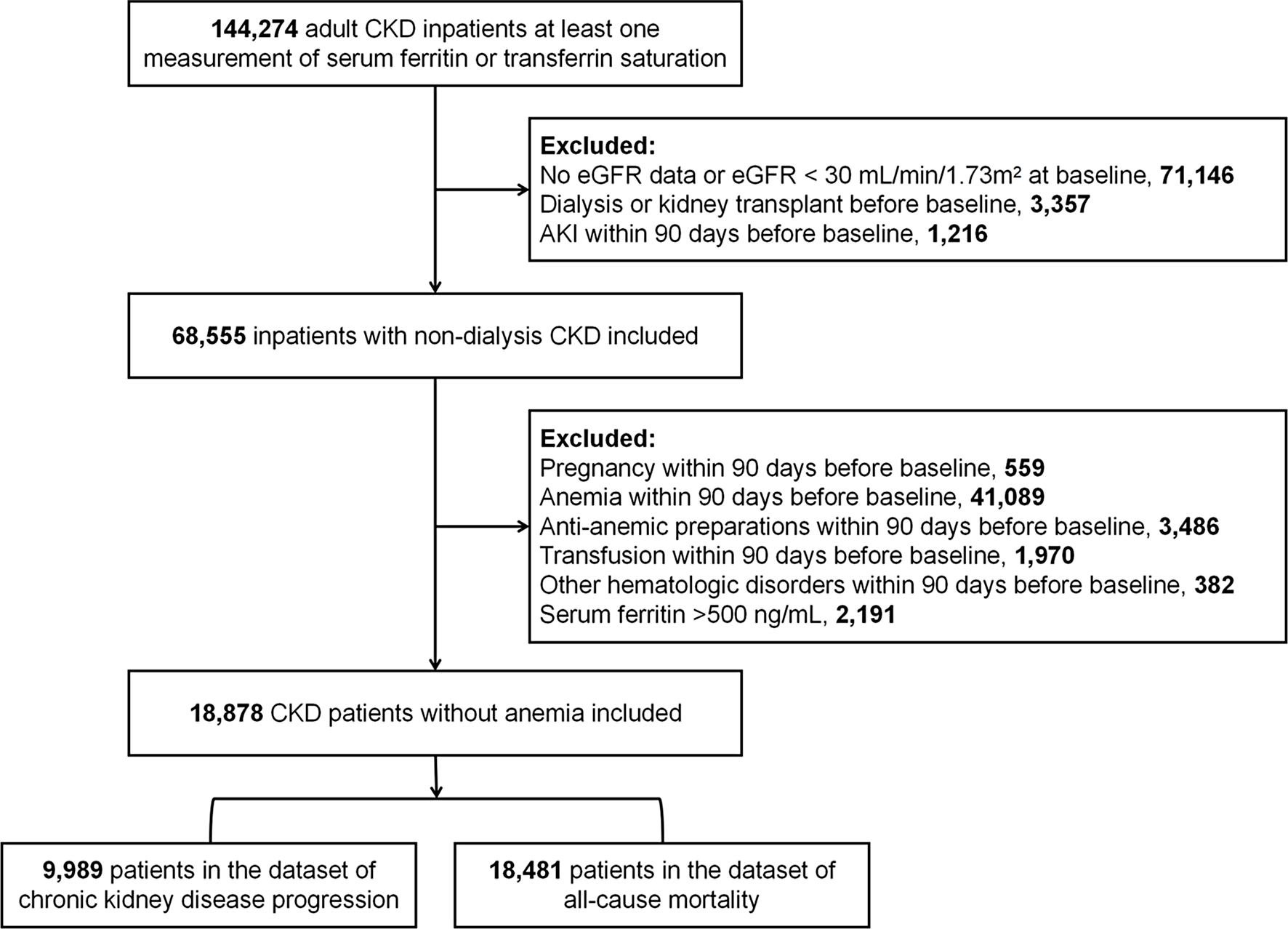
In this large, multicenter, retrospective cohort study, iron deficiency, characterized by decreased level of serum ferritin or TSAT, was prevalent in NDD-CKD patients without anemia. Our findings indicate that in NDD-CKD patients without anemia, lower TSAT level was associated with higher risks of CKD progression and all-cause mortality. However, we found no significant association between serum ferritin and the risk of CKD progression or all-cause mortality.
