Patient selection
Patients aged 18 and over with histologically confirmed non-resectable metastatic colorectal cancer (mCRC) were eligible for inclusion. Patients were required to have received, and experienced progression or unacceptable adverse effects with standard chemotherapies regimens. Previous treatment must have included fluoropyrimidine, irinotecan, oxaliplatin, anti-VEGF monoclonal antibody (not limited to bevacizumab) or anti-EGFR (epidermal growth factor receptor) monoclonal antibody (for patients with RAS wild-type disease). Neoadjuvant or adjuvant chemotherapy was allowed if the disease recurred during treatment or within six months of the last dose. Additionally, MMR, BRAF, and RAS status had to be determined prior to enrolment. Eligible patients were required to have adequate organ function and an Eastern Cooperative Oncology Group (ECOG) performance-status score of 0 or 1. Organ function criteria included an absolute neutrophil count ≥1500 cells/mL, haemoglobin ≥9 g/dL, platelets ≥100,000/mL, creatinine ≤1.5 times the upper limit of normal (ULN) or creatinine clearance >50 mL/minute calculated by the Cockcroft-Gault equation, bilirubin ≤1.5 mg/dL or ≤2.0 ULN in the presence of liver metastases, and alanine transaminases ≤3 times ULN (or ≤5 times ULN in patients with liver metastases). The main exclusion criteria included high microsatellite instability/mismatch repair deficiency, BRAF V600 mutations and brain metastases.
Ethics approval statements
The protocol was approved by the Ethics Committee “Comité de Protection des Personnes Sud-Ouest et Outre-Mer IV on under the 5 May 2022 number 22.00525.000075 and by the ANSM (MEDAECNAT-2022-05-0020 2022-001400-18) in accordance with French Law. The study was registered with ClinicalTrials.gov under the identifier NCT05201352. The study complied with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all patients prior to selection.
Study design
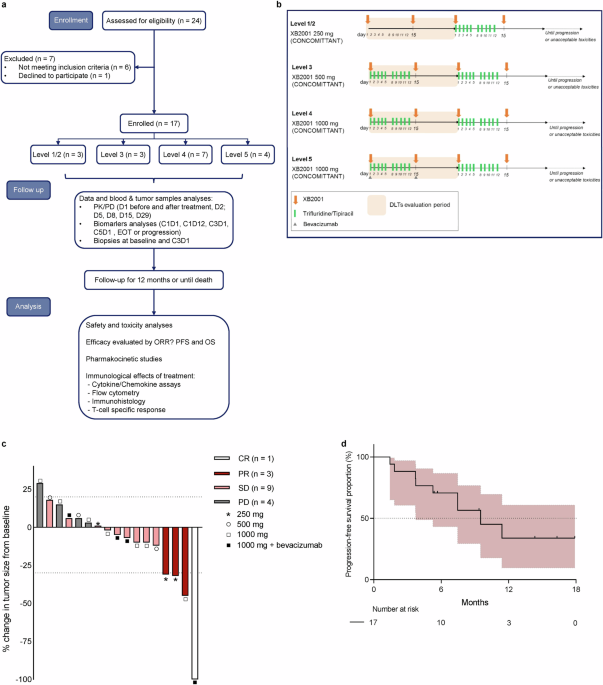
The protocol of this phase I, open label, 3 + 3 dose escalation study has previously been described elsewhere.28 Briefly, the study aimed to evaluate the safety and tolerability and to establish the Maximum Tolerated Dose (MTD) of XB2001 in patients with mCRC receiving FTD/TPI-based chemotherapy (FTD/TPI 35 mg/m² on days 1–5 and 8–12 every 28 days.). Each patient in phase I part of this study was treated until disease progression or the onset of unacceptable toxicities. Three patients were treated at each dose level of XB2001. Level 1/2 involved XB2001 at a 250 mg dose for two doses alone, followed by concomitant administration of FTD/TPI plus XB2001 at the 250 mg dose (3 patients were treated at this level). Level 3 consisted of XB2001 at a 500 mg dose, combined with FTD/TPI (3 patients were treated at this level). Level 4 involved concomitant administration of XB2001 at a dose of 1000 mg plus FTD/TPI, with 6 patients were expected. However, an additional patient was added due to an error in the administration of XB2001, which was given at 500 mg instead of 1000 mg for patient 8, making it impossible to assess the dose-limiting toxicity (DLT) period. Finally, following the approval of concomitant administration of FTD/TPI and bevacizumab as a new standard of care, 4 additional patients were added (level 5) to assess the safety of FTD/TPI plus bevacizumab (5 mg/kg i.v. every 14 days) in combination with XB2001 at the 1000 mg dose. For each dose level, 3 patients were treated, and if there was no dose-limiting toxicities (DLTs) in the first cycle, the protocol moved to the next highest dose. If DLT occurred, a further 3 patients were treated at this dose. If ≥2 patients showed DLT, the dose was considered as not tolerated, and lower doses were studied in subsequent cohorts. At the highest dose, 6 patients were included. The MTD was defined as the highest dose achieved at which no more than one out of six patients developed DLT. The Recommended phase 2 dose (RP2D) was determined on the basis of safety, pharmacokinetics and preliminary efficacy assessments, in patients treated at doses authorized for safety.
