
記住我








Between 2006 and 2010, the UK Biobank study recruited more than 500,000 adults aged 37–73 years from the community population, which was one of the large-scaled epidemiological cohort studies worldwide [27]. At the baseline visit, participants completed a touch-screen questionnaire, a face-to-face interview, and anthropometric measurements in one of 22 assessment centers across England, Scotland, and Wales. Extensive information was collected on early-life experiences, demographic characteristics, lifestyle factors, and physical and mental health status, along with the biological sample collection. The North West Multi-Centre Research Ethics Committee (reference: 21/NW/0157) approved the ethical of UK Biobank study, and all participants wrote the informed consent before the baseline assessment.
Definitions of MASLD populationAccording to the international expert consensus [3], MASLD was defined as the hepatic steatosis in combination with at least one following metabolic dysfunction: excess adiposity (WC ≥ 88 cm for females or ≥ 102 cm for males, or BMI ≥ 25 kg/m2), prediabetes (glycated haemoglobin [HbA1c] ≥ 39 mmol/L) or type 2 diabetes, hypertension (systolic/diastolic blood pressure ≥ 130/85 mmHg, or using antihypertensive drugs), hypertriglyceridemia (triglycerides [TG] ≥ 1.70 mmol/L, or using lipid-lowering drugs), and decreased high-density lipoprotein cholesterol (HDL-C) (HDL-C ≤ 1.0 mmol/L, or using lipid-lowering drugs). Due to the absence of ultrasonographic assessments of hepatic steatosis in the UK Biobank, fatty liver index (FLI) was calculated to determinate hepatic steatosis [28], which has been validated in evaluating the hepatic steatosis in previous studies [29]. The calculation of FLI incorporated BMI, WC, serum TG, and serum γ-glutamyltransferase and the equation was as following: FLI = \(\:\frac^\text\text\left(\text\text\right)+0.139\text\text\text\text+0.718\text\text\text\left(\text\text\text\right)+0.053\text\text\text-15.745}\right)}}^\text\text\left(\text\text\right)+0.139\text\text\text\text+0.718\text\text\text\left(\text\text\text\right)+0.053\text\text\text-15.745}\right)}*100\). According to previous study [28], an FLI ≥ 60 was unitized to diagnose hepatic steatosis, representing a sensitivity of 87% and specificity of 86%.
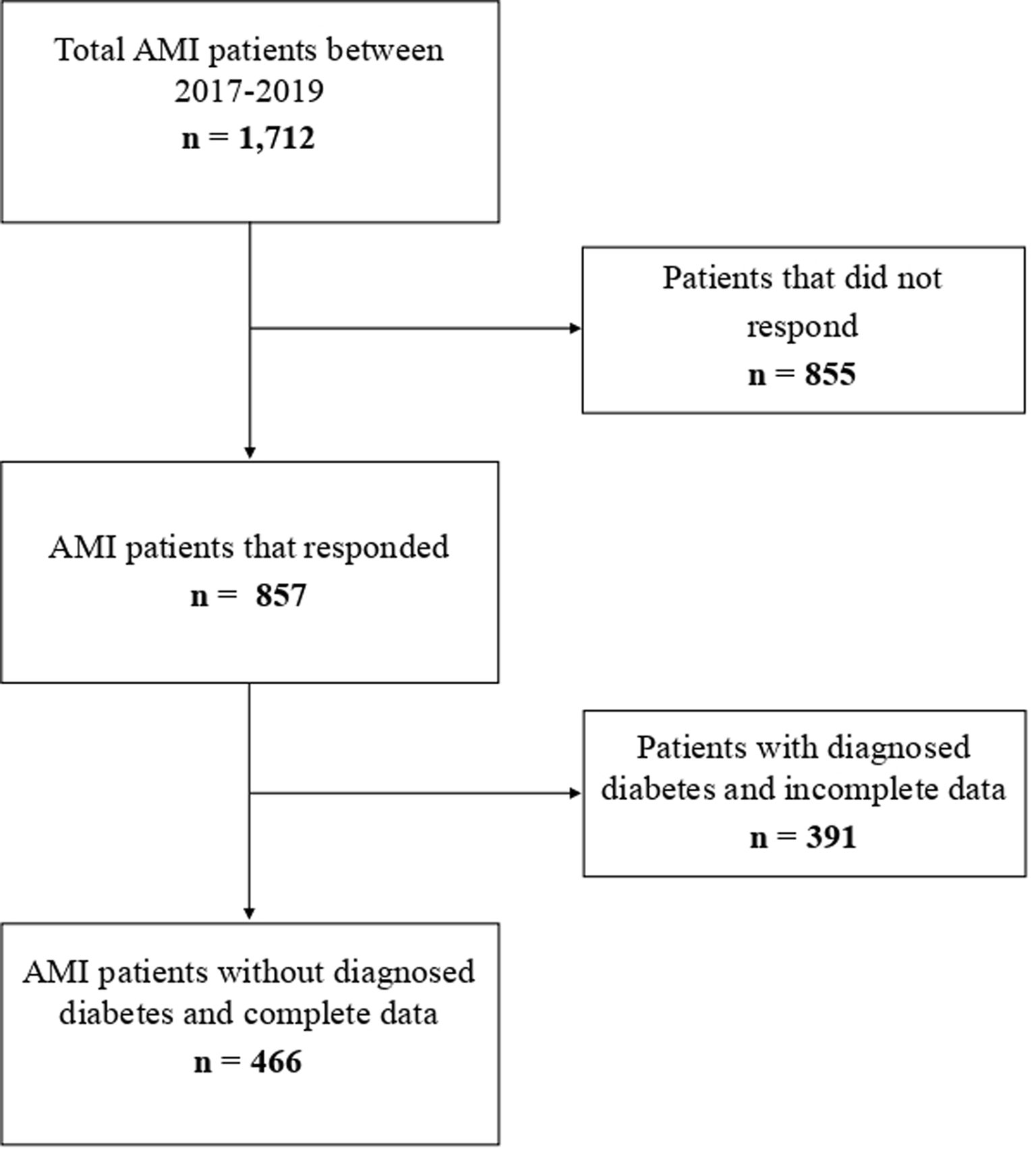
