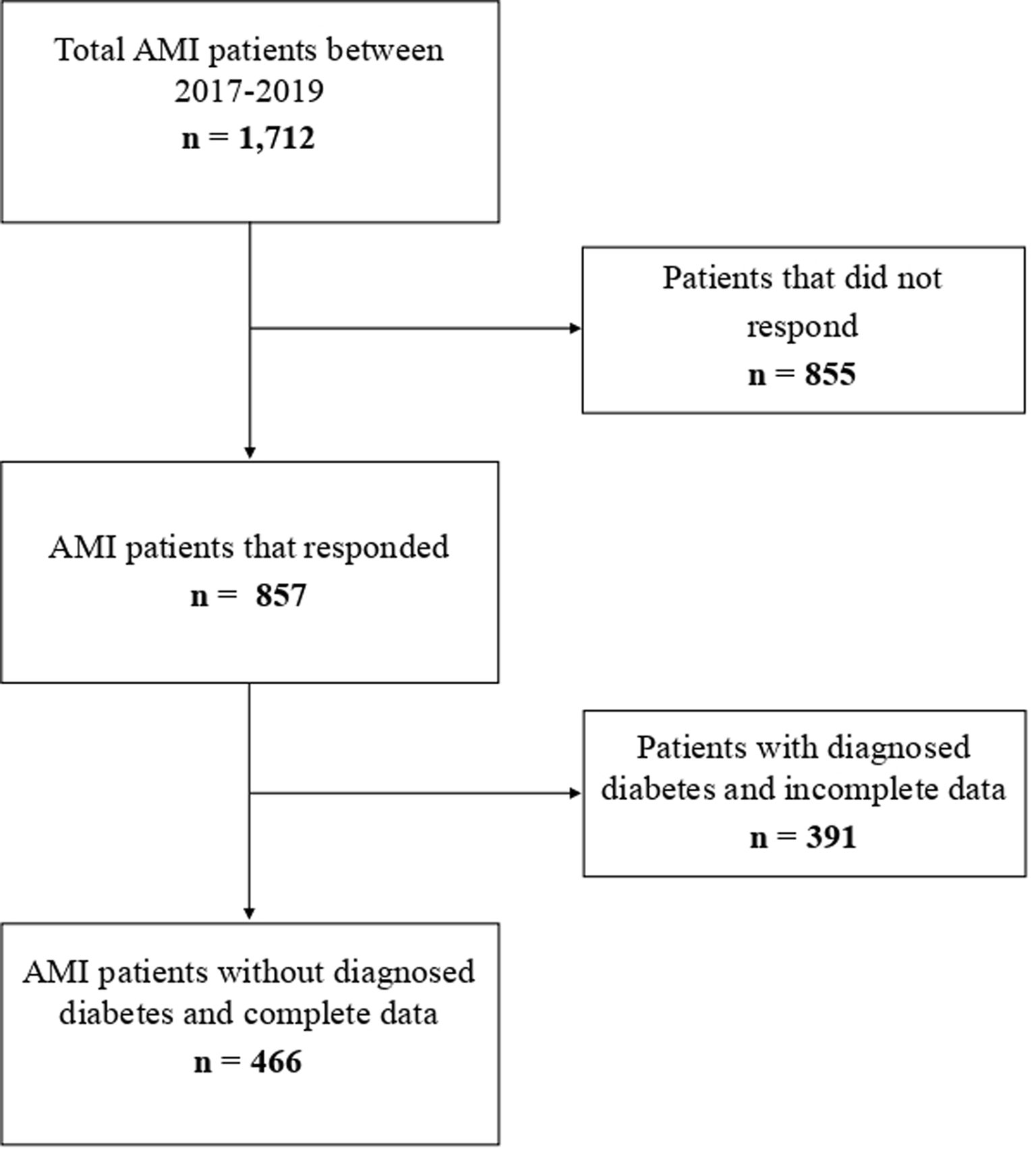
In April 2023, all survivors of acute or recurrent myocardial infarction admitted to a hospital between 2017 and 2019 (n = 1,712) were contacted via a postal questionnaire. A total of 857 patients (50.1%) returned the completed questionnaire. Among the non-responders, 67 patients had passed away, 104 had relocated to an unknown address, and 42 were unwilling or unable to participate. The remaining individuals (n = 642) received a reminder by mail but did not respond.
For statistical analysis, the study excluded patients previously diagnosed with diabetes. Additionally, patients lacking complete information on FINDRISC criteria (see 2.2) or self-perceived diabetes risk were omitted from the analysis.
All participants provided written informed consent. The data collection methods received approval from the the ethics committee at the Bavarian Medical Association (Bayerische Landesärztekammer), and the study adhered to the ethical guidelines of the Declaration of Helsinki. The study was registered at the German Register of Clinical Studies (DRKS, project number DRKS00029042).
Variables of interest
The Augsburger Herzinfarkt-Versorgungsstudie 2023 utilized a questionnaire to assess self-reported information about demographics, health status, history of diabetes, health-related quality of life, symptoms of depression, fatigue, and mental health literacy. This data was linked with existing medical chart data provided by the Myocardial Infarction Registry to enhance the dataset with further socio-economic and clinical data.