Iron deficiency is a prevalent issue, affecting approximately 25% of the general population [11, 25] and 30–45% of CKD patients [26]. Previous studies have found that lower TSAT was associated with cardiovascular hospitalizations and mortality in CKD patients [10,11,12,13,14,15, 26,27,28]. However, these studies primarily focused on the association between abnormal iron levels and adverse outcomes in anemic patients. The impact of iron deficiency on CKD progression and all-cause mortality in NDD-CKD subjects without anemia has not been well studied. Moreover, the findings regarding the relationship between iron status and CKD progression were inconsistent [10, 14, 16, 17, 29, 30]. A retrospective study involving 453 veterans with NDD-CKD suggested that higher TSAT levels were associated with higher risk of CKD progression, while lower TSAT or serum ferritin did not show a significant association with CKD progression [9]. In contrast, another observational cohort study including 2,500 patients found a negative correlation between TSAT levels and adverse renal outcomes (renal replacement therapy or a composite of renal replacement therapy plus 50% decline in eGFR) in males and non-anemic patients [17]. These studies were limited by the small sample size and the use of surrogate endpoints. Our large-scale analysis of real-world medical data revealed that lower TSAT level was associated with higher risks of CKD progression and all-cause mortality in NDD-CKD patients without anemia.
The gold standard method for assessing iron stores is the semiquantitative staining of bone marrow iron. However, due to its invasive nature, this test is often not favored in clinical practice. While TSAT and serum ferritin concentration are commonly used tests to diagnose iron deficiency [10], they reflect different aspects of iron status in the body. Serum ferritin assesses the level of storage iron, while transferrin saturation reflects the availability of iron for tissue use [21]. Additionally, serum ferritin levels can be influenced by various pathological conditions such as inflammation, malignancy, and pregnancy [3, 31, 32]. Inflammation can distort interpretation of serum ferritin concentrations, and potentially obscure the diagnosis of iron deficiency [21]. In cases of the functional iron deficiency, characterized by insufficient iron delivery to target tissues and cells, systemic inflammation can enhance the synthesis and secretion of ferritin, resulting in serum ferritin levels that remain within the normal range for many patients [33]. On the other hand, TSAT shows better sensitivity than ferritin in detecting iron deficiency [34]. Our study demonstrated that lower TSAT, rather than ferritin levels, was closely associated with higher risks of renal outcome and all-cause mortality in NDD-CKD patients.
Body iron homeostasis is a delicate balance regulated by various cellular and systemic processes [35]. Iron serves as a co-factor for hemoproteins and non-heme iron-containing proteins, which are essential for a range of enzymatic functions in living organisms [36, 37]. Hemoproteins play crucial roles in essential biological functions such as oxygen binding and transport (hemoglobin), and cellular respiration (cytochromes). Proteins containing non-heme iron are important for fundamental cellular processes such as gene regulation, DNA synthesis, and cell proliferation [37]. Therefore, iron deficiency, whether inherited or acquired, can significantly affect the function of various organs, especially major iron-utilizing and recycling organs. The kidney is actively involved in systemic iron homeostasis as it reabsorbs filtered iron to prevent its excretion in the urine [35]. Furthermore, iron is essential for the high metabolic demands of renal cells, which are rich in mitochondria and actively participate in oxidative reactions [38]. Studies on pregnant rats with prenatal iron deficiency suggest that iron is important for nephrogenesis and physiological renal function [35, 39, 40]. These mechanisms may contribute to increased risks of CKD progression among NDD-CKD patients with iron deficiency without anemia. However, the effects of iron deficiency on the kidney are not fully understood, highlighting the need for further research to clarify the impact of iron deficiency on kidney function.
This study has several strengths. Firstly, it is one of the largest studies to assess the association between iron deficiency and CKD progression as well as all-cause mortality in the NDD-CKD patients without anemia. Secondly, robust kidney outcomes were utilized to analyze the relationship between iron deficiency and CKD progression. For all-cause mortality, information was sourced from the national electronic cause-of-death reporting system of the China Center for Disease Control and Prevention, which has undergone extensive validation [22]. Thirdly, adjustments were made for important potential confounders, such as comorbidities, concomitant medications, CRP levels, and hemoglobin concentration.
Nevertheless, our study has several limitations that must be acknowledged. Firstly, the retrospective and observational design of our study did not allow us to confirm causal relationship between iron deficiency and defined outcomes. Secondly, despite adjusting for numerous key variables in the models, some confounders might remain unadjusted. For example, the impact of inflammation could not be accurately assessed, as some inflammatory markers were not measured in many patients in this study. Thirdly, TSAT measurements were unavailable for the majority of study patients, particularly those without anemia. Consequently, the analysis of the relationship between TSAT levels and the risk of CKD progression was restricted to patients with available TSAT measurements. This limitation may partially affect the generalizability of our findings. However, despite the relatively small sample size, a significant association between TSAT levels and the risk of CKD progression was observed. This underscores the importance of screening TSAT levels in CKD patients, including those without anemia. Fourthly, our reliance on single baseline values of ferritin and TSAT may not have captured the effect of exposure duration, potentially leading to misclassification of the primary exposure due to fluctuations in ferritin and TSAT levels over time. Lastly, the predominantly Chinese sample in our study limits the generalizability of our findings to other ethnic populations.





留言 (0)