Selection of study populationOf 502,366 participants in the UK Biobank study, we firstly excluded those without complete data on components of MASLD or TyG-related indices (n = 97,465), leaving a total of 404,901 participants. In addition, we further excluded those with a diagnosis of CVD at or before the baseline assessment (n = 30,775), those with missing data on covariates (n = 98,425), and those free of MASLD at baseline (n = 178,370). Finally, a total of 97,331 participants with MASLD and free of CVD were included in current study. Figure 1 illustrated the detailed procedure of selecting study population.
Fig. 1
Flowchart of participants selection
Assessment of TyG-related indicesA random peripheral venous blood sample was taken from each participant at the baseline assessment, and biochemical measurements, including glucose, TG, total cholesterol, HDL-C, low-density lipoprotein cholesterol, C-reactive protein, uric acid, and creatinine, were performed on a Beckman Coulter AU5800 chemistry analyzer. Detailed methods and quality control are available on the UK Biobank website (https://biobank.ndph.ox.ac.uk/showcase/refer.cgi?id=1227). Besides, three indictors of BMI, WC, and WHtR were selected to measure general or central obesity in participants with MASLD. Thus, the final analyses included four TyG-related indices, namely TyG, TyG-BMI, TyG-WC, and TyG-WHtR [30]. The following equations were used to calculate four above indices:
(1)TyG = Ln[TG (mg/dL)*glucose (mg/dL)/2]
(2)TyG-BMI = Ln[TG (mg/dL)*glucose (mg/dL)/2]*[weight (kg) / height2 (m2)]
(3)TyG-WC = Ln[TG (mg/dL)*glucose (mg/dL)/2]*WC (cm).
(4)TyG-WHtR = Ln[TG (mg/dL)*glucose (mg/dL)/2]*[WC(cm)/height(cm)]
Assessment of outcomesThe primary outcome in present study was the incidence of overall CVD (including CHD and stroke) in individuals with MASLD. The secondary outcome was all-cause and cardiovascular mortality. Participants were followed from the date of competing baseline assessment to the date of incident first CHD or stroke, or death, or November 30, 2022, whichever came first. The date of new-onset incident cases was identified through linkage with hospital inpatient data and death register records. The occurrence of overall CVD and cardiovascular mortality was defined by the 10th revision of International Classification of Diseases (ICD-10) codes, including I20-I25 for CHD and I60-I64 for stroke.