Fourty questions were applicable to all participants, while an additional seven targeted those with diagnosed diabetes. For the present analysis, 11 specific questions were selected that included assessments of age, weight, height, waist circumference (female: <80 cm, 80–88 cm,>88 cm; male: <94, 94–102 cm, > 102 cm), physical activity, healthy eating habits, use of antihypertensive medication, previous hyperglycemia, and first or second degree family history of diabetes (first degree: immediate relatives like parents or siblings; second degree: distant relatives like grandparents or aunts/uncles).
Responses to these questions were scored according to the scheme established by Lindström et al. [5], and the FINDRISC score was calculated as the sum of these subscores. The score was used to categorize patients into five risk levels for developing diabetes within the next decade: ≤6 points (very low), 7–11 points (low), 12–14 points (moderate), 15–20 points (high), and > 20 points (very high). According to Lindström et al., the corresponding estimated risk of diabetes in the next 10 years is 1%, 4%, 17%, 33%, and 50%, respectively [5, 8]. Participants were also asked to self-report their perceived risk of developing diabetes if they had not been diagnosed, with response options matching the five FINDRISC categories.
Additional questionnaire items were selected that assessed marital status, education level and mental health. For multivariable analysis, marital status was simplified by combining ‘divorced’ and ‘widowed’ participants with ‘singles’, resulting in two categories: ‘single’ and ‘married’. Education was categorized into several levels (dropped out of school, 9 years, 10 years, 12 years, university degree) and dichotomized into ‘low’ and ‘high’ education categories, using 12 years of schooling as the threshold for higher education for clearer statistical interpretation.
The PHQ-9 (Patient Health Questionnaire-9) score, a screening tool for depressive symptoms based on the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders) system, was also assessed. It included nine items that evaluate the frequency of depressive symptoms experienced over the past two weeks. The total score was categorized into four levels of depression severity (mild, moderate, moderately severe, severe) as defined by Kroenke et al. [9]. For multivariable logistic regression analysis, this score was treated as a continuous variable to provide a nuanced interpretation of mental health’s impact on self-perceived diabetes risk.
Data from participants who completed the questionnaire were integrated with medical chart data to encompass information on smoking history and the clinical course of AMI. The expanded dataset included variables such as previous AMI, type of infarction (ST Elevation Myocardial Infarction, Non-ST Elevation Myocardial Infarction), and therapeutic procedures such as percutaneous transluminal coronary angioplasty (PTCA) and aorto-coronary bypass surgeries. Furthermore, the dataset included the time interval between the occurrence of AMI and the completion of the survey.
Statistical analysis
The primary outcome of this study was the misperception of drug-treated diabetes risk in AMI patients, defined by the difference between self-assessed diabetes risk and the FINDRISC score. This difference categorized patients into three groups: those who overestimated (positive difference), underestimated (negative difference), or accurately assessed (zero difference) their risk. For statistical analysis, participants who overestimated or accurately assessed their risk were combined into the single group “Overestimation”, based on findings that overestimation is less harmful than underestimation in terms of preventive behaviors [10]. Thus, the comparative analysis focused on the differences between participants who underestimated and those who did not underestimate their risk.
Baseline characteristics were presented as absolute frequencies and percentages for categorical variables and differences in them between the groups were evaluated using chi-squared tests. For continuous variables, differences were assessed using Student’s t-test or the Mann-Whitney U test (non-normally distributed variables), with results presented as means with standard deviations (SD) and medians with interquartile ranges (IQR).
Multivariable logistic regression models were calculated to identify variables significantly associated with the underestimation of drug-treated diabetes risk. Prior to conducting the logistic regression analysis, the model’s assumptions were validated to ensure the reliability and validity of the results (tests for multicollinearity and log-linearity of continuous variables).
The initial logistic regression model included a comprehensive set of variables, including age, sex, BMI, waist circumference, marital status, education level, diet, physical activity, smoking, first and second degree family history of diabetes and second degree family history of diabetes, previous diagnosed elevated blood glucose levels (dichotomous), antihypertensive drug use, PHQ9 score (categorical), previous AMI, type of infarction, PTCA, aorto-coronary bypass and time span from AMI. A backward elimination process was employed manually, whereby the least significant predictor was removed at each step. This process was continued until only statistically significant predictors remained in the parsimonious model. The results are presented as odds ratios (OR) with 95% confidence intervals (CI) and p values.
To further validate the logistic regression model, a supplementary linear regression analysis was conducted and is detailed in Supplementary Material Table S1. This analysis aimed to confirm the difference between perceived and calculated FINDRISC diabetes risk scores (outcome) by assessing how demographic, clinical, and behavioral factors in the linear regression model contribute to any discrepancies in risk perception.
The analysis was restricted to complete case data. A p-value of less than 0.05 was considered indicative of statistical significance. All statistical analyses were performed using R Studio (Version 2023.12.1 + 402) with the following packages: broom, car, dplyr, ggplot2, glm2, haven and readr.









留言 (0)