Patients were included in the safety analysis if they received at least one dose of XB2001. Safety assessments encompassed physical examinations, laboratory tests, electrocardiograms, and monitoring of adverse events (AEs), which were graded using the NCI Common Terminology Criteria for Adverse Events (version 4.03). Investigators determined the relationship of each AE to the study drug as unrelated, unlikely, possibly, probably, or definitely related. DLTs were defined as grade 4 (G4) haematologic AEs or grade ≥3 non-haematologic AEs that were considered related to the study drug, but not to disease progression, and that did not resolve within 14 days following presentation with standard management. DLTs were evaluated during the first 28 days of treatment.
All patients received prophylactic G-CSF.
Efficacy
CT scan imaging was obtained at screening and every 8 weeks during treatment for the first 12 months of treatment and then every 12 weeks, until end-of-treatment (EOT). Objective response was assessed using RECIST version 1.1 (RECIST v1.1) in patients who received at least one dose of XB2001. Progression-free survival (PFS) is defined as the time from inclusion in the clinical trial to disease progression or death from any cause.
Plasma collection
Blood samples were collected from patients for pharmacokinetics analysis at the following time-points: pre-dose; and days 1, 2, 5, 8, 15, 28 post-dose. Blood samples were also collected from patients for biomarker analysis at the following time-points: Cycle 1 Day 1, Cycle 3 Day 1, Cycle 5 Day 1 and at the end of treatment. After the blood sampling was done at the different times described above, a heparin tube was used to isolate and bank the plasma. For this purpose, after collection, the heparin tube was centrifuged at 1000 g for 10 min at room temperature. The plasma was then recovered, aliquoted at a rate of 1000 µL per cryotube and stored at −80 °C until analysis.
Peripheral blood mononuclear cell isolation
Using the blood samples for biomarker analysis taken on Cycle 1 Day 1, Cycle 3 Day 1, Cycle 5 Day 1 and at the end of treatment, after blood sampling in EDTA tubes, peripheral blood mononuclear cells (PBMC) were isolated from the whole blood by density gradient centrifugation (Lymphocyte Separation Medium, CMSMSL0101, Eurobio) with UNI-SEP tubes (U-16, Eurobio Scientific). Whole blood was transferred into UNI-SEP tubes at a volume of 17 mL per tube and centrifuged at 1000 g for 20 min, with an acceleration setting of 5 and no brake applied. Following the removal of as much plasma as possible, the phase containing enriched PBMCs was recovered. The cells were then washing twice with 45 mL of phosphate-buffered saline (PBS), and centrifuged at 300 g for 10 min. The resulting PBMC pellet was resuspended in 5 mL of PBS 1X for counting. A final wash with 5 mL of PBS 1X was performed before cryopreservation, which involved freezing at a concentration of 10.106 cells per cryotube in a solution containing 50% CS5 Cryostor (C2874, Sigma-Aldrich) and 50% CS10 Cryostor (C2999, Sigma-Aldrich) until further use.