CovariatesAccording to previous related studies, we also collected several potential covariates at the baseline visit. These factors included baseline age (years, continue variable), sex (female and male), ethnicity (white and nonwhite ethnicity), Townsend deprivation index (TDI) (continue variable, with a higher score indicating more deprived), education (college degree and above and others), employed status (employed and not), family income (less than £18,000, £18,000 to £51,999, and equal to or greater than £52,000), smoking (never, ever, and current smoking), physical activity (total amount of moderate-intensity activity ≥ 75 min/week or vigorous-intensity activity ≥ 150 min/week or equal combination and not), frequency of alcohol drinking (never drinking or special occasions, one to three times a month, once or twice a week, once or twice a week, three or four times a week, and daily or almost daily), total sleep duration (< 7 h/day, 7–8 h/day, and > 8 h/day), healthy diet score (continue variable, a higher score indicating healthier diet, comprising of seven diet components) [31], family history of cardiometabolic diseases (yes and not, including hypertension, diabetes, and CVD).
Statistical analysisBaseline characteristics of study population were summarized according the occurrence of new-onset overall CVD. Kolmogorov-Smirnov test was used to examine the normality of continue variables. Non-normally distributed continue variables were summarized as median (interquartile range, IQR), while normally distributed variables as mean (standard deviation, SD). Categorical variables were expressed as number (%). Then, Student’s t tests (for continue variables with normal distribution) or Kruskal-Wallis ranks-sum tests (for continue variables with non-normal distribution) or Pearson Chi-square tests (for categorical variables) were performed to compare the between-group differences in baseline characteristics. In addition, we divided participants into four groups according to the quartiles of TyG index and compared the baseline characteristics in each group with the same statistical methods as above.
Kaplan-Meier curves stratified by the quartiles of TyG index with log-rank tests were applied to compare the cumulative hazard of each study outcome. Cox proportional hazards models were used to estimate the hazard ratios (HRs) and 95% confidence intervals (95% CIs) for the associations of TyG-related indices with CVD and mortality in participants with MASLD. Multivariate-adjusted HRs were estimated for higher quartiles of each TyG-related index versus the lowest quartiles and for each 1-standard deviation (SD) increment in TyG-related indices. Additionally, restrict cubic spline (RCS) based on the Cox proportional hazards models were applied to flexibly evaluate the shape of associations between TyG-related indices and all study outcomes with four knots (at the 5th, 35th, 65th, and 95th percentiles). If there existed nonlinear relationship, the threshold values were estimated by trying all possible values and chose with the highest likelihood. We further fitted the two-segmented Cox proportional hazard models on both sides of the threshold point to assess the associations between TyG-related indices and outcomes. All above models were adjusted for age, sex, ethnicity, education, TDI value, family incomes, employed status, smoking, drinking, physical activity, sleep duration, diet, and family of cardiometabolic diseases.
Additionally, we calculated Harrell’s C index, net reclassification index (NRI), and integrated discrimination improvement index (IDI) to assess the incremental performance of TyG-related indices over conventional risk factors for CVD and mortality in MASLD patients [32]. C index is a discrimination index, while IDI and NRI assess whether the new model provides improved risk stratification compared to the basic model. A basic model was developed using variables from the Framingham Cardiovascular Risk Score [33], including age, sex, smoking status, BMI, SBP, anti-hypertensive medication, diabetes, total cholesterol, and HDL-C. We then compared the predictive value of the basic model with that obtained by incorporating TyG-related indices.
Several additional analyses were performed to confirm the robustness of our results. Firstly, to minimize the potential reverse causality, landmark sensitivity analyses were conducted by excluding MASLD patients who occurred corresponding study outcome within the first 2 years of follow-up. Secondly, we repeated all analyses with the multiple imputation of missing data on covariates using a chained equation method. Thirdly, to control the competing risk from other cause mortality, Fine-Gray competing risk models were conducted to analyze overall CVD, CHD, stroke, and cardiovascular mortality, when treating mortality from other causes as a competing risk. Fourthly, considered the effect of diabetes on CVD and mortality risk, we reanalyzed the associations between TyG-related indices and risk of CVD and mortality in those with diabetes at baseline. Fifthly, we additionally adjusted for HbA1c to reduce the potential influence of non-fasting blood glucose [19]. Finally, subgroup analyses were conducted according to baseline age (< 60 vs. ≥ 60 years), sex (female vs. male), and the frequency of drinking (less than twice a week vs. more than twice week a week) to evaluate the susceptible population.
Two-sided P < 0.05 was considered to be statistically significant. All statistical analyses were conducted using R software (version 4.4.0, R Foundation for Statistical Computing).
留言 (0)