Pharmacokinetic of XB2001
Blood samples were collected from patients for XB2001 pharmacokinetics analysis at the following time-points: pre-dose; and days 1, 2, 5, 8, 15, 28 post dose. Plasma concentrations of XB2001 were determined by ELISA, according to the procedure from XBiotech. Briefly, after coating of the capture antigen on a microplate for at least 1 hour at 37 °C and blocking of the capture antigen with 20% of FBS-TBS buffer for at least 1 hour at room temperature (RT), the standards, controls and samples were prepared and samples were diluted in a 20% FBS-TBS buffer in three independent dilutions (1/100 1/1000, 1/5000) and then transferred to the microplate and incubated at RT for approximately 2 h. After washing the plate 5 times with wash buffer, the secondary antibody mouse anti-human IgG4 Fc-HRP (0.5 mg/ml, Southern Biotech Product, Clone: HP6025) was transferred into the microplate and incubated at RT for approximately 1 h in the dark. Finally, after washing the plate 5 times with wash buffer, TMB substrate (421101, BioLegend) was added into each well and incubated at RT in the dark for 15 min. The reaction was stopped by adding stop solution (423001, BioLegend) to each well of the microplate and after gently vortexing the plate, the absorbance was read at 450 nm.
Non compartmental analysis (NCA) of XB2001 was performed using PKanalix software (MonolixSuite 2023R1, Lixoft, Antony, France) in order to calculate pharmacokinetics parameters, for each individual. The trapezoidal linear method was used to compute the area under the curve from time zero to the time of the last measured concentration (AUC0-last). This method only uses observed data during the first infusion, in order to calculate the slope of the terminal elimination phase and the corresponding terminal half-life (T1/2). In this case, it allows to compute specific pharmacokinetics parameters for intravenous administration, such as the clearance (Cl) and the volume of distribution (Vd). Maximum observed concentration (Cmax) was determined from the observed concentration. AUC0-last was computed rather than AUC0-inf because the percentage of AUC0-inf due to extrapolation from the last time point to infinity was too high (>20). Default software settings were used unless otherwise stated.
Anti-product response analysis
The anti-product response to XB2001 was assessed by ELISA assay according to XBiotech’s procedure and carried out at the following sample times: pre-dose; and days 1, 2, 5, 8, 15, 28, 56, 112 post dose. Briefly, a dilution of the capture antibody (XB2001) or coating buffer alone were added on each well of the microplates and plates were incubated at 37 °C for 1 h. After blocking and washing of microplates, plasma samples were diluted 1/500 with 20% of FBS-TBS solution and then were added in each well (coated or non-coated with Natrunix) and incubated at RT for 2 h. During incubation, the dilution of each secondary antibody (mouse anti-human IgG2 Fc-HRP conjugated (9060-05, Southern Biotech, Clone: 31-7-4), mouse anti-human IgG3 (hinge region specific)-HRP conjugated (9230-05, Southern Biotech, Clone: SB81a), mouse anti-human IgG1 (Fc specific)-HRP conjugated (9054-05, Southern Biotech, Clone: HP6001), goat anti-human IgA (a-chain specific)-HRP conjugated (2050-05, Southern Biotech), mouse anti-human IgM (μ-chain specific)-HRP conjugated (9040-05, Southern Biotech, Clone: JDC-10)) was prepared in 20% FBS-TBS buffer. After washing the microplates, the different secondary antibodies were added to each well of interest in microplates coated and non-coated with XB2001 and were incubated at RT in the dark for 1 h. After washing the microplates, TMB substrate was added into each well and incubated at RT in the dark for 15 min. The reaction was stopped by adding stop solution to each well of the microplate and after gently vortexing the plate, the absorbance was read at 450 nm.
Pharmacodynamics: The following sampling times were analysed: pre-dose, and days 5 and 28 post dose. Plasma IL-6 concentrations were determined using ELISA, following the manufacturer’s guidelines (Biolegend, 430517).
Histology
Biopsies were obtained either prior to study entry using archival materials less than 2 years old or at baseline as fresh samples. Fresh biopsies were fixed in PFA immediately after collection and embedded in paraffin by the pathology laboratory. Four-micron slices were prepared from FFPE tumour samples using a Tissue-Tek Autosection microtome (Sakura). Slide staining was performedon an Autostainer 48 (Agilent) using primary antibodies against IL1α primary antibody (clone BSB-138, Diagomics) or CD3 (clone F7.2.38, Agilent). Slides were deparaffinized in a pH9 buffer at 95 °C for 25 min, then cooling and washed twice in wash buffer (Agilent) for 5 min each. Peroxydase activity was blocked with peroxydase blocking reagent (SM801, Agilent). Anti-human CD3 or anti-human IL1α antibodies were applied for 30 min (CD3) or 60 min (IL1α) at room temperature. After two washes, EnVision FLEX HRP polymers (SM802, Agilent) were added for 20 min (CD3) or 30 min (IL1α) at room temperature. DAB (SM803, Agilent) was applied for 5 min (CD3) or 10 min (IL1α), followed by two washes. Finally, slides were stained with hematoxylin (SM806, Agilent) for 5 min and mounted using a Leica automated coverslipper. The slides were then digitalised at x20 magnification using a VS200 scanner (Olympus) to generate whole slide imaging (WSI) files in vsi format. The analysis was performed with QuPath software (v.5.1), and ROIs were selected on each slide.
For CD3 analysis, the number of positive cells was counted in each area and the average was determined. IL-1α staining was evaluated independently by two pathologists and split into three groups, namely IL-1α negative, IL-1α low and IL-1α high.
The immunoscore for CD8/PDL1 was assessed by measuring the densities of PD-L1+ and CD8+ cells and evaluating their spatial proximity within a single tissue section. Immunohistochemistry was performed using anti-PD-L1 (QR1), anti-CD8 (C8/114B) antibodies, followed by hematoxylin counterstaining. PD-L1 and CD8 antibodies were visualized using DAB and Magenta-HRP, respectively. All stained slides were digitized at 20x magnification using a high-resolution scanner (VS200, Olympus). The resulting whole-slide images were analysed using QuPath software.
Bioplex assay
Forty-five analytes were quantified in plasma at two timepoints: Cycle 1 Day 1 and Cycle 3 Day 1, using the Human XL Cytokine Magnetic 45-plex Luminex® assay (#898855, R&D Systems, USA) according to the manufacturer’s protocol. These analytes included: C-C motif chemokine ligand (CCL)2, 3, 4, 5, 11, 19, and 20, CD40 ligand, fractalkine, C-X-C motif chemokine ligand (CXCL) 1, 2, and 10, epidermal growth factor (EGF), fibroblast growth factor (FGF), FMS-like tyrosine kinase 3 ligand (FLT3L), granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), granzyme B, interferon (IFN)-α, -β, -γ, interleukin (IL)-1α, 1β, 1RA, 2, 3, 4, 5, 6, 7, 8, 10, 12, 13, 15, 17A, 17E, and 33, programmed death-ligand 1 (PD-L1), platelet-derived growth factor (PDGF)-AA and AB/BB, transforming growth factor (TGF)-α, tumour necrosis factor (TNF)-α, TNF-related apoptosis inducing ligand (TRAIL), and vascular endothelial growth factor (VEGF). The standard performance values for each analyte are provided in Supplementary Table 7.
Immune cells analysis
We performed immunophenotyping by flow cytometry on PBMCs from Cycle 1 Day 1 and Cycle 3 Day 1.
Blood count analysis
Antibodies used: Multicolour flow cytometry was performed using custom-designed tubes from Beckman Coulter incorporating dry coating technology with the following antibodies: anti-CD16-FITC (clone 3G8), anti-CD56-PE (clone N901), anti-CD25-ECD (clone B1.49.9), anti-HLA-DR-PE-Cy5.5 (clone Immu-357), anti-CD14-PE-Cy7 (clone RMO52), anti-CD4-APC (clone 13B8.2), anti-CD8-AlexaFluor700 (Clone B9.11), anti-CD3-APC-AlexaFluor750 (clone UCTH1), anti-CD15-PacificBlue (clone 80H5) and anti-CD45-KromeOrange (clone J.33). Liquid antibodies were also used: anti-CD127-BV605 (BioLegend, clone A019D5), anti-CCR7-BV650 (BioLegend, clone G043H7) and anti-CD45RA-BV785 (BioLegend, clone HI100).
Staining protocol: After thawing and counting, 1.106 of PBMCs were added to DURAClone tubes containing liquid antibodies, vortexed for 15 s and incubated at room temperature in the dark for 15 min. Next, 2 mL of red blood lysis solution (VersaLyse solution, A09777, Beckman Coulter) mixed with 50 μL of IOTest 3 Fixative solution (A07800, Beckman Coulter) was added, inverted and incubated for an additional 15 min in the dark. Following incubation, the cells were centrifuged at 1000 rpm for 5 min. The pellet was washed with 2 mL PBS, centrifuged again at 1000 rpm for 5 min and resuspended in 150 µL PBS. Finally, cell acquisition was performed on a DxFLEX cytometer (Beckman Coulter).
Data analysis
FCS files were analysed by commercial software Kaluza (Beckman Coulter) and Omiq (Omiq, Inc.).
Manual gating: After checking and validating the compensations for each FCS file in Kaluza software (Beckman Coulter), live singlet CD45+ cells were exported for analysis on a pipeline implemented in Omiq.
High-dimensional data analysis was performed on 31 samples (n = 16 samples at Cycle 1 Day 1 and n = 15 samples at Cycle 3 Day 1) and 5 000 cells per sample were included (total n = 155,000 CD45+ immune cells).
Uniform Manifold Approximation and Projection (UMAP) analysis: Visualization of the global single-cell landscape was performed using UMAP in Omiq based on channels CD16, CD56, CD25, HLA-DR, CD14, CD4, CD8, CD3, CD127, CCR7 and CD45RA, random seed 4478, epochs 200, learning rate 1, neighbours 75 and minimum distance 0,4. Then ClusterX was performed based on the umap-1 and umap-2 features, and by using a Gaussian Kernel with an alpha coefficient of 0.001.
T cell specific immune response
Circulating tumour-specific T cell responses were evaluated using an IFN-γ ELISPOT assay after short-term in vitro stimulation of PBMCs. Cells were stimulated with a mixture of eight TERT-derived major histocompatibility complex class II‒binding peptides (a pool of HLA-DR and HLA-DP-restricted TERT peptides29,30) and NY-ESO1 peptides at a concentration of 5 μg/mL for six days, as previously described.29,31 All synthetic peptides (>90% purity) were obtained from JPT (Germany). To asses antiviral recall responses, a peptide mixture referred to as CEF – comprising peptides from influenza virus (Flu), Epstein–Barr virus, cytomegalovirus (Cellular Technology Ltd) was used. Frozen PBMCs were thawed and cultured with tumour-derived peptides (5 µg/ml) in RPMI supplemented with 5% fetal bovine serum in 24-well plates (4 × 106 cells per well). IL-7 (5 ng/mL, 200-07, PeproTech) and IL-2 (20 UI/mL, 202-IL-010, Novartis) were added on days 1 and 3, respectively. On day 7, the antigen-specific T cells was quantified using the IFN-γ ELISpot assay following the manufacturer’s instructions (hIFNgp-2M/5, Human IFN-γ Single-Color ELISPOT Precoated 96 wells Strip, ImmunoSpot). Briefly, lymphocytes from the in vitro stimulation (105 cells per well) were incubated for 24 h at 37 °C in ELISpot plates precoated with anti-human IFN-γ antibodies, in the presence or absence of peptide mixtures, using CTL-Test™ PLUS Medium (CTLTP-010, ImmunoSpot). Controls included cells cultured with medium alone (negative control) and phorbol 12-myristate 13-acetate (1 ng/mL; P8139, Sigma-Aldrich)/ionomycin (10 mmol/L; I3909, Sigma-Aldrich) as positive control. IFN-γ spots were revealed as per the manufacturer’s protocol (Immunospot, CTL, Germany). The number of specific T cells, expressed as ΔIFN-γ spots per 105 cells, was calculated by subtracting the background value (medium control). Spot-forming cells were quantified using the C.T.L. Immunospot system (Cellular Technology Ltd). Responses were deemed positive if the number of IFN-γ spots exceeded 10 and was at least twice the background level.32
Correlative studies
We examined correlations in immunohistological analysis with analysis of IL1α expression, CD3 content and Immunoscore IC, serum analysis with assessment of cytokine changes using bioplex assay, evolution of immune cell numbers in blood using multiparametric flow cytometry and study of telomerase-specific T-cell response using ELISPOT.
Statistical analysis
Patient characteristics and AEs were summarized using descriptive statistics. The safety analysis included all enroled patients who received at least one dose of XB2001, while efficacy and biomarker analyses included patients who completed at least one treatment cycle. Comparisons of patient characteristics were conducted using the Mann–Whitney unpaired test for continuous variables, as applicable. The prognostic value of variables for PFS was assessed using univariate Cox regression models. Continuous variables were dichotomized based on either the median cut-off or the methodology proposed by Lausen et al.33, utilizing the maxstat R library. Survival probabilities were estimated using the Kaplan–Meier method, and survival curves were compared with the log-rank test. All statistical analyses were performed using R software (version 4.2.3) and GraphPad Prism (version 10.0.02). A p-value < 0.05 was considered statistically significant.



留言 